Correspondence: ‘Influenza as a Cause of SIADH Related Hyponatremia’
Takahiko Nagamine1
1 Department of Emergency Medicine, Sunlight Brain Research Center, Hofu, Yamaguchi, Japan.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Takahiko Nagamine, 4-13-18 Jiyugaoka, Hofu, Yamaguchi, Japan.
E-mail: tnagamine@outlook.com
Dear Editor,
I read with great interest the article by Gaglani B et al., reporting a patient of Syndrome of Inappropriate Antidiuretic Hormone Secretion (SIADH) caused by influenza infection [1]. SIADH is associated with pulmonary infection, but rarely with influenza virus [1-3]. I agree with the interesting aspect of this case. I would like to comment some speculated pathogenesis, because I recently experienced an elderly patient who presented with severe symptomatic hyponatremia caused by influenza-induced SIADH.
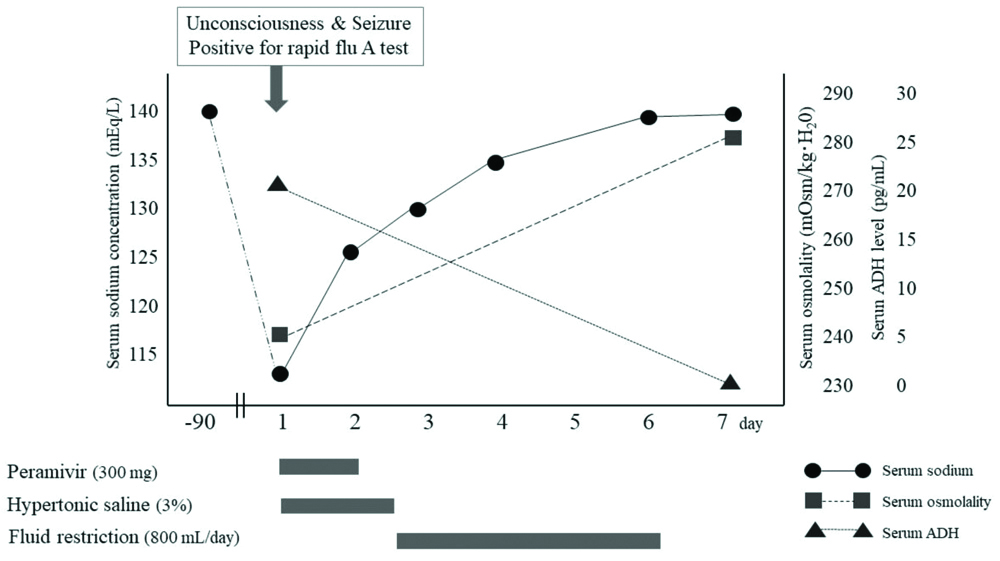
A 92-year-old woman was transferred to the emergency department because of non-productive cough and gradual decline in mental status. She had been in good health until she caught cold a few days ago. She did not receive any influenza vaccination in this season. While in the emergency room, she was noted to have generalised tonic-clonic seizures due to severe hyponatremia of 113 mEq/L. Rapid flu test was positive for influenza type A. Laboratory evaluation indicated plasma osmolality which was 240 mOsm/kg H20, whereas urine osmolality was 416 mOsm/kg H20. The plasma Antidiuretic Hormone (ADH) concentration markedly increased to 22.3 pg/mL even though there was severe hyponatremia. These findings were consistent with SIADH. Peramivir 300 mg was administered for influenza, and 3% hypertonic saline at 20~40 mL/hour with frequent monitoring of serum sodium levels with a sodium correction of less than 10 mEq/L in 24 hours [Table/Fig-1]. In this patient, symptoms associated with hyponatremia emerged just with influenza infection, and successful correction of sodium levels to normal range with peramivir treatment and hypertonic saline might have led influenza infection to cause SIADH.
Clinical course; change in the patient’s serum sodium levels.
Main pathogenesis is thought to be the secretion of inflammatory cytokines. These in turn strongly stimulate hypothalamic-pituitary-adrenal axis. The latter probably stimulate parvocellular and magnocellular arginine vasopressin neurons, resulting in secreting more ADH. Basic researches have indicated that inflammasomes induced by infection produce active Interleukin (IL)-1β and IL-6 that stimulate the secretion of ADH from the posterior pituitary gland. These multi-protein complexes can cause brain cells to low osmolality. Cell swelling with hypo-osmotic environment activates the release of IL-1β and IL-6, which increase the production of ADH leading to more profound hyponatremia, establishing a vicious circle [4]. Clinically, Hodax JK et al., have reported a case of both systemic juvenile idiopathic arthritis and SIADH successfully treated with tocilizumab, an IL-6 receptor antibody, that inhibits IL-6 activity [5]. When influenza infection stimulate the production of cytokines, ADH secretion may increase, resulting in SIADH.
There is no published data regarding the actual incidence of SIADH associated with influenza. Clinicians should be aware of the possibility of influenza-induced SIADH to allow for accurate diagnosis and treatment of this condition. Further studies are needed to elucidate the precise mechanism of influenza-induced SIADH basically and its incidence in clinical practice.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Aug 28, 2019
Manual Googling: Oct 22, 2019
iThenticate Software: Oct 28, 2019 (14%)
[1]. Gaglani B, Gupta S, Chavez O, Libardo R, Influenza as a cause of SIADH related hyponatremia: A case reportJ Clin Diagn Res 2017 11(5):OD10-11.10.7860/JCDR/2017/25785.979728658832 [Google Scholar] [CrossRef] [PubMed]
[2]. Mifsud S, Zammit MA, Casha R, Fsadni C, Influenza A: Another cause of SIADH?BMJ Case Rep 2018 pii:bcr-2018-22615410.1136/bcr-2018-22615430337286 [Google Scholar] [CrossRef] [PubMed]
[3]. Pathak R, Khanal A, Poudel DR, Karmacharya P, Down with the Flu: Hyponatremia in a patient with influenzaN Am J Med Sci 2015 7(5):227-28.10.4103/1947-2714.15748826110135 [Google Scholar] [CrossRef] [PubMed]
[4]. Kim JH, Park JH, Eisenhut M, Yu JW, Shin JI, Inflammasome activation by cell volume regulation and inflammation-associated hyponatremia: A vicious cycleMed Hypotheses 2016 93:117-21.10.1016/j.mehy.2016.05.01827372869 [Google Scholar] [CrossRef] [PubMed]
[5]. Hodax JK, Bialo SR, Yalcindag A, SIADH in systemic JIA resolving after treatment with an IL-6 inhibitorPediatrics 2018 141(1):pii:e2016417410.1542/peds.2016-417429242269 [Google Scholar] [CrossRef] [PubMed]