Introduction
Children with hearing loss are either fitted with hearing aid or implanted with Cochlear implants and Brainstem Implants. It is essential for these children to undergo intervention during the critical period, a lot of objective evidences such as Brainstem Evoked Response Audiometry, Late Latency Response and Mismatch Negativity have shown the benefit of early implantation, there is also a need to document subjective evidences to show the outcomes of early implantation.
Aim
To compare the auditory performance in early and late Implantees using LittlEARS Auditory Questionnaire.
Materials and Methods
A cross-sectional descriptive study was designed. Children with bilateral profound hearing loss, unilateral cochlear implant users and implant ages between six months to 24 months were considered for the study. A hundred random samples of parents of Congenital Hearing Impaired children participated. A Tamil translated version of LittlEARS Auditory Questionnaire was administered to the parents of cochlear implantees, the samples were grouped as early implantees and late implantees. Mean scores were analysed and compared between the groups using descriptive and inferential statistics.
Results
Results reveal early Implantees had a better mean (28.52) score of auditory development than late implantees (27.69) and statistical significance (<0.005) was not obtained between the groups. This shows that the performance did not significantly differ between the groups, in terms of auditory behaviour and early preverbal skills.
Conclusion
LittlEARS Auditory Questionnare is a better and promising tool to measure outcomes in cochlear implant and also provides us the evidence, the need for early implantation.
Auditory verbal therapy, Critical period, Development, Early preverbal skills, Objective measures, Subjective measures
Introduction
The term critical period (Biological Maturation) is used to depict neurosensory development that takes place in children, plasticity of neurosensory period is maximum at earlier ages when compared to late ages. There are number of developmental process that takes place during critical period which include myelination, dendritic pruning and axonal growth [1]. Gable S et al., in 2000 stated that at birth, the human brain is still not developed completely. In initial three years of life, the brain organises and reinforces the connections with neighbouring neurons. These connections happen when stimulus is transmitted to and forth between the neurons. Axons sends messages and dendrites receive them and hence these connections form synapses. These synapses become more complex as the child grows. Though the amount of neurons remains constant, the amount of synapses increases day by day with new experiences in the initial three years of life. After three years of age, spreading of synapses slows down until about ten years of age. During the critical period, the brain multiplies the synapses that it needs and this period takes place in the initial three years of life. Few synapses will stay permanently in brain and few will be eliminated. This is where experience plays an important role in wiring a young child’s brain [2].
Literature reported by Kappel V et al., states that there is a possible anatomical or functional change at the level of auditory system with respect to the new arrival of information and their view strongly supports the auditory plasticity mechanism [3]. So it is important to know the mechanism behind how an individual with hearing impaired react to the auditory events. Hearing loss has an effect on decreasing the calibre to perceive and detect sounds, which also affects the individual’s limitation in other domains such as social, and emotional development.
Musiek FE et al., reported that, the auditory system’s plasticity increases with the influence from the environment [4]. They also reported that plasticity in the sensory system can be seen in both peripheral pathways and central pathways. Transmitting acoustic information can make changes in physiological, biochemical or anatomical properties of the central neurons (it is also a biodynamic phenomenon). The auditory system is capable of recognising itself even though changes occur (plasticity), since stimulus input changes (i.e., decreased input for cochlear injury or increased input for postnatal development and when assistive devices are placed).
Individuals with congenital severe to profound hearing loss require management options. These management options include hearing aids, Cochlear implants (CI) [5] and Auditory Brainstem Implants (ABI) [6]. The outcomes of treatment depends on the age at Implantation and Duration of Deafness. Various studies support the fact that early Implantation results in better prognosis.
Sharma A et al., conducted a study in 2002 by comparing P1 responses in early and late implantees, they had found out that early implanted children had better wave morphology and earlier P1 latency response [7]. Zhang F et al., studied the effect of mismatch negativity in late implanted children, where they had found out that moderate to poor performers had small or absent Mismatch Match Negativity (MMN) thus concluding that late implantation not only has an effect on the auditory cortical level but also affects the cognitive level [8].
There are several studies that have documented the effect of early and late implantation using objective test measures, but there are several limitation in relying only on objective test procedures as it is time consuming, restricted to laboratory and difficult to measure patient perspective outcomes. On the other hand subjective tests are easy to administer, less time saving, cost effective and gives us patient perspective and realistic outcomes. Subjective tests can be directly administered to the patients or given in the form of a questionnaire to parents.
Some of the known subjective tools for measuring auditory skills are Categories of Auditory Perception (CAP) scale, Speech Intelligibility Rating (SIR) scales, Meaningful Auditory Integration Scale (MAIS) and Infant Toddler Meaningful Auditory Integration Scale (IT-MAIS). But these tools lack several domains to assess auditory skills. Out of the subjective tools available, the LittlEARS Auditory Questionnaire tool is found to assess both auditory behaviour and early auditory preverbal skills [9]. The tool also provides the feasibility to translate and validate across different cultural and linguistic backgrounds.
With limited literature available, there is a need to document a research that measures the outcomes of early implantation using subjective tests, LittlEars Auditory Questionnaire is the most feasible tool that gives us the option to measure the auditory skills and early preverbal skills of children.
The aim of the study was to compare the auditory performance in early and late implantees using LittlEARS Auditory Questionnaire, with the objectives of profiling the auditory development of cochlear implantees with their implant age within two years of age and later comparing the performance of early and late implantees.
Materials and Methods
The clinical study work was approved by the Ethical Committee guidelines followed at Madras ENT Research Foundation-Institute of Speech and Hearing (P) ltd. (Ethical clearance number-EC-AUG.17/15).
Research Design
A cross-sectional descriptive study was aimed to estimate the parental experiences and preverbal auditory development of Paediatric Cochlear Implantee that represent Indian community. The study commenced for a total period of six months from July 2017 to January 2018 from commencement till completion.
Participants of the Study
Hundred random samples considered for this study were parents of prelingual (Congenitally deaf) paediatric cochlear implantees who were implanted in the same centre participated in the study. Randomisation was done through a simple random sampling. The questionnaire was administered to the parents of the cochlear implanted children, who were native Tamil speakers and able to read Tamil. The random samples were later divided into early and late implantees based on their age at implantation with age at implantation below 3.5 years considered as early implantees and above 3.5 years considered late implantees [7]. The Questionnaire used was a Tamil version of LittlEARS Auditory Questionnaire (LEAQ) [10].
Inclusion Criteria
Participants with congenital bilateral severe to profound hearing loss and having a normal cochlear anatomy were selected as participants. Participants chosen were unilateral Cochlear Implant users with chronological ages between one to ten years (mean age of 4.18 years) and implant ages between six months to 24 months (mean age of 12.5 months). Study included children with cochlear implant, who were undergoing their one year Auditory Habilitation with a minimum of six months auditory habilitation Programme and also their recent Aided audiometry results were well within the speech spectrum. In relevance to experience, regular usage of cochlear implant was considered.
Exclusion Criteria
Participants of post lingual deafness were excluded. The children with implant ages beyond two years and chronological age above 10 years were not included in the present study. Individuals with inner ear or nerve abnormalities such as thin cochlear nerve, aplasia or dysplasia and Auditory Neuropathy Spectrum Disorders (ANSD) were excluded. Children of Bimodal device usage, Re-implantation, Neuro-developmental disorders and other syndromes were also eliminated from the study.
An informed consent were sent to the chosen parents of cochlear implant children who met the inclusion criteria. Parents were informed about the test procedure, the test duration and the purpose of conducting the study.
The questionnaire consisted of 35 sequential age-related questions that should be given “Yes” or “No” by the parents. The questions hierarchy is in the order of simple to complex levels. Scoring of the LEAQ consist of “one” point for each yes answers and “zero” for no answers. Interpretations of the LEAQ is higher the “yes” scores better the auditory development [9] (Annexure)
Parents were instructed properly to reduce the response bias and answer each questions based on his/her own experiences with their child. The questionnaire were distributed to all the parents who were implanted in the same implant centre. Out of 100 participants 81 mothers (single parent-mother) were interviewed face to face and four of them were interviewed via E-mail and 15 of the parents were interviewed through phone call since parent could not access the centre.
Statistical Analysis
The data for each group was tabulated and statistical analysis was carried out using Statistical Package for the Social Sciences (SPSS) software version 20.0. To profile the performance of the implanted children, Descriptive statistics and inferential statistics were done. Test of normality was done using the Shapiro Wilkis test, datas were not normally distributed due to which a Mann Whitney test was carried out to find the significance between the two groups.
Results
1. LEAQ Scores for total Number of Samples
Out of the 100 samples 51 were girls and 49 were boys, the mean age was four years. A score of 28.1 had been secured out of 35 as mentioned in [Table/Fig-1], thus signifying that cochlear implant is providing benefit in auditory performance as results obtained are not too deviant from the normal values.
Mean, standard deviation and range of LEAQ scores taken for total number of samples of cochlear implant children, early implantees and late implantees.
| N | Range | Mean | Median | Standard deviation | Skewness | Kurtosis |
|---|
| Total samples | 100 | 25 | 28.10 | 30 | 5.37 | | |
| Early implantees | 40 | 18 | 28.52 | 30 | 4.53 | -1.41 | 1.62 |
| Late implantees | 60 | 25 | 27.69 | 30 | 6.52 | -0.82 | -0.13 |
2. LEAQ Scores for Early Implantees
Hundred randomly selected participants of the study were further grouped into early and late Implantees, children with an age at implantation below 3.5 years were considered early implantees [7]. A total of 40 participants were under the category of early implantees, 15 were males and 25 were females. The mean scores and standard deviation showed remarkable development, the range was found to be less indicating less dispersion.
3. LEAQ scores for Late Implantees
On the other hand 60 participants were under the category of late implantees, these participants had an age at implantation of 3.5 years and above. Out of the 60 participants 26 were females and 34 were males with a mean age of five years. Their mean scores, standard deviation showed remarkable development being late implanted.
4. Comparison between Early and Late Impantees
Inferential statistics was done to find out the significant difference between the LEAQ score of early implanted children and late implanted children. Kolmogorov-Smirnov test and Shapiro-Wilk’s test were done to find out the normality of the data [Table/Fig-2] and the results revealed that the data did not follow a normal distribution curve and hence a non parametric test (Mann Whitney) was used. The results of the z test (z=-0.126, p>0.005) retained the null hypothesis on the equality of the means when comparing with early and late implanted children [Table/Fig-2,3 and 4].
Shapiro-Wilk’s test of normal distribution.
| Tests of normality |
|---|
| Early and late implantees | Shapiro-Wilk |
|---|
| Statistic | df | Sig. |
|---|
| LEAPQ | Early implantee | 0.847 | 42 | <0.001 |
| Late implanteete | 0.921 | 58 | 0.001 |
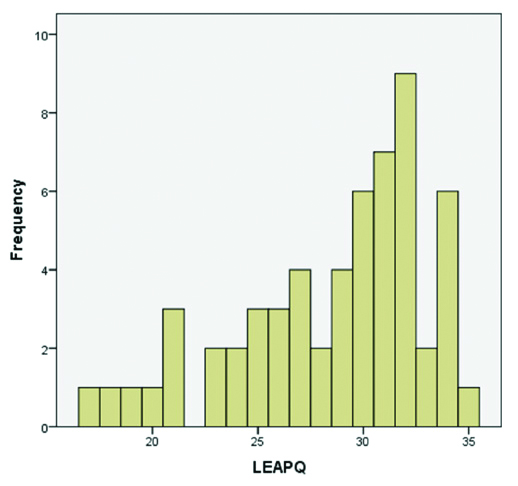
Graph for early implanted children, Mean=28.52.
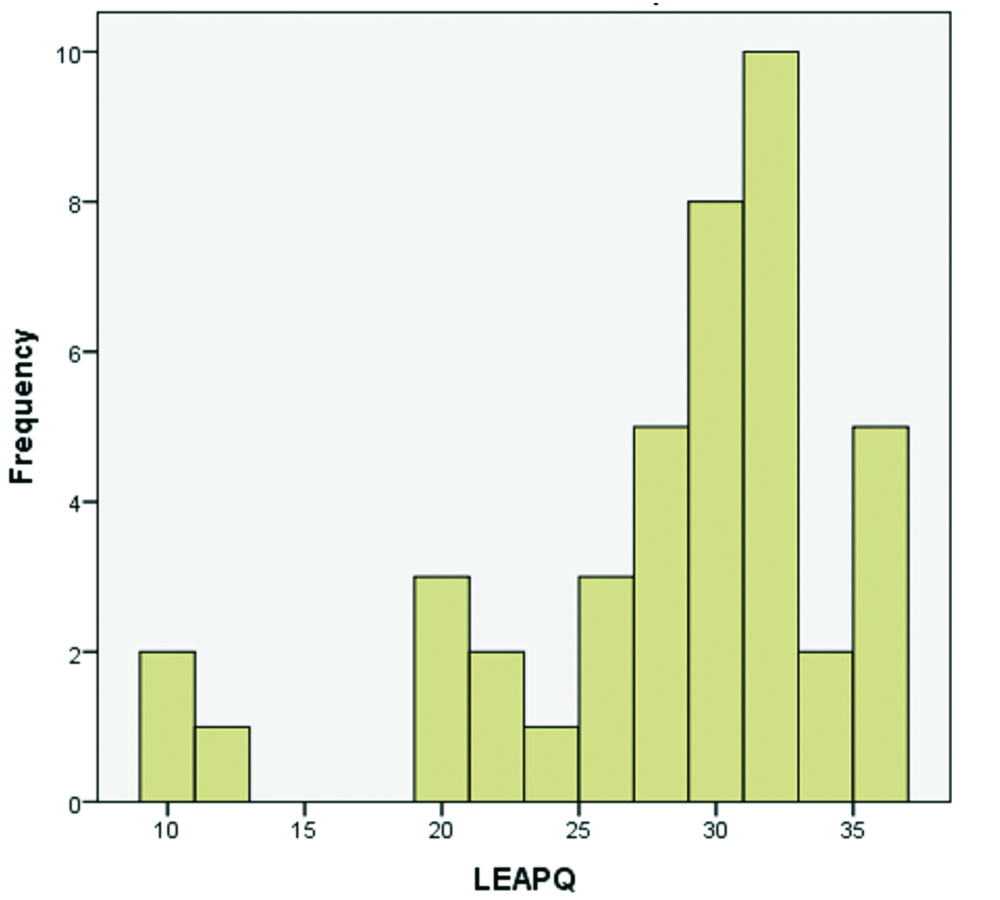
Graph for late implanted children, Mean=27.69.
Discussion
The study aimed at comparing the auditory performances between early implanted and late implanted individuals, null hypothesis was retained in during statistical analysis which signifies that there is not much of differences between early and late implantees in terms of early prevebal skills and auditory development. Most of the literature oppose our findings by providing evidence that early implanted children perform better, study done by Geal-Dor M et al., stated that children with 2 years of hearing age have better scores, in cochlear implant children, the rate of progress was found to be better, these individuals not only improved in their auditory skills and early preverbal skills but also possessed to have better cognitive abilities, another study done by May-Mederake B et al., state that a maximum score of auditory and preverbal skills can be achieved after 22 months of implant age if the child is implanted below two years of age [11,12]. The findings of Wang L et al., mention that early implanted children had faster and steeper improvement in auditory preverbal skills when compared to late implanted children [13]. There has been rapid improvement in children implanted younger than 12 months in their auditory skills where they initially have a delay but later achieve a ceiling limit rapidly [14]. The perfect age for a child to undergo cochlear implantation would be within 2 years as they achieve their milestones 6 months faster when compared to the other groups implanted late [15]. Authors propose the fact that children undergoing cochlear implantation must be given adequate time to develop their auditory skills, receptive and expressive language along with phonological development, hence earlier implantation would give sufficient time to develop [16]. However in some cases there is not much of differences in all domains between the early implanted and late implanted group as they both almost perform equally, which supports our study findings [17]. With a plethora of evidences now available it is proven that early implanted children perform better than late implanted children, however when it comes to early preverbal skills and auditory development, both the groups perform in the similar way.
Limitation
Even though the study has been done on a large population of cochlear implant children, it is essential to compare it with normal hearing population and population of children using hearing aids. The study is a cross-sectional study where a trend could not be established across chronological age, hence it is essential to perform a longitudinal study until 2 years of hearing age in order to monitor the development appropriately. This test tool can be administered in children with anomalous cochlea and ABI children to yield appropriate subjective results from them. A subjective-objective correlation must also be done for better outcome measurement.
Conclusion
The study concludes that based on parental questionnaires, there isn’t much of a difference between the performance of early and late implantees although many literatures provide evidence of early implantees showing better performances when compared to late implantees. This shows that cochlear implantation provides betterment to young congenitally deaf implant users regardless of their age at implantation. It is essential for parents and habilitationalist to provide adequate stimulation to implanted children for a better progress. A similar study with more sample size and longitudinal design must be carried out for yielding better results.
Author Declaration:
Financial or Other Competing Interests: No
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. No
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Jun 14, 2019
Manual Googling: Oct 24, 2019
iThenticate Software: Nov 05, 2019 (5%)
[1]. Harrison RV, Gordon KA, Mount RJ, Is there a critical period for cochlear implantation in congenitally deaf children? Analyses of hearing and speech perception performance after implantationDevelopmental Psychobiology: The Journal of the International Society for Developmental Psychobiology 2005 46(3):252-61.10.1002/dev.2005215772969 [Google Scholar] [CrossRef] [PubMed]
[2]. Gable S, Hunting M, Nature, nurture and early brain development 2000 ColumbiaMU Extension, University of Missouri-Columbia [Google Scholar]
[3]. Kappel V, Moreno AC, Buss CH, Plasticity of the auditory system: Theoretical considerationsBrazilian Journal of Otorhinolaryngolo 2011 77(5):670-74.10.1590/S1808-8694201100050002222030979 [Google Scholar] [CrossRef] [PubMed]
[4]. Musiek FE, Shinn J, Hare C, Plasticity, auditory training, and auditory processing disordersInSeminars in hearing 2002 Vol. 23(No. 04):263-276.Copyright© 2002 by Thieme Medical Publishers, Inc., 333 Seventh Avenue, New York, NY 10001, USA. Tel.:+ 1 (212) 584-466210.1055/s-2002-35862 [Google Scholar] [CrossRef]
[5]. Chen MM, Oghalai JS, Diagnosis and management of congenital sensorineural hearing lossCurrent Treatment Options in Pediatrics 2016 2(3):256-65.10.1007/s40746-016-0056-628083467 [Google Scholar] [CrossRef] [PubMed]
[6]. Shah PV, Kozin ED, Kaplan AB, Lee DJ, Pediatric auditory brainstem implant surgery: A new option for auditory habilitation in congenital deafness?J Am Board Fam Med 2016 29(2):286-88.10.3122/jabfm.2016.02.15025826957388 [Google Scholar] [CrossRef] [PubMed]
[7]. Sharma A, Dorman MF, Spahr AJ, A sensitive period for the development of the central auditory system in children with cochlear implants: implications for age of implantationEar and Hearing 2002 23(6):532-39.10.1097/00003446-200212000-0000412476090 [Google Scholar] [CrossRef] [PubMed]
[8]. Zhang F, Hammer T, Banks HL, Benson C, Xiang J, Fu QJ, Mismatch negativity and adaptation measures of the late auditory evoked potential in cochlear implant usersHearing Research 2011 275(1-2):17-29.10.1016/j.heares.2010.11.00721129468 [Google Scholar] [CrossRef] [PubMed]
[9]. Tsiakpini L, Weichbold V, Kuehn-Inacker H, Coninx F, D’haese P, Almadin S, LittlEARS auditory questionnaire 2004 Innsbruck, AustriaMED-EL [Google Scholar]
[10]. Rahul KR, Jayachandran D, Rajeswaran R, Umashankar A, Adaptation of littlears auditory questionnaire in TamilEuropean Journal of Special Education Research 2019 4(4):162-69. [Google Scholar]
[11]. Geal-Dor M, Jbarah R, Meilijson S, Adelman C, Levi H, The Hebrew and the Arabic version of the LittlEARS® auditory questionnaire for the assessment of auditory development: results in normal hearing children and children with cochlear implantsInternational Journal of Pediatric Otorhinolaryngology 2011 75(10):1327-32.10.1016/j.ijporl.2011.07.03021868106 [Google Scholar] [CrossRef] [PubMed]
[12]. May-Mederake B, Kuehn H, Vogel A, Keilmann A, Bohnert A, Mueller S, Evaluation of auditory development in infants and toddlers who received cochlear implants under the age of 24 months with the LittlEARS® Auditory QuestionnaireInternational Journal of Pediatric Otorhinolaryngology 2010 74(10):1149-55.10.1016/j.ijporl.2010.07.00320688403 [Google Scholar] [CrossRef] [PubMed]
[13]. Wang L, Sun X, Liang W, Chen J, Zheng W, Validation of the Mandarin version of the LittlEARS® Auditory QuestionnaireInternational Journal of Pediatric Otorhinolaryngology 2013 77(8):1350-54.10.1016/j.ijporl.2013.05.03323806742 [Google Scholar] [CrossRef] [PubMed]
[14]. Waltzman SB, Roland JT, Cochlear implantation in children younger than 12 monthsPediatrics 2005 116(4):e487-93.10.1542/peds.2005-028216199675 [Google Scholar] [CrossRef] [PubMed]
[15]. Tait ME, Nikolopoulos TP, Lutman ME, Age at implantation and development of vocal and auditory preverbal skills in implanted deaf childrenInternational Journal of Pediatric Otorhinolaryngology 2007 71(4):603-10.10.1016/j.ijporl.2006.12.01017239961 [Google Scholar] [CrossRef] [PubMed]
[16]. Schramm B, Bohnert A, Keilmann A, Auditory, speech and language development in young children with cochlear implants compared with children with normal hearingInternational journal of Pediatric Otorhinolaryngology 2010 74(7):812-19.10.1016/j.ijporl.2010.04.00820452685 [Google Scholar] [CrossRef] [PubMed]
[17]. Anderson I, Weichbold V, D’Haese PS, Szuchnik J, Quevedo MS, Martin J, Dieler WS, Phillips L, Cochlear implantation in children under the age of two-what do the outcomes show us?International Journal of Pediatric Otorhinolaryngology 2004 68(4):425-31.10.1016/j.ijporl.2003.11.01315013608 [Google Scholar] [CrossRef] [PubMed]