Milky Colour Ascitic Fluid in Idiopathic Nephrotic Syndrome: Pseudochylous Ascites
Parveen Kumar Antil1, Bablu Kumar Gaur2, Meenakshi Dadwal3, Baljeet Maini4
1 Junior Resident, Department of Paediatrics, Maharishi Markandeshwar Institute of Medical Sciences and Research, MMU (Deemed to be University), Ambala, Haryana, India.
2 Associate Professor, Department of Paediatrics, Teerthankar Mahaveer Medical College and Research Centre, TMU, Moradabad, Uttar Pradesh, India.
3 Junior Resident, Department of Paediatrics, Maharishi Markandeshwar Institute of Medical Sciences and Research, MMU (Deemed to be University), Ambala, Haryana, India.
4 Professor, Department of Paediatrics, Teerthankar Mahaveer Medical College and Research Centre, TMU, Moradabad, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Bablu Kumar Gaur, A-110, Parshawnath Pritibha Apartment, Delhi Road, Moradabad, Uttar Pradesh, India.
E-mail: drbkgaur@gmail.com
In normal conditions, ascitic fluid is clear to pale yellow. The causes of milky colour ascitic fluid in children includes spontaneous bacterial peritonitis, chylous ascites and pseudochylous ascites. Pseudochylous ascites is an uncommon clinical entity in children. Nephrotic syndrome rarely causes pseudochylous ascites. Here the present authors report a case of 24-month-old child (male) who presented with clinical features of nephrotic syndrome. Diagnostic paracentesis was done which strikingly showed milky colour ascitic fluid. Physical appearance of ascitic fluid and laboratory findings were consistent with nephrotic syndrome associated with pseudochylous ascites. He was started on medical treatment and is under regular follow-up. Pseudochylous ascites should be considered in differential diagnosis of milky colour ascitic fluid in nephrotic syndrome.
Children, Oedema, Paracentesis
Case Report
A 24-month-old child (male) presented to Paediatric Intensive Care Unit (PICU) with chief complain of swelling all over the body for last six days, initially started from face then involved whole body progressively, more in the morning hours with abdominal distension. The medical history, family history, antenatal, natal and post-natal history was not significant. He was immunised as per his age (BCG scar present over left arm), achieved all milestones as per age.
On admission, heart rate was 112 beats/minute, respiratory rate 26/minute, SpO2 98% at room air, blood pressure was 98/64 (between 50th and 8th centile). On general physical examination, the child had generalised swelling all over the body with scrotal oedema, everted umbilicus and pitting oedema. On per abdominal examination, abdomen was distended, tense, shiny, non tender and fluid thrill was present on percussion.
He was investigated thoroughly to delineate the cause of generalised oedema. His blood reports were as follows: Haemoglobin 11.2 gm%, leukocyte count 9.0×1000/Cumm, platelet count 300×1000/Cumm, renal function test showed urea-24 mg/dL, creatinine- 0.24 mg/dL, uric acid- 5 mg/dL, serum sodium- 136 mEq/L, potassium- 3.9 mEq/L, chloride-100 mEq/L, bilirubin total- 0.22 mg/dL, bilirubin direct- 0.10 mg/dL, SGOT-37IU/L, SGPT-30IU/L, alkaline phosphate- 84IU/L, total protein-4.0 gm/dL, albumin-1.6 gm/L. Fasting lipid profile showed hypertriglyceridaemia (324 mg/dL) and hypercholesterolaemia (557 mg/dL). Urine routine examination was 4+ for albumin; his 24-hour urine for albumin was 2.9 gm, with urine output of 750 mL in 24 hours. USG abdomen showed massive ascites.
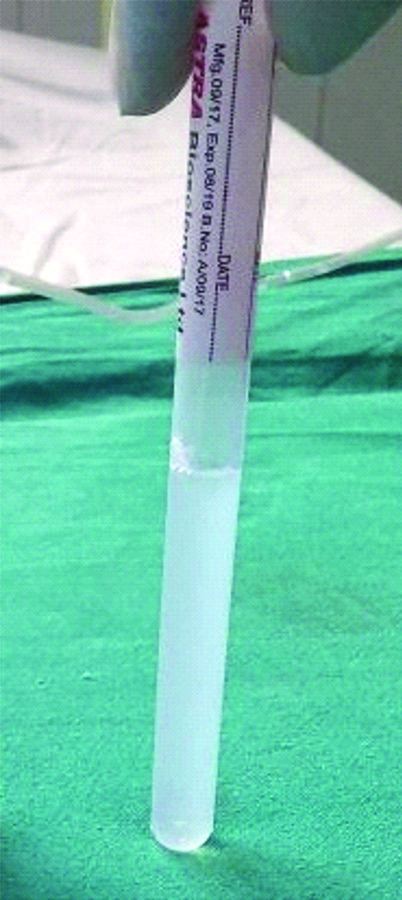
Milky colour ascitic fluid was detected after abdominal diagnostic paracentesis [Table/Fig-1]. Routine analysis of ascitic fluid revealed: cell count 104/mm3 (lymphocyte predominant), glucose- 112 mg/dL, protein- 0.1 gm/dL, albumin-0.1 gm/dL, triglyceride level 49 mg/dL; and adenosine deaminase 6 U/L. Gram stain of ascitic fluid had no pus cells, no bacteria. Ascitic fluid culture was sterile. Routine urine showed 4-5 pus cells with albumin +4, urine culture was sterile. Physical appearance of ascitic fluid and ascitic fluid analysis reports were consistent with pseudochylous ascites associated with nephrotic syndrome (hypoalbuminemia, oedema, proteinuria and hypercholesterolemia). After diagnosis prednisolone (2 mg/kg/day) was started and patient got relieved after 10 days of steroids and discharged on oral steroid for 3 month and asked for regular follow-up.
Milky colored ascitic fluid.
Discussion
Ascites is a clinical manifestation of a number of diseases, including malignancy, renal diseases, cardiac diseases, hepatic diseases and infection. In children, renal disorders are the most common causes of ascites [1]. Nephrotic syndrome is one of the common renal disorder presented with ascites or generalised swelling. In children, differential diagnosis of milky colour ascitic fluid includes chylous ascites, spontaneous bacterial peritonitis and pseudochylous ascites [2]. Chylous ascites is defined as a milky colour, triglyceride-rich ascitic fluid, characterised by the presence of thoracic or intestinal lymph in the abdominal cavity [3]. In children, congenital lymphatic abnormalities and trauma are considered the most common aetiologies [4].
Diagnostic paracentesis is indicated in children with undifferentiated ascites or suspected complications like Spontaneous bacterial peritonitis Peritonitis (SBP). Ascitic fluid is analysed for colour, cell count, gram staining, glucose levels, protein level, triglycerides levels, Adenosine Deaminase (ADA) levels and culture [5]. Spontaneous bacterial peritonitis is confirmed by a predominance of polymorphonuclear cells (>250 cells/μL), a positive Gram stain or a positive culture [6].
On the basis of triglyceride concentration of >200 mg/dL and milky ascitic fluid the diagnosis of chylous ascites is made [7]. The pseudochylous ascites can be due to either long standing collection of fluid in peritoneal cavity or post inflammatory (degeneration of leukocytes without high concentration of triglycerides or active peritoneal infection). The chronic long standing effusions contain breakdown parts of cell membranes which are rich in cholesterol with no triglycerides and chylomicrons [7]. Chylous and pseudochylous ascites may be differentiated by presence of chylomicrons and triglyceride levels [8]. Nephrotic syndrome with milky colour ascitic fluid but without SBP is a very rare coexistence in children.
Conclusion
Milky colour ascitic fluid may occur without any obvious demonstrable obstruction in lymph channels. Nephrotic syndrome should be considered in the differential diagnosis.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Sep 24, 2019
Manual Googling: Nov 06, 2019
iThenticate Software: Nov 15, 2019 (15%)
[1]. Oey RC, van Buuren HR, de Man RA, The diagnostic work-up in patients with ascites: current guidelines and future prospectsNeth J Med 2016 74(8):330-35. [Google Scholar]
[2]. Huang LL, Xia HH, Zhu SL, Ascitic fluid analysis in the differential diagnosis of ascites: focus on cirrhotic ascitesJ Clin Transl Hepatol 2014 2(1):58-64.10.14218/JCTH.2013.00010 [Google Scholar] [CrossRef]
[3]. Cardenas A, Chopra S, Chylous ascitesAm J Gastroenterol 2002 97:1896-900.10.1111/j.1572-0241.2002.05911.x12190151 [Google Scholar] [CrossRef] [PubMed]
[4]. Steinemann DC, Dindo D, Clavien PA, Nocito A, Atraumatic chylous ascites: systematic review on symptoms and causesJournal of the American College of Surgeons 2011 212(5):899-905.10.1016/j.jamcollsurg.2011.01.01021398159 [Google Scholar] [CrossRef] [PubMed]
[5]. Tarn AC, Lapworth R, Biochemical analysis of ascitic (peritoneal) fluid: what should we measure?Ann Clin Biochem 2010 47:397-407.10.1258/acb.2010.01004820595402 [Google Scholar] [CrossRef] [PubMed]
[6]. Runyon BA, Akriviadis EA, Keyser AJ, The opacity of portal hypertension-related ascites correlates with the fluid’s triglyceride concentrationAm J Clin Pathol 1991 96(1):142-43.10.1093/ajcp/96.1.1422069132 [Google Scholar] [CrossRef] [PubMed]
[7]. Kasper DL, Braunwald E, Fauci AS, Harrison’s principles of internal medicine 2011 18th editionNew York, USAMcGraw-Hill [Google Scholar]
[8]. Senousy BE, Dragnov PV, Evaluation and management of patients with refractory ascitesWorld J Gastroenterol 2009 15:67-80.10.3748/wjg.15.6719115470 [Google Scholar] [CrossRef] [PubMed]