Fabrication of Hollow Complete Denture with Althaea- A Case Report
KV Anitha1, Gopi Naveen Chander2, Srividya Devi3, Sanjana Tharakan4
1 Reader, Department of Prosthodontics, SRM Dental College, Ramapuram, Chennai, Tamil Nadu, India.
2 Professor, Department of Prosthodontics, SRM Dental College, Ramapuram, Chennai, Tamil Nadu, India.
3 Postgraduate student, Department of Prosthodontics, SRM Dental College, Ramapuram, Chennai, Tamil Nadu, India.
4 Postgraduate student, Department of Prosthodontics, SRM Dental College, Ramapuram, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: KV Anitha, 76/110, F-1, Chakra Enclave, Bajanai Koil Street, Choolaimedu, Chennai-600089, Tamil Nadu, India.
E-mail: dranikv@yahoo.co.uk
Rehabilitation of extremely resorbed residual ridges present a threat to dental clinicians. Fabrication of dentures with excessive inter-ridge distance makes the prosthesis heavy. Fabricating light weight dentures is important to reduce the discomfort of patient. Several methods have been tried and till now there is no definitive and simple way to fabricate hollow removable dental prosthesis. This case report describes a new variant method for fabrication of hollow complete denture with edible Althaea candy. Althaea officinalis L is scientific name for marsh-mallow perennial plant with each part having health benefits. Roots are powdered and mixed with sugar and egg white to make it edible as candy. These candies were used as index spacers for hollowing removable dentures. Patient comfort, mastication and phonetics are improved with wearing of light weight dental prosthesis.
Edible candies, Light weight, Removable dental prosthesis
Case Report
A 64-year-old female patient reported to the Department of Prosthodontics for replacement of her previous complete denture with primary complaint of heaviness in the dentures. She had been wearing this denture with discomfort for the past 4 years. She had difficulty in mastication and phonetics.
The patient was diabetic and her intra-oral examination showed extremely resorbed ridges in both maxillary and mandibular arch. No evident pathological findings were detected in the oral cavity. A complete evaluation of the previous denture was done and deemed to be satisfactory except for the overweight of the prosthesis. The weight of the old conventional prosthesis was measured using a digital gauge and was estimated to be 37.23 gm for maxillary denture and 31.47 gm for mandibular denture. With exactness of chief complaint, rendering hollow dental prosthesis was decided for the patient.
Denture Fabrication Technique
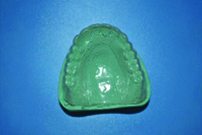
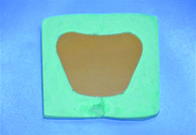
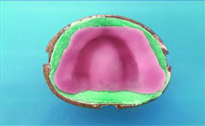
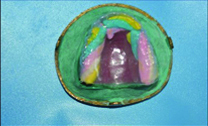
Preliminary impression was made with mucostatic irreversible hydrocolloid material (Zelgan; Dentsply). A selective pressure impression technique was adopted for making the secondary impression with zinc oxide eugenol impression paste (DPI; Dental Products of India). After secondary impression, the master cast was duplicated with silicone duplication material (DoubleTakeR; Ivoclar Vivadent) to fabricate heat cure denture base [Table/Fig-1]. The heat cured denture base was fabricated using conventional compression molding technique with heat activated poly-methyl methacrylate material (DPI Heat Cure; Dental Products of India). After try-in completion, the waxed up denture was duplicated to make a clear template with 0.3 mm thermoplastic resin sheet (BiostarR transparent, India) in order to gauge the amount of hollow space created in the denture [Table/Fig-2]. Conventional denture processing method with compression molding technique was adhered for making the prosthesis. The master cast with waxed up denture was invested using artificial stone (Ultra Stone; Kalabhai Karson Pvt., Ltd.,). Regular dewaxing was done to remove all wax components [Table/Fig-3]. To obtain a uniform heat cure resin sheet of 2 mm thickness, a stone mold method with double thickness of shellac baseplate (Pyrax Base Plate; Pyrax Polymars) into a mix of dental stone (Ultra stone; Kalabhai Karson Pvt., Ltd.,) was followed [Table/Fig-4,5]. Once the mold was prepared, the mix of heat cure poly methyl methacrylate resin (DPI Heat Cure; Dental Products of India) polymer and monomer was proportioned according to manufacturer’s recommendation. Separating medium (DPI Heat Cure Cold Mould Seal, Dental Products of India) was applied into stone mold before placing the resin dough into it. A cellophane sheet was used to carry the dough into the mold, and a roller pin was used to get a uniform sheet thickness of 2 mm. The excess material was cut with a sharp Bard-Parker blade No. 15 (Surgeon; Kehr Surgical Pvt., Ltd.,) [Table/Fig-6]. The resin sheet was now adapted onto the body of the flask where the denture teeth are embedded in the mold [Table/Fig-7]. Althaea candies (Haribo Pink Chamallows; Godrej Nature’s Basket) were packed in the clear resin template and was placed over the adapted resin sheet [Table/Fig-8]. The amount of hollow space created was evaluated with an endodontic file and a rubber stopper [Table/Fig-9]. Depending upon the shape and size of Althaea, as many candies as possible were packed until the mold was completely filled. The resin template was removed and components of flask were approximated and secured with clamp. The denture processing was done in a conventional method. The packed candies disappeared during curing cycle to create a hollow cavity within the confines of the prosthesis. Finished and polished hollow complete denture was delivered to the patient.
Silicone duplicated mold of master cast.

Duplicated master cast with clear resin template.

Stone mold to get resin sheet.

Two shellac baseplates placed into mold.
Resin sheet of uniform 2 mm thickness.

Resin sheet adapted into body of flask.
Marshmallows packed into the mold.
Evaluation of hollow space with endodontic file.

Patient’s subjective satisfaction was verified by instructing to feel the light weight of the new made prosthesis. An objective evaluation of the weight of the prosthesis was done with a digital weighing balance to confirm the weight of the denture. The weight of the prosthesis determined with a digital weighing machine (Kerro BL5002; Mxrady lab Solutions Pvt., Ltd.,) showed that it was only 17.42 gm for maxillary denture and 16.34 gm for mandibular denture. Periodic review was conducted to affirm the improvement in patient comfort, mastication and speech with this hollow complete denture [Table/Fig-10].
Postoperative intraoral denture placement.

Discussion
Edentulous condition is a common clinical phenomenon affecting geriatric population and denture wearing patients present with varied complaints because of their lack of adaptation to the artificial prosthesis. There is a compromise in their quality of life if the mastication, phonetics and aesthetics are not restored to near normalcy. The situation becomes severe when there is excessive Residual alveolar Ridge Resorption [RRR] and a long waiting period of edentulism without rehabilitation. Studies done by Huumonen S et al., have inferred that individuals with severe RRR represent more subjective complaints in the form of difficulty in wearing dentures, difficulty in eating or speaking and low denture stability [1,2]. Management of extreme RRR with fabrication of light weight prosthesis improves the patient satisfaction.
Several attempts have been made to make the prosthesis light weight by creating hollowness by use of solid spacers like dental stone, cellophane covered asbestos, silicone putty, modelling clay, gauze roll with light body silicone, thermocol [3-6]. Different processing techniques for the same have also been tried with single-flask and double-flask method. In double-flask technique, intaglio surface is prepared in one half and occlusal and polished surfaces in other half. Later these two halves are joined with self-cure acrylic resin. All these procedures require escape holes or space to be created for removal of packed material after processing of denture. Self-cure poly methyl methacrylate is then used for closing the hole [7].
In this clinical report, marshmallows which has never been used prior in dentistry was employed to create hollow cavity within denture. It was chosen because of several advantages when compared to previous specified techniques for hollow denture fabrication. When marshmallows are used, a single flasking method can be employed and there is no need for interchange of components of flask while processing the final denture. A uniform resin sheet thickness was obtained with stone mold technique. In all the previous techniques removal of packed spacer material was difficult. This may result in incomplete retrieval of packed material or needs additional procedure to evacuate the spacer to create hollowness [4]. Once they are removed, a tight seal has to be made with self-cure acrylic resin. If the hole made is large then, obtaining an intact seal is a problem. Issues like leakage and color difference becomes distinct [7]. Difficulties aforementioned were overcome by the use of marshmallows as spacer material.
In the previous literature by Bhushan P et al., caramel was used as spacer material for creating hollow dentures. But it had a limitations that caramel could get contaminated with water while denture packing and solid caramel had a tendency to break while handling [8]. A search for an alternative material to overcome the limitations of caramel, thumped up with marshmallows. Scientific name for marshmallows is Althaea officinalis L, are edible candies made from sugar, water and gelatin or egg whites (albumen). They are basically sugar solution to which gelatin or egg whites are added as protein stabilising agents to prevent air from escaping, thus acting as an aerator [9]. Physical properties of this material make it more suitable for making the hollow denture. They are fundamentally a foam like material prepared as a confectionary and filled up with 50% air. Gelatin is the most commonly used aerator in manufacturing of Althaea candies. It forms a network between water molecules and air bubbles. Its melting point is 35°C much less than curing temperature, indicating that melting of marshmallow was possible during curing procedure. As the candy consists of 50% air, it is clear that particles in it have more empty space and freedom of movement, thereby an increased level of kinetic energy to evacuate when subjected to increase in temperature. Packing with Althaea candy spacer was easy as it is only puffed with air in it. With increase in temperature, the gas molecules expand and increase the puffiness of marshmallows. But as the air bubbles grow in size, they rupture [10]. At the same time water molecules evaporate creating a hollowness inside the denture. There is a change of state from solid to liquid to gas in Althaea as thermal energy is increased. Processed dentures also have a pleasant flavor which emanate from the melted marshmallows [11,12]. Unlike caramel spacer, the candies are soft solids and not hard, so brittleness was not a problem while handling. Approximately, a 20-25 gm reduction in weight of the prosthesis was appreciated when compared to conventional complete dentures.
Conclusion
An effective management of edentulous patient with primary complaint of heaviness in the prosthesis is elucidated. Commercially available Althaea candies are used as first of its kind to create hollow cavity within the confines of the denture. The laboratory step of making escape holes for retrieval of spacer material is eliminated when dentures are fabricated using this technique. Physical properties and handling characteristics of this material make it practically suitable for fabricating hollow dentures.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 28, 2019
Manual Googling: Nov 07, 2019
iThenticate Software: Nov 19, 2019 (9%)
[1]. Huumonen S, Haikola B, Oikarinen K, Söderholm AL, Remes-Lyly T, Sipilä K, Residual ridge resorption, lower denture stability and subjective complaints among edentulous individualsJ Oral Rehabil 2012 39:384-90.10.1111/j.1365-2842.2011.02284.x22289034 [Google Scholar] [CrossRef] [PubMed]
[2]. Haikola B, Oikarinen K, Söderholm AL, Remes-Lyly T, Sipilä K, Prevalence of edentulousness and related factors among elderly FinnsJ Oral Rehabil 2008 35:827-35.10.1111/j.1365-2842.2008.01873.x18482342 [Google Scholar] [CrossRef] [PubMed]
[3]. Deogade SC, Patel A, Mantri SS, An alternative technique for hollowing maxillary complete dentureJ Indian Prosthodont Soc 2016 16:412-15.10.4103/0972-4052.19128527746610 [Google Scholar] [CrossRef] [PubMed]
[4]. Brown KE, Fabrication of a hollow-bulb obturatorJ Prosthet Dent 1969 21:97-103.10.1016/0022-3913(69)90035-3 [Google Scholar] [CrossRef]
[5]. Fattore LD, Fine L, Edmonds DC, The hollow denture: an alternative treatment for atrophic maxillaeJ Prosthet Dent 1988 59:514-16.10.1016/0022-3913(88)90053-4 [Google Scholar] [CrossRef]
[6]. Worley JL, Kniejski ME, A method for controlling the thickness of hollow obturator prosthesesJ Prosthet Dent 1983 50:227-29.10.1016/0022-3913(83)90022-7 [Google Scholar] [CrossRef]
[7]. Elliott DJ, The hollow bulb obturator: its fabrication using one denture flaskQuintessence Dent Technol 1983 7:13-14. [Google Scholar]
[8]. Bhushan P, Aras MA, Chitre V, Mysore AR, Mascarenhas K, Kumar S, The hollow maxillary complete denture: A simple, precise, single-flask technique using a caramel spacerJ Prosthodont 2019 28(1):e13-17.10.1111/jopr.1261628383131 [Google Scholar] [CrossRef] [PubMed]
[9]. Pakrokh Ghavi P, The extraction process optimization of antioxidant polysaccharides from Marshmallow (Althaea officinalis L.) rootsInt J Biol Macromol 2015 75:51-57.10.1016/j.ijbiomac.2014.11.04725603144 [Google Scholar] [CrossRef] [PubMed]
[10]. Yuan X, Carter BP, Schmidt SJ, Determining the critical relative humidity at which the glassy to rubbery transition occurs in polydextrose using an automatic water vapor sorption instrumentJ Food Sci 2011 76:E78-89.10.1111/j.1750-3841.2010.01884.x21535679 [Google Scholar] [CrossRef] [PubMed]
[11]. Ergun R, Lietha R, Hartel RW, Moisture and shelf life in sugar confectionsCrit Rev Food Sci Nutr 2010 50:162-92.10.1080/1040839080224883320112158 [Google Scholar] [CrossRef] [PubMed]
[12]. Richard W Hartel, Annakate Hartel, Candy Bites: The Science of Sweets 2014 New YorkCopernicus:199-202.10.1007/978-1-4614-9383-9_50 [Google Scholar] [CrossRef]