Anomalous Morphology of Liver and Rare Variation of Ligamentum Teres
Rajani Singh1
1 Additional Professor, Department of Anatomy, AIIMS Rishikesh, Rishikesh, Uttarakhand, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Rajani Singh, Department of Anatomy, AIIMS Rishikesh, Veerbhadra Marg, Rishikesh-249203, Uttarakhand, India.
E-mail: nani_sahayal@rediffmail.com
Hypoplasia, absence or accessory lobes are common variations in liver. Anatomically liver is divided into right and left lobes by falciform ligament, fissure for ligamentum teres and fissure for ligamentum venosum. Ligament of teres is present in the free margin of falciform ligament and winds round the inferior border of liver to reach the fissure for ligamentum teres. During routine dissection of abdomen of a 75-year-old female cadaver fixed in 10% formalin, abnormal disposition of ligamentum teres together with variant morphology of liver on its anterior surface consisting of a curved depression and an elongated gap was observed. Ligamentum teres was attached to superior margin of curved depression 6 cm above the inferior margin of liver. It passed through elongated gap situated 2.5 cm above inferior border of liver. The fissure for ligamentum teres and quadrate lobe was normally present. There was no other abnormality in the liver. The depression and gap found on the anterior surface of liver may give false impression of abnormal cavity to a surgeon during laproscopic liver surgery and also it may lead to misinterpretation of radiographs. Though ligamentum teres is described to be less important yet its variant dispostion is important in various therapeutic and diagnostic procedures.
Accessory lobe, Falciform ligament, Laproscopic surgery
Case Report
During routine dissection of abdomen of a female cadaver 75-year-old fixed in 10% formalin for MBBS 1st year students of AIIMS Rishikesh in the Department of Anatomy, a liver was found having multiple variations in morphology and a variant structural organisation. These variations were observed: i) morphology of anterior surface of liver; and ii) anomalous disposition of ligamentum teres. A remarkable unusual depression on the anterior surface of liver 6 cm above inferior border of liver bordered by the anomalous gap 2.5 cm above inferior border of liver was observed [Table/Fig-1]. The width of the gap was larger in left side and progressively narrowed down towards right side. The extended rounded liver tissue has been separated from rest of liver body by varying width of gap. The liver tissue was terminated by right sided narrow gap.
Showing abnormal configuration of ligamentum teres, elongated gap and depression in liver.
GB: Gall bladder; D: Depression; LT: Ligamentum teres
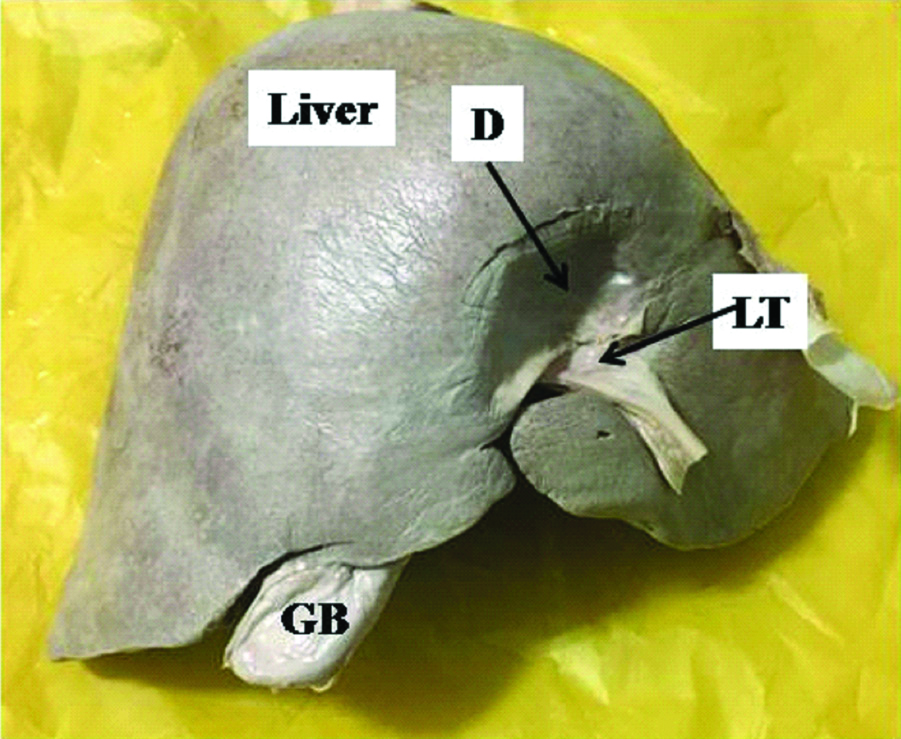
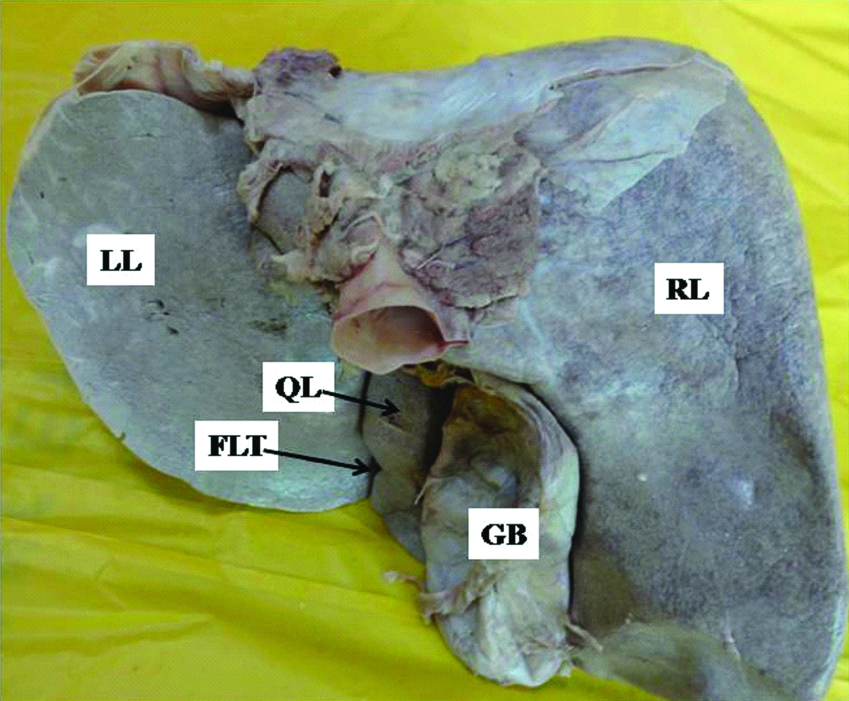
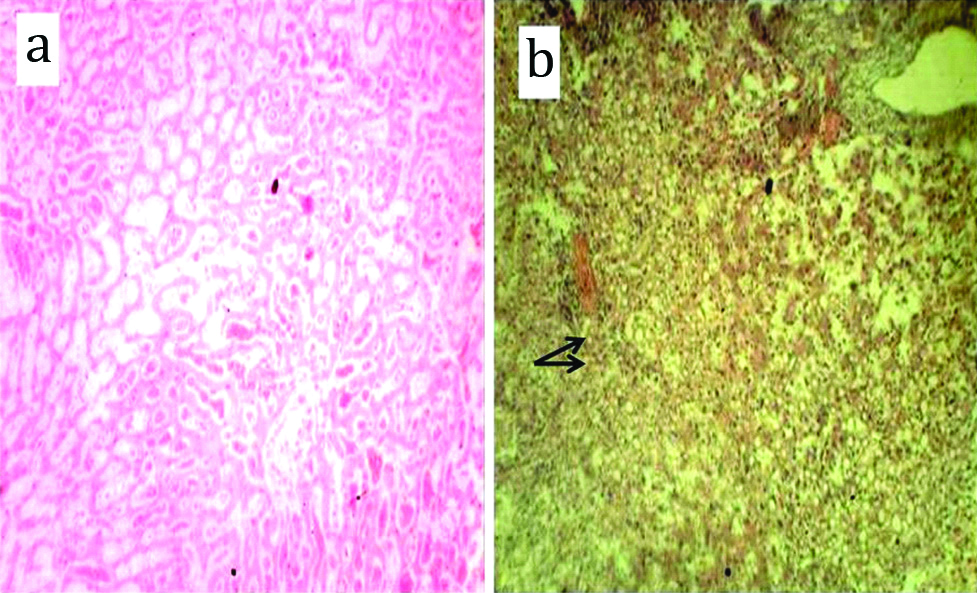
Ligamentum teres was attached to superior margin of anomalous depression [Table/Fig-1]. The ligamentum teres was passing through the wider part of gap to appear on visceral surface in place of normally passing over inferior margin to enter the floor of fissure for ligamentum teres. Fissure for ligamentum teres and quadrate lobe were normally present [Table/Fig-2]. Histological slides stained with haematoxylin and eosin prepared from depression when compared with normal liver tissue revealed fatty infiltration [Table/Fig-3,4]. The normal architecture of the liver is disturbed and hepatocytes are filled with fat cells as is evident from normal liver tissue slide prepared.
Showing normal fissure for ligamentum teres and quadrate lobe.
LL: Left lobe; RL: Right lobe; QL: Quadrate lobe; FLT: Fissure for ligamentum teres; GB: Gall bladder
Showing: a) Normal histological slide of liver tissue prepared from normal liver present in Anatomy department; b) Histological slide of liver tissue from depression. (H&E stain -10x)
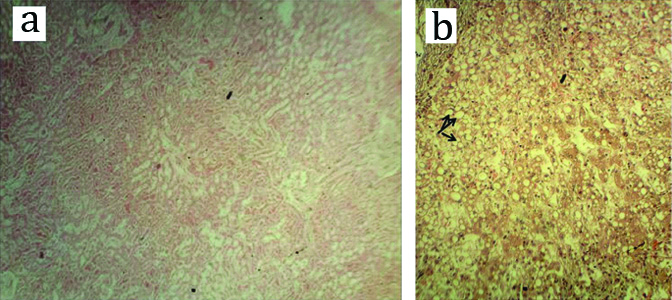
Showing: a) Normal histological slide of liver tissue prepared from normal liver present in Anatomy department; b) Histological slide of liver tissue from depression. (H&E stain -4x)
Discussion
Anatomically, liver is divided into right and left lobes by falciform ligament, fissure for ligamentum teres and fissure for ligamentum venosum. Ligamentum teres, which is present in the free margin of falciform ligament of liver and is known by different names like round ligament of the liver and Ligamentum teres hepatis. It is located in the free edge of falciform ligament and then courses through the fissure for the ligamentum teres travelling from inferior border of liver to the left end of porta hepatis. Ligamentum teres is remnant of fetal left umbilical vein. The left fetal vein remains patent for a month or two after birth and then it degenerates into ligamentum teres. In adults, paraumbilical vein forms a content of this ligament. Paraumbilical vein is an important part of portocaval anastomosis and affected in portal hypertension causing caput medusae [1]. The round ligament, a remnant of umbilical vein is attached to the umbilicus. It is an exemplary identification mark. According to some investigators, ligamentum teres is clinically unimportant. The ligamentum teres is frequently utilised for cannulation in various clinical conditions for diagnosis and prescribing treatment [2]. While attempting pneumo-peritoneum in supine position, some air enters the fissure for ligamentum teres which produces area of hyperlucency in radiographs [3]. Area of hyperlucency may not appear due to presence of elongated opening and may lead to misinterpretation of radiographs and misdiagnosis. Sometimes, when pressure is very high as in cirrhosis and portal hypertension, the ligamentum teres may again become patent causing recanalisation allowing blood to pass through it. So importance of this ligament cannot be ignored.
Fissure for ligamentum teres was observed to be absent by many authors [4-6]. Two case reports have been reported elaborating variations in ligamentum teres and fissure for ligamentum teres [7,8]. Both these cases reported formation of complete tunnel through which passed ligamentum teres to reach the visceral surface of liver. In case of Ebby S et al., the tunnel was observed on the diaphragmatic surface of the liver and quadrate lobe was absent [6]. However, in study by Satheesha Nayak B et al., the tunnel transmitting the ligamentum teres connected the anterior surface and inferior surface of the liver near the vicinity of fissure for ligamentum teres which was absent. Because of absence of fissure for ligamentum teres, quadrate lobe could not be delineated from left lobe of liver [7]. In present case, the ligamentum teres passed through elongated gap to reach the visceral surface. But fissure for ligamentum teres was present and so quadrate lobe could be delineated very well.
The liver is divided into right and left lobe by falciform and round ligament in the 2nd month of embryonic life. When this demarcation does not occur, it may lead to fusion of lobes of liver [9]. In study by Satheesha Nayak B et al., no demarcation of lobes was observed so it fused to form complete tunnel [7] whereas in our case the lobes could be well delineated on visceral surface but on anterior surface two lobes could not be demarcated. This may be due to incomplete fusion resulting from abnormal disposition of ligamentum teres.
Quadrate lobe was found to be absent in 3.7% of cases as described in literature. Fissure for ligamentum teres and quadrate lobe was observed to be absent in a case report [10]. But in this case, though there was abnormal disposition of ligamentum teres yet both fissure for ligamentum teres and quadrate lobe were well demarcated. Nayak SB et al., observed an accessory lobe in ligamentum teres near porta hepatis which may be misinterpreted as a lymph node [11].
Conclusion
Knowledge of abnormal elongated gap, depression and ligamentum teres in the liver observed in present study may surprise the surgeon during laparoscopic liver surgeries confusing them for pathological cavity. It may also cause misinterpretation of radiographs. Thus anomalies described in present study are of utmost use to surgeons in carrying out liver surgery, radiologists and anatomists.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? NA
For any images presented appropriate consent has been obtained from the subjects. NA
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Aug 07, 2019
Manual Googling: Sep 05, 2019
iThenticate Software: Oct 17, 2019 (8%)
[1]. Keith LM, Arthur FD, Clinically oriented anatomy 2006 5th edPhiladelphiaLippincott Williams & Wilkins:291 [Google Scholar]
[2]. Li XP, Xu DC, Tan HY, Li CL, Anatomical study on the morphology and blood supply of the falciform ligament and its clinical significanceSurg Radiol Anat 2003 26(2):106-09.10.1007/s00276-003-0184-014586564 [Google Scholar] [CrossRef] [PubMed]
[3]. Sanli EC, Kurtoglu Z, Kara A, Uzmansel D, Left sided-right portal joined round ligament with an anomaly of the intrahepatic portal veinSaudi Med J 2006 27(12):1897-900. [Google Scholar]
[4]. Aysin K, Ozcam G, Adnan O, Bulent B, Ahmet U, Ilke Ali G, A rare variation of round ligament of the liverInt J Anat Var 2009 2:262-64. [Google Scholar]
[5]. Abdullahi DZ, Tadros AA, Usman JD, Bello A, Absence of the left lobe of the liver in a cadaver: Case reportJ Med Trop 2010 12(1):45-47.10.4314/jmt.v12i1.69314 [Google Scholar] [CrossRef]
[6]. Ebby S, Ambike MV, Anatomical variation of ligamentum teres of liver- A case reportWebmed Cent Anat 2012 3(5):WMC003389 [Google Scholar]
[7]. Satheesha Nayak B, Kumar N, Srinivasa Rao S, Reghunathan D, Patil J, Swamy Ravindra S, Tunnel for ligamentum teres: A rare variation of the liverOA Case Reports 2013 2(10):9510.13172/2052-0077-2-10-806 [Google Scholar] [CrossRef]
[8]. Sato S, Watanabe M, Nagasawa S, Niigaki M, Sakai S, Akagi S, Laparoscopic observations of congenital anomalies of the liverGastrointest Endosc 1994 7(2):136-40.10.1016/S0016-5107(98)70345-1 [Google Scholar] [CrossRef]
[9]. Cho KC, Baker SR, Air in the fissure for ligamentum teres: New sign of intraperitoneal air on plain radiographsRadiology 1991 178(2):489-92.10.1148/radiology.178.2.19876131987613 [Google Scholar] [CrossRef] [PubMed]
[10]. Nayak SB, Mishra S, George BM, Shetty SD, Kumar N, Guru A, A peculiar liver with surgically and radiologically important variations: A case reportAnat Cell Biol 2013 46(1):82-84.10.5115/acb.2013.46.1.8223560240 [Google Scholar] [CrossRef] [PubMed]
[11]. Nayak SB, Kumar N, Sirasanagandla SR, Shetty SD, A mini accessory liver lobe in the fissure for ligamentum teres and its clinical significance: A case reportJ Clin Diagn Res 2013 7(11):2573-74.10.7860/JCDR/2013/6114.361524392404 [Google Scholar] [CrossRef] [PubMed]