Passage of Gangrenous Small Bowel Per Rectum Following Superior Mesenteric Vessel Thrombosis
Meenakshi Eknath Yeola (Pate)1, Aditya Prabhalkarrao Borgaonkar2
1 Professor and Head, Department of General Surgery, JNMC, Sawangi Meghe, Wardha, Maharashtra, India.
2 Postgraduate Student, Department of General Surgery, JNMC, Sawangi Meghe, Wardha, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Aditya Prabhalkarrao Borgaonkar, Department of Surgery, JNMC, DMIMS (DU), Sawangi Meghe, Wardha, Maharashtra, India.
E-mail: adityaRSML08@gmail.com
Mesenteric venous thrombosis is a rare cause of chronic pain in abdomen. Only in few cases with abdominal pain, bowel infarct has been reported. This report is that of a 42-year-old male with a history of chronic alcoholism, presented with continuous dull pain in abdomen for 1 year and vomiting for 1 month, typically after ingestion of food. At the time of admission, his vitals were stable. On examination of abdomen, the only finding was tenderness in left hypochondriac and left lumbar region without guarding or rigidity. His erect abdomen radiograph suggested no evidence of intestinal perforation or obstruction. Ultrasonography of abdomen suggested bowel loops with normal peristalsis, no evidence of any dilatation or oedema of wall or of free fluid in peritoneal cavity. CT angiography of abdomen was suggestive of Superior Mesenteric Artery (SMA) thrombosis. While on conservative management he passed almost 2 feet small bowel per rectum. Emergency diagnostic laparoscopy showed faecal matter in left paracolic gutter. Exploratory laparotomy was done and jejuno-ileal resection and anastomosis were done.
Acute abdomen, Mesenteric ischaemia, Mesenteric vessels thrombosis, Small bowel gangrene
Case Report
A 42-year-old male, complained of pain in abdomen for one year. Pain was insidious in onset, dull aching type, continuous, in left lumbar region, non-radiating, no aggravating or relieving factors. Vomiting episodes typically followed ingestion of food.
He gave history of vomiting for 1 month with loss of appetite and weight. Patient was a chronic alcoholic. He was admitted to several hospitals in last one year for same complaints. Angiography revealed superior mesenteric artery thrombosis and he was managed conservatively, without relief of his pain.
At the time of presentation, he was afebrile with heart rate 88 Beats/minute, Blood pressure 110/70 mmHg and Respiratory rate 20/minute. His abdomen was scaphoid with normally inverted umbilicus; without distension, visible peristalsis or dilated veins. There was mild tenderness in left lumbar, left hypochondriac regions without guarding or rigidity. Bowel sounds were heard.
Liver and kidney function tests were normal with PT-INR 1.16 seconds. CBC-WBC:10300/mL, Platelets: 474000/mL. Ultrasonography (USG) abdomen and pelvis suggested bowel loops with normal peristalsis with no evidence of any dilatation or oedema of wall or free fluid in peritoneal cavity. Normal flow in portal vein at porta and confluence was seen.
Contrast Enhanced Computed Tomography (CECT) abdomen and pelvis reports revealed chronic thrombotic occlusion of coeliac axis artery from its origin along superior mesenteric artery just distal to its origin, multiple mesenteric collaterals, partial hepatic artery thrombosis with recanalization. Suprarenal abdominal aortic segment appears irregular with plaque and relative narrowing, dominant inferior mesenteric artery circulation. Central filling defects involving mesenteric veins and extending to portal vein confluence suggestive of mesenteric venous thrombosis. Oedematous enhancing segmental bowel (ileum), splenic and liver infarcts.
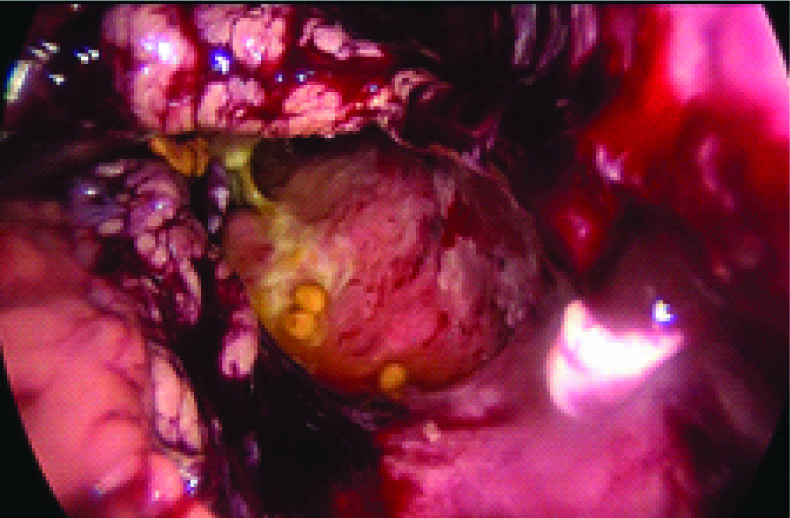
With patient being vitally stable and no abnormality on laboratory workup, he was planned for conservative management, but when one evening he passed a portion of his small bowel per rectum [Table/Fig-1], an emergent diagnostic laparoscopy was done under general anaesthesia which showed adhesions in bowel loops in epigastrium, left hypochondrium, left lumbar regions and presence of faecal matter in left paracolic gutter [Table/Fig-2].
The specimen shed per rectally.

Diagnostic laparoscopy showing faecal matter in right paracolic gutter.
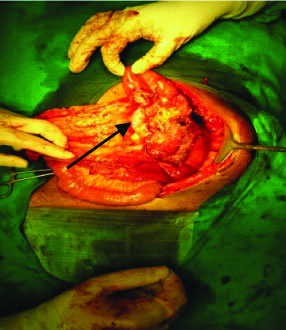
Exploratory laparotomy was mandatory which revealed dense adhesions in jejunum and descending colon with presence of concealed transection of jejunum at 20-25 cm distal to Duodenojejunal (D-J) flexure [Table/Fig-3]. Adhesions were separated. Jejuno-ileal resection and anastomosis were done [Table/Fig-4].
Concealed complete transection of small intestine.

Patient had an uneventful post-operative period and was asymptomatic during follow-up visits.
Discussion
Despite recent advances and research in the medical field, acute thromboembolism of superior mesenteric artery still carries poor prognosis [1,2] with arterial thrombosis having poorer prognosis than venous [3,4], this is attributed to rather nonspecific signs and symptoms that characterise acute mesenteric ischaemia [5,6]. In the early stage of ischaemia, abdomen remains soft and non tender with pain out of proportion to physical examination findings [7,8].
Romano N et al., reported a case of 39-year-old female that developed small bowel infarct due to SMA thrombosis [9]. Raherinantenaina F et al., reported a case of 35-year-old male having paroxysmal pain in epigastrium and bloody diarrhoea for 13 days with patient being stable haemodynamically [10]. Segmental ischaemia was found at 10 cm from ileo-caecal junction. Resection and anastomosis were done.
However, the index case presented with complete concealed transection of ileum with passing of 2 feet of small bowel per rectally making it a unique presentation.
Conclusion
Though acute mesenteric ischaemia due to Superior Mesenteric Artery (SMA) thrombosis is a rare cause of presentation of acute abdomen, it should be considered in all cases where there are non-specific signs and symptoms accompanying the acute abdomen as presented in this case, clinicians should be prepared for unexpected surprises that nature and human body present in harmless looking cases.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 12, 2019
Manual Googling: Nov 15, 2019
iThenticate Software: Nov 29, 2019 (12%)
[1]. Björck M, Acosta S, Lindberg F, Troëng T, Bergqvist D, Revascularization of the superior mesenteric artery after acute thromboembolic occlusionBritish Journal of Surgery 2002 89(7):923-27.10.1046/j.1365-2168.2002.02150.x12081744 [Google Scholar] [CrossRef] [PubMed]
[2]. Schoots IG, Koffeman GI, Legemate DA, Levi M, Van Gulik TM, Systematic review of survival after acute mesenteric ischaemia according to disease aetiologyBritish Journal of Surgery 2004 91(1):17-27.10.1002/bjs.445914716789 [Google Scholar] [CrossRef] [PubMed]
[3]. Yasuhara H, Acute mesenteric ischemia: the challenge of gastroenterologySurgery Today 2005 35(3):185-95.10.1007/s00595-004-2924-015772787 [Google Scholar] [CrossRef] [PubMed]
[4]. Oldenburg WA, Lau LL, Rodenberg TJ, Edmonds HJ, Burger CD, Acute mesenteric ischemia: a clinical reviewArchives of Internal Medicine 2004 164(10):1054-62.10.1001/archinte.164.10.105415159262 [Google Scholar] [CrossRef] [PubMed]
[5]. Kurland B, Brandt LJ, Delany HM, Diagnostic tests for intestinal ischemiaSurgical Clinics of North America 1992 72(1):85-105.10.1016/S0039-6109(16)45629-X [Google Scholar] [CrossRef]
[6]. Sachs SM, Morton JH, Schwartz SI, Acute mesenteric ischemiaSurgery 1982 92(4):646-53. [Google Scholar]
[7]. Kozuch PL, Brandt LJ, diagnosis and management of mesenteric ischaemia with an emphasis on pharmacotherapyAlimentary Pharmacology and Therapeutics 2005 21(3):201-15.10.1111/j.1365-2036.2005.02269.x15691294 [Google Scholar] [CrossRef] [PubMed]
[8]. Hariharan M, Balasubramaniam R, Shetty SK, Yadavalli S, Ahetasham M, Devarapalli S, Uncommon causes of acute abdominal pain–A pictorial essayJournal of Clinical Imaging Science 2016 6:410.4103/2156-7514.17754827014500 [Google Scholar] [CrossRef] [PubMed]
[9]. Romano N, Prosperi V, Basili G, Lorenzetti L, Gentile V, Luceretti R, Acute thrombosis of the superior mesenteric artery in a 39-year-old woman with protein-S deficiency: a case reportJournal of Medical Case Reports 2011 5(1):1710.1186/1752-1947-5-1721244677 [Google Scholar] [CrossRef] [PubMed]
[10]. Raherinantenaina F, Rakotondrazafy TF, Ratsimba HR, Rajaonanahary TM, Acute intestinal ischemia complicating mesenteric venous thrombosisJournal of Visceral Surgery 2019 pii:S1878-7886(19)30131-3610.1016/j.jviscsurg.2019.08.00631471177 [Google Scholar] [CrossRef] [PubMed]