Proliferative Diabetic Retinopathy (PDR) occurs in 50% of cases of diabetic retinopathy after 25 years of onset of diabetes. Neovascularization associated with diabetic retinopathy stimulates scar formation, which leads to retinal detachment, the separation of the neuro-sensory retina proper from the retinal pigment epithelium. Management options, which include pars plana vitrectomy, anti-Vascular Endothelial Growth Factor (anti-VEGF) injections, and pan-retinal LASER photocoagulation, are not always effective. Here, the present authors report a case of 41-year-old male who presented with foreign-body sensation for 1 year, photophobia for 8 months, and distorted image perception for 6 months. The patient was diagnosed as having Kacha (diminished vision) according to Ayurveda. He was managed using oral medications, viz., Samirapancakam Kashaya, Cirivilvadi Kashaya, and Laksha Jala, and external therapy, which comprised of local therapies for both the eyes and head. Assessment at discharge by fundus photography demonstrated reduction in retinal haemorrhages, and optical coherence tomography showed reduction in macular oedema and vitreo-macular traction.
Case Report
A 41-year-old male presented to the OPD with a complaint of foreign body sensation in both eyes (OU) since one year associated with photophobia OU since 8 months and distorted image perception OU for 6 months.
The patient was apparently healthy before one year, after which he started gradually experiencing foreign body sensation, which he neglected. Photophobia developed 8 months ago. The patient consulted an ophthalmologist, who diagnosed him with Proliferative Diabetic Retinopathy (PDR) and retinal detachment. He underwent pars plana vitrectomy and silicone oil removal in his right eye but got no relief. Gradually, his left eye also became affected. He was diagnosed with PDR in his left eye and underwent two courses of Laser therapy. He has advised surgery in his left eye also, but he refused. He came to Hospital to seek alternative options.
The patient is a known diabetic for 8 years and has been under medication for 6 months. His father was a known case of diabetes. His treatment history is remarkable for pars plana vitrectomy in his right eye in November 2018, silicone oil removal in his right eye in February 2019, and two rounds of Laser therapy in his left eye in January 2019. His personal history is unremarkable and he does not have any addictions or habits.
Distant Visual Acuity (DVA) at admission was hand movements (HM+ve) in his right eye (OD) and 6/36 Snellen (LogMAR 0.77) in his left eye (OS); anterior segment examination OU was normal; and pupillary reactions OU were within normal levels.
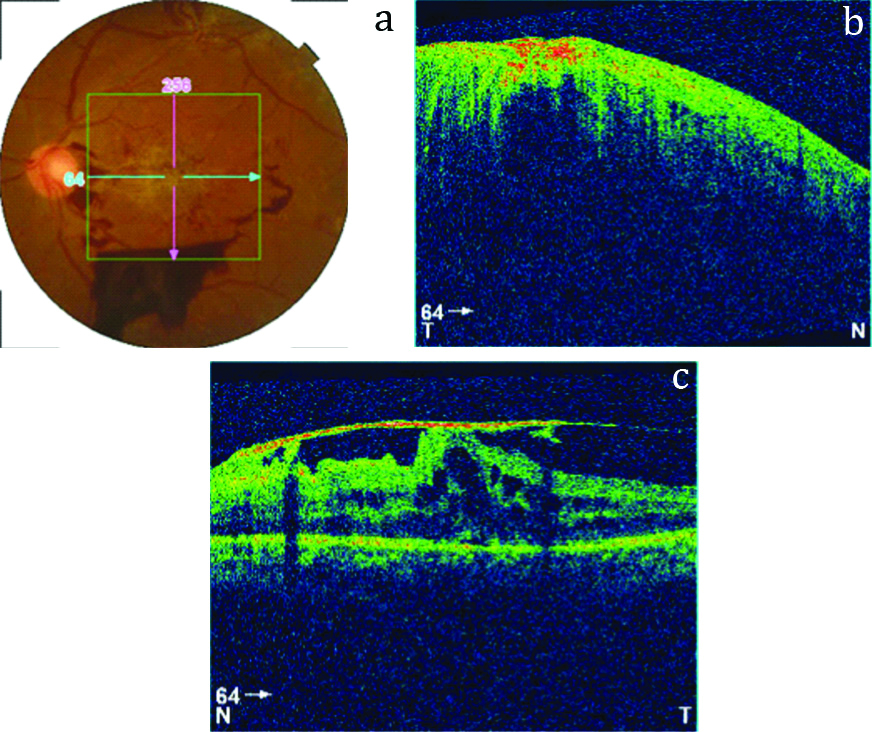
Fundus examination OS showed a macular scar and presence of haemorrhages near the optic disc and in the inferior quadrant [Table/Fig-1a]. Optical Coherence Tomography (OCT) scanning OD showed elevation of the retina due to vitreous accumulation under the structure [Table/Fig-1b]. OCT scanning OS showed vitreo-macular traction and cyst-like lesions at the macula, suggestive of cystoid macular oedema and tractional retinal detachment [Table/Fig-1c].
a) Fundus photograph OS at admission; b) OCT scan OD at admission; c) OCT scan OS at admission.
A provisional diagnosis of proliferative diabetic retinopathy with tractional retinal detachment was made based on the examination and investigations. Raktaja Kacha (diminished vision due to blood), a Drishtigata Roga (disease of vision) according to Ayurveda, was explored for this patient based on the symptom of blurring of vision and vascular abnormalities and haemorrhages seen in the fundus. Parimlayi, a type of Kacha according to Susruta, and involvement of Rakta Dhatu (haemoglobin fraction of blood) was explored based on the changes in the retinal vasculature seen in proliferative diabetic retinopathy. Tractional retinal detachment was explored along the lines of increased Kapha Dosha and Rakta.
He was prescribed Samirapancakam Kashaya (60 mL at 6 am and 6 pm)*, Cirivilvadi Kashaya (60 mL at 10 am and 4 pm), and Laksha Jala (500 mL at 10 am) orally [Table/Fig-2]. External therapies included Siroveshtana (application of paste on a Cora cloth over the head), Anjana (collyrium), Ascyotana (eye drops), Purampada (application of paste over the eyelid), Sirolepa (application of paste over the head), and Talapoticchil (application of paste in a plantain leaf over the head) [Table/Fig-3].
| Medicine | Preparation | Dosage | Time | Duration |
|---|
| Samirapancakam Kashaya (decoction of Cyperus rotundus Linn., etc.)* | 1 part of the ingredients are boiled in 4 parts of water and reduced to 1/4. | 60 mL | 6 am and 6 pm | 07/05/2019-22/05/2019 |
| Cirivilvadi Kashaya (decoction of Holopteleaintegrifolia Planch., etc.) | 1 part of the ingredients are boiled in 4 parts of water and reduced to 1/4. | 60 mL | 10 am and 4 pm | 10/05/2019-14/05/2019 |
| 10 am | 15/05/2019-23/05/2019 |
| Laksha Jala (water processed with Laccifer lacca Kerr.) | 1 part of the powder is taken and mixed with 500 mL of water | 500 mL | 10 am | 10/05/2019-23/05/2019 |
| Treatment | Medicine | Method of administration | Duration |
|---|
| Siroveshtana | Vasa Lakshadi Churna (powder prepared from Adathodavasica Nees., etc.) | 45g of powder was made into a paste by mixing with water. The decoction was added to one Gutika (tablet). A Cora cloth was immersed in 350 mL of the decoction and the paste is smeared over the cloth. The cloth was applied over the forehead from one ear to the other and tied over the head. | 07/05/2019-12/05/2019 |
| VasaTriphalaKvatha (decoction of Terminaliachebula Retz., etc.) |
| KaruttaGutika (tablet prepared from Boswellia serrata Planch., etc.) |
| Anjana | Netramrtam (sterile drops prepared from NaCl, etc.)* | 1 drop of the medicine was instilled from a height of 2 Angula (2 fingers) in both eyes. The patient was asked to gently rotate the eyes while keeping them closed. | 07/05/2019 |
| Ascyotana | Drops prepared from Veroniacinerea Less. | 07/05/2019-19/05/2019 |
| Purampada | Desmodiumtriflorum Linn. and Cynodondactylon C. Fisher | A paste prepared from the medicine was applied over the eyelid, obviating the lashes. | 16/05/2019-24/05/2019 |
| Sirolepa | Desmodiumtriflorum Linn. and semisolid constituency of Adathodavasica Nees. | 60g of the powdered ingredients and semisolid were made into a paste and applied to the forehead. | 16/05/2019-24/05/2019 |
| Talapoticchil | Vasa LakshadiChurna (powder prepared from Adathodavasica Nees., etc.) | A paste prepared by mixing 60g of the powder and 300 mL of the decoction mixed with the tablet was applied on a plantain leaf, which was kept face down over the head, obviating a small circular hole in the centre. | 16/05/2019-24/05/2019 |
| VasaTriphalaKvatha (decoction of Terminaliachebula Retz., etc) |
| KaruttaGutika (tablet prepared from Boswelliaserrata Planch.) |
Ingredients for the medicines were procured at Sreedhareeyam’s own herbal gardens and the medicines were manufactured by Sreedhareeyam Ayurvedic Medicines Pvt. Ltd., the hospital’s GMP-certified manufacturing unit.
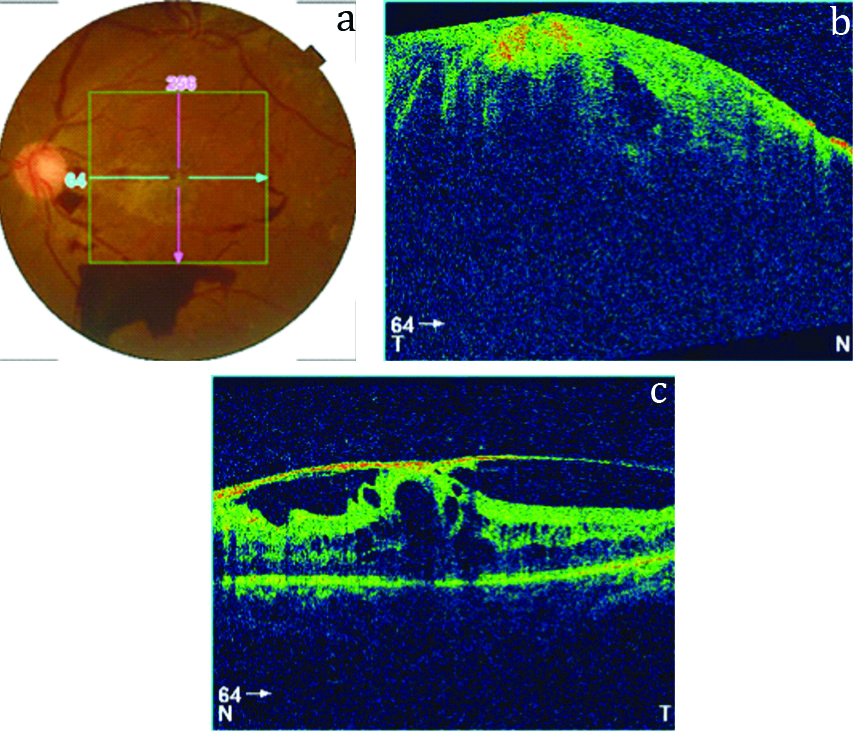
Assessment was done by DVA, fundus examination, and OCT. DVA was maintained at discharge. Fundus examination OS showed reduction in haemorrhages [Table/Fig-4a]. OCT scanning OD showed absorption of vitreous humour from the retina [Table/Fig-4b]. OCT scanning OS showed reduction in vitreo-macular traction and absorption of macular oedema [Table/Fig-4c].
a) Fundus photograph OS at discharge; b) OCT scan OD at discharge; c) OCT scan OS at discharge.
The patient was prescribed medicines at discharge [Table/Fig-5] and advised regular follow-ups. One of the medicines, Chimium-Co, was manufactured by J&J Dechane Laboratories Pvt. Ltd.; the others were manufactured by Sreedhareeyam Ayurvedic Medicines, Pvt. Ltd. A timeline of events is also given [Table/Fig-6].
| Medicine | Dosage | Time |
|---|
| Samirapancakam Kashaya (decoction of Cyperus rotundus Linn., etc.)* | 15 mL with 45 mL boiled and cooled water | Twice a day before food |
| AmalakiChurna (powder of Emblicaofficinalis Gaertn.) | 5 gm | Make into a paste by mixing with decoction and apply over the forehead for one hour |
| LakshaChurna (powder of Lacciferlacca Kerr.) | 5 gm |
| Chinium-Co (capsule prepared from Rheumemodi Wall.)^ | 1 capsule | Twice a day after food |
| VasaSree (tablet prepared from Adathodavasica Nees., etc.)* | 1 tablet | Twice a day after food |
| VaraCurna (powder prepared from Terminaliachebula Retz., etc.) | 3 gm | 1/2 hour after food at night |
| Cardocure (tablet prepared from Rauwolfiaserpentina Royle ex. Benth., etc.)* | 1 tablet | Twice a day after food |
| Time | Event |
|---|
| 05/2018 | Experiences foreign body sensation OU, which he neglects
|
| 09/2018 | Experiences photophobia OU
|
| 11/2018 | Experiences distorted vision OD Diagnosed with proliferative diabetic retinopathy and retinal detachment Pars plana vitrectomy OD and injection of silicone oil
|
| 01/2019 | Experiences distorted vision OS 2 rounds of LASER therapy OS Advised surgery, which he declines
|
| 02/2019 | Silicone oil removal OD
|
| 06/05/2019 | Consultation at Sreedhareeyam and admission for inpatient management DVA: HM +ve OD and 6/36 OS Fundus exam OS: macular scar and haemorrhages near the optic disc and in the inferior quadrant OCT scanning OD: elevation of the retinal layers due to vitreous accumulation OCT scanning OS: vitreo-macular traction and cyst-like lesions at the macula
|
| 07/05/2019 | Samirapancakam Kashaya* is started Siroveshtana with VasaLakshadiChurna, VasaTriphaladiKashaya, and KaruttaGutika is started Anjana with Netramrtam* is done Ascyotana with drops prepared from Veronia cinerea Less. is started
|
| 10/05/2019 | CirivilvadiKashaya is started (at 10 am and 4 pm) LakshaJala is started
|
| 12/05/2019 | Siroveshtana is stopped
|
| 15/05/2019 | CirivilvadiKashaya is continued by giving only at 10 am
|
| 16/05/2019 | Purampada with paste prepared from Desmodiumtriflorum Linn. and Cynodondactylon C. Fisher. is started Sirolepa prepared from Desmodiumtriflorum Linn. and semisolid constituency of Adathodavasica Nees. is started Talapoticchil with VasaLakshadiChurna, VasaTriphaladiKashaya, and KaruttaGutika is started
|
| 19/05/2019 | Ascyotana is stopped
|
| 22/05/2019 | SamirapancakamKashaya is stopped
|
| 23/05/2019 | LakshaJala is stopped
|
| 24/05/2019 | Purampada, Sirolepa, and Talapoticchil are stopped Fundus exam OS: Reduction in haemorrhages OCT scan OS: Reduction in vitreo-macular traction and absorption of macular oedema OCT scan OD: Absorption of vitreous
|
*Patented medicines of Sreedhareeyam Ayurvedic Eye Hospital and Research Centre
^Patented medicine of J & J Dechane Laboratories
Discussion
Diabetic retinopathy (DR) is a micro-angiopathy that primarily affects pre-capillary arterioles, capillaries, and post-capillary venules of the retina [1]. The Early Treatment Diabetic Retinopathy Study (ETDRS) classifies DR into background or Non-Proliferative DR (NPDR), diabetic maculopathy, pre-proliferative DR, proliferative DR (PDR), and advanced diabetic eye disease. PDR affects 5-10% of the diabetic population, especially Type 1 diabetic, with an incidence of 60% after 30 years [2]. In general, the pathogenesis of DR involves cellular damage.
Neovascularization, the hallmark finding of PDR, can be either at the optic disc (neovascularization disc or NVD) or elsewhere (neovascularization elsewhere or NVE). It is caused by capillary non-perfusion, which leads to retinal hypoxia. New vessel growth is thought to be caused by an imbalance between angiogenic and anti-angiogenic factors, in an attempt to re-vascularize the already hypoxic retinal tissue. Neovascularization may encourage scarring at the macula, which results in retinal detachment.
Kacha is a Drishtigata Roga (disease of vision) described by Acharya Vagbhata in the Ashtanga Hrdaya Uttara Sthana. When the pathological Doshas (humours) invade the 3rdPatala (layer) of the eye, objects are perceived above but not below, objects are covered by a thin cloth, vision gradually reduces, and the area of vision (Drshti) gets colorized based on the Dosha [3]. Raktaja Kacha is characterised by redness of the organ of vision and seeing of objects as either red or black [4].
The concept of Meha (metabolic disorders including diabetes) as a cause for Netraroga was mentioned by Netra Prakashika, an ancient text dealing with eye care [5]. The Samprapti (pathogenesis) of diabetic retinopathy according to Ayurveda revolves around Srotobhishyanda (pathological oozing of fluid from Srotas or channels) and Raktavaha Sroto Dushti (pathological activity of the channels carrying blood) [6]. Acakshushya Ahara and Vihara (diet and lifestyle choices detrimental to eye health) aggravate Pitta Dosha. Pitta in turn aggravates Rakta as the two share Asraya Asrayi Bhava (homologous connection) with each other. These two traverse the Urdhvavaha Sira (vessels of the upper extremity) and lodge in Netra. The pathogenic factors of DR are due to the Kleda (moisture) and Kapha in Prameha, causing Srotorodha (obstruction of the channels) in the retinal vasculature. This Srotorodha results in Atipravrtti (increased flow) of already-increased Doshas, which may be compared to neovascularization [7].
In this patient, the neovascularization caused a macular scar, which in turn led to a tractional retinal detachment. The Atipravrtti of Doshas ended up at the macula and the already-increased Kapha solidified Rakta into a scar. The Gurutva (heaviness) and Mahatva (prominence) of Kapha caused the mzàcula to undergo tractional movement and thus detach the retina from its normal place.
Based on the above descriptions, a treatment protocol according to Ayurvedic principles may be explored. Two case studies of diabetic retinopathy managed with Ayurvedic treatments such as Panchakarma (detoxification) and Kriyakalpa (local ocular therapeutics) showed improvement in maintenance of serum glucose, identification of primary colours, and clarity of vision both at discharge and at follow-ups [8].
Ciribilvadi Kashaya acts as a digestive agent and helps move adherent Doshas including Vata downwards. Laksha (Laccifer lacca Kerr.), by its properties of Pitta-Kapha Nasaka (diminishing Pitta and Kapha), Sandhaniya (binding), Balya (strengthening), and Ropana (healing), helps the retina restore itself to the rest of the eye, and at the same time, treats Rakta by acting on Pitta and Kapha. Mixing Laksha with water helps to flush out the impurities caused by aggravated Pitta and Kapha.
Siroveshtanam, Sirolepa, and Talapoticchil reach the target tissue by absorption through the skin and hair follicles. This allows them to bypass the blood-brain barrier and the blood-ocular barriers.
The ingredients used for Siroveshtana, Sirolepa, and Talapoticcihil all act on Rakta Dhatu, Netra (eye), and help to rejoin the retina to the rest of the eye. Vasa (Adathoda vasica Nees.) is known to treat Raktapitta (bleeding disorders) by its wound-healing properties. Vasa improved breaking strength, absorption, and extensibility in wound tissue, and hence has been proven to be an excellent wound healing drug [9]. Triphala (Terminalia chebula Retz., Terminalia bellerica Linn., and Emblica officinalis Gaertn.) are indicated in both Prameha (diabetes) and Netra Roga (ophthalmic diseases). Terminalia chebula Retz. and Terminalia bellerica Linn. have antioxidant properties, which eliminate free radicals in the retinal tissue. The ingredients of Karutta Gutika possess binding and healing properties, and thus enable the retina to firmly adhere to the rest of the eye.
Purampada (application of paste over the closed eyelids) reduces pressure by applying counterpressure from the lids. It allows for faster mobilisation of toxins, stimulation of peripheral nerves, and reducing subretinal fluid in the eye. Ascyotana (eye drops) and Anjana (collyrium) allows deeper penetration by factors such as height and temperature of the medicine.
Samirapancakam Kashaya, prepared from Cyperus rotundus Linn., Hordeum vulgare Linn., Picorrhiza kurroa Royle. ex. Benth., Santalum album Linn., and Tinospora cordifolia Miers., is indicated in Pramehajanya Netraroga (DR) and Raktapitta (bleeding disorders). Netramrtam is prepared from NaCl, KAl (SO4)2, and distilled water, and is a promoter of vision. Vasa Sree is prepared from Adathoda vasica Nees., Mesua ferrea Linn., Emblica officinalis Gaertn., and Hemidesmus indicus Linn., and is indicated in Raktaja Netra Rogas (ophthalmic diseases caused by blood) and diabetic retinopathy. Cardocure is prepared from Rauwolfia serpentina Royle ex. Benth, Terminalia chebula Retz., Terminalia bellerica Linn., Emblica officinalis Gaertn, and Clitoria ternatea Linn., and is indicated in hypertensive conditions.
Challenges in managing of DR include vigorous maintenance of serum glucose and preservation of existing vision. Promising effects of the Ayurvedic intervention were noted in the fundus examination and OCT scanning. Vision was maintained throughout, with no further deterioration. Hence, this modality may be explored.
Conclusion
This Ayurvedic protocol for managing Proliferative Diabetic Retinopathy (PDR) and TRD not only targeted the ocular conditions, but enabled normal physiology to be adequately restored in terms of digestion and metabolism. Hence, the protocol may be considered as a treatment option. The case may be used as a stepping stone for further management and the results obtained may be verified using large-scale sample trials.
*
Patented medicines of Sreedhareeyam Ayurvedic Eye Hospital and Research Centre^Patented medicine of J & J Dechane Laboratories
[1]. Kanski JJ, Clinical Ophthalmology: A Systematic Approach, 5th Edition 2003 Butterworth Heinemann, an imprint of Elsevier Science Limited:439 [Google Scholar]
[2]. Kanski JJ, Clinical Ophthalmology: A Systematic Approach, 5th Edition 2003 Butterworth Heinemann, an imprint of Elsevier Science Limited:447 [Google Scholar]
[3]. Murthy K R S, Ashtangahrdaya of Vagbhata: Text, English Translation, Notes, Appendices, and Index 1997 Vol. III2nd EdVaranasiUttara Sthana, Krishnadas Academy:107 [Google Scholar]
[4]. Murthy KRS, Ashtangahrdaya of Vagbhata: Text, English Translation, Notes, Appendices, and Index 1999 Vol. IIIVaranasiUttara Sthana, Krishnadas Academy:109 [Google Scholar]
[5]. Shankar U, Netra Prakashika of Ayurveda Shatpannasara 2013 1st EdVaranasiChaukhambha Vishwabharati:31 [Google Scholar]
[6]. Sahoo PK, Fiaz S, Conceptual analysis of diabetic retinopathy in AyurvedaJournal of Ayurveda and Integrative Medicine 2017 (8):122-131.10.1016/j.jaim.2016.12.00328526441 [Google Scholar] [CrossRef] [PubMed]
[7]. Dastapure M, Shekar V, Mamatha KV, Sujathamma K, Diabetic retinopathy and its management in Ayurveda-A Special Case ReportInternational Ayurvedic Medical Journal 2015 3(8) [Google Scholar]
[8]. Sandhya Rani D, Seetha Devi P, Kulkarni PS, Ayurvedic Management of Diabetic Retinopathy- Case StudyInternational Journal of Innovative Pharmaceutical Sciences and Research 2015 3(8):1185-1191. [Google Scholar]
[9]. Gangwar AK, Ghosh AK, Medicinal uses and Pharmacological activity of Adathoda vasicaInternational Journal of Herbal Medicine 2014 2(1):88-91. [Google Scholar]