Introduction
Augmented incidence of anxiety is associated with Coronary Artery Bypass Graft (CABG) compared to other surgeries; it affects the function of vital organ. Preoperative anxiety may persist after surgery and affects health related quality of life. Music therapy is found to have an impact on patient’s anxiety.
Aim
To find the effect of music therapy on hospital induced anxiety and Health Related Quality of Life (HRQoL) in patients after CABG.
Materials and Methods
Forty participants were recruited for the study, (age group 30-80 years) and randomised into two groups. The intervention group received music therapy along with cardiac rehabilitation and control group received cardiac rehabilitation alone once in a day. The primary outcome measure was Hospital Anxiety and Depression Score (HADS) was measured by a trained physiotherapist on preoperative day and postoperative day 2 and 7. The secondary outcome measures were SF-36 and 6 minute walk distance, measured by a trained physiotherapist on preoperative day and post operative day 7.
Results
HADS anxiety score showed significant difference within the intervention as well as control group, with p-value <0.05. The p-value of HADS depression component was <0.05 within each group. The values show that there is the reduction in both anxiety and depression in both groups nevertheless the p-value between the group was >0.05, which showed that there is no significant difference in HADS score between groups. The p-value of 6 MWT between the group was >0.05, but showed significant difference in control group. Physical component of SF-36 outcome did not show significant difference between the groups with p-value >0.05. Mental component of SF-36 did not established significant improvement between the groups. There was significant improvement in Physical component of SF-36 within the intervention group.
Conclusion
Both Phase I cardiac rehabilitation and music therapy has positive impact on anxiety, with music therapy being the most advisable.
Cardiac rehabilitation, Cardiac surgery, Coronary artery disease, Sedative music
Introduction
In India, CAD is a major causative factor for death which contributes more than 25% of death among general population [1]. Elevated Low Density Lipoproteins (LDL) and other factors such as change the permeability of vessel wall and generate inflammatory reactions which cause migration of monocytes to the site of inflammation. Monocytes then convert into macrophages, which is rich in cholesterol esters and free fatty acids thus infiltrate the coronary vessels and reduce the coronary blood flow to the cardiac muscles [2].
Preventive measures (diet modification, weight reduction, smoking cessation, cholesterol control, and control of diabetes and high blood pressure) and medications are used in the early stage of the disease [3]. In severe cases, CABG is employed to improve the circulatory compromise. Anxiety caused by fear of death, or level change in health conditions, stressful setting in the ICU, continuous monitoring by nurses, surrounding noise contributes to depression in post surgery patients. Patients undergo anxiety and depression after surgery due to factors like fear, pain, and lack of sleep can lead to reduced functional mobility and thereby reducing health related quality of life [4-8].
Health-Related Quality of Life (HRQOL) is an essential aspect in assessing the outcome of any surgical intervention. Various studies investigated the factors contributing to the reduction in quality of life after surgeries and found to have a relationship between psychosocial factors, demographic factors, and patient-related characteristics. Factors such as sex, diabetes mellitus, low ejection fraction, emotional response, and sleep along with cardiac symptoms affect the Health Related quality of life [9-11]. Cardiac rehabilitation is the standard of care after CABG. Cardiac rehabilitation consists of several definitions but all the systems of definition poses common focus on a multidisciplinary approach and it is mainly directed to patient’s physical, psychological and social wellbeing. Cardiac rehabilitation is the essential care after CABG with level Ia evidence [12].
Music therapy is considered as an alternative intervention to reduce the anxiety and without any side effects [13-16]. Sedative music has shown better improvement in patients undergone heart surgery [17]. Listening to music arouse activities in nucleus accumbens NAc and Ventral Tegmental Area (VTA) and releases dopamine. There is release of endorphins and reduction in catecholamine release which in turn lowers blood pressure [18]. A systematic review supports the effect of music therapy on anxiety in hospitalised persons [19]. Listening to music during bed rest after open-heart surgery has some effects on the relaxation system as regards s-oxytocin and subjective relaxations levels [20]. It has found to be cost effective and improves quality of life in patients. Music reduces environmental sounds and provides calm atmosphere thereby enhance psychological well-being [21,22].
In addition, few studies have made known that heart rate and respiratory rate improve, and oxygen consumption decreases after music therapy and found out that music therapy lowers the Heart Rate, Systolic Blood Pressure (SBP), and Mean Arterial Pressure (MAP) among patients undergoing CABG. Also, studies reveal that music therapy reduces the level of anxiety among patients undergoing cardiac surgery. Music therapy reduces pain perception and the dosage of analgesics administered during the intensive care unit and surgery unit stays of patients undergoing coronary artery surgery. Few studies showed that music therapy did not affect HR, SBP, Diastolic Blood Pressure (DBP), MAP, and anxiety among patients undergoing cardiac surgery [23-26].
The present authors found that there is a lack of evidence to provide music therapy as an adjunct in Phase I cardiac rehabilitation. The present authors assumed that music therapy along with the standard cardiac rehabilitation may enhance the quality of life and prevent or control anxiety. Therefore, conducted this study to evaluate the role of music therapy in the standard cardiac rehabilitation protocol for improving the health-related quality of life and reduce the anxiety.
Materials and Methods
Ethical clearance was obtained from Institutional Ethics Committee, Nitte Institute of Physiotherapy, Deralakatte, Mangalore (Ref:NIPT/IEC/Min//001/2016-2017/dated16-03-2017). Written permission to conduct this randomised controlled trial was obtained from the Head of the Cardiovascular Surgery Department and informed consent was obtained from patients. The study was prospectively registered in the clinical trials registry-India with the registration number of CTRI/2017/06/008927.
To calculate sample size the technique of estimation of sample size for paired t-test was used:
Where Δ is technically significant (0.7). α is the confidence level (5%) 1-α is power of the test (80%). SD is the standard deviation. The calculated sample size in each group was 17.
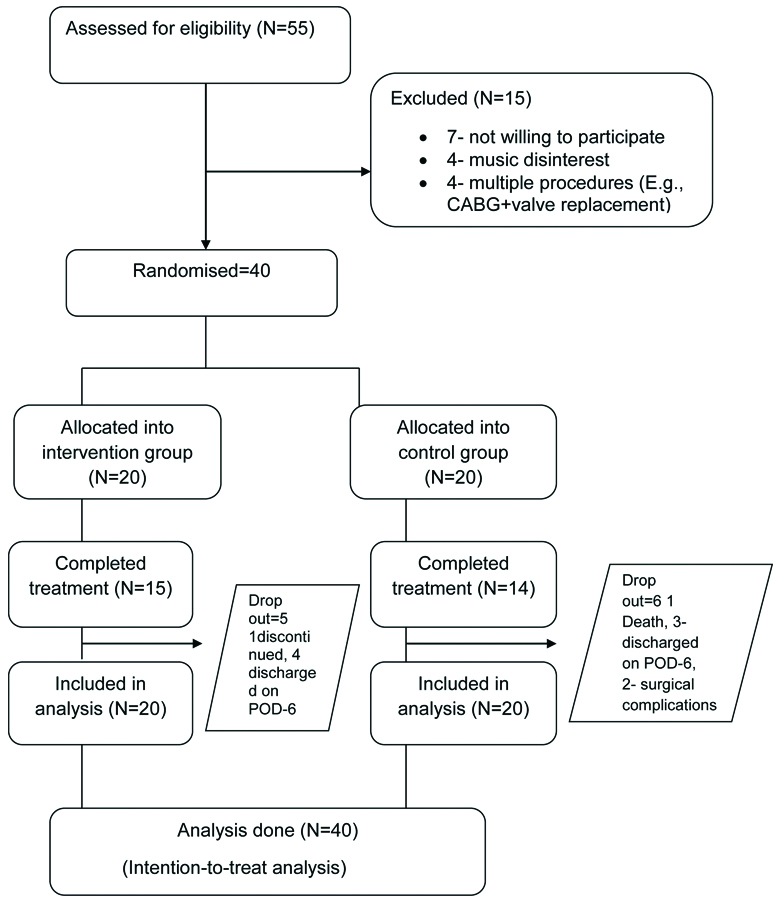
A sample size of 40 was considered and 40 sealed envelopes were made. Patients who were willing to participate and who met the inclusion criteria were randomised and allocated into two groups based on computer generated randomisation and sequentially numbered opaque sealed envelope method.
Inclusion and exclusion criteria are listed in [Table/Fig-1]. Based on inclusion-exclusion criteria baseline data of patients were obtained prior to intervention (including heart rate, respiratory rate, blood pressure, body mass index, rate of perceived exertion, 6 minute walk test, SF-36, Hospital Anxiety and Depression Scale, history regarding any other medical treatment and other health related conditions).
Inclusion and exclusion criteria.
| Inclusion criteria |
|---|
Subjects 30-80 years of age Both male and female patients CABG both on pump and off pump. Patients with LVEF <60% Patients with 2 grafts
|
| Exclusion criteria |
Patients who are having hearing impairments Patients after postoperative day 7, enter into phase II cardiac rehabilitation Patients with multiple procedures (E.g., CABG+ valve replacement) Patients who do not have interest in music Patient contraindicated to 6 minute walk test
|
Prior to the delivery of music the head-phones were sterilised with steriliser (ALCO SWAB® containing 70% alcohol- Isopropyl alcohol). Instructions were given prior to the intervention, instructed patient to inform the therapist whenever he/she felt discomfort in between the treatment session. During the delivery of sedative music the volume and pitch were adjusted according to patient’s comfort. Position of the patient during the music therapy was selected according to his/her comfort and cardiac the rehabilitation protocol. The sedative music without lyrics (60-80 beats per minute) was delivered for 20 minutes, once daily from the postoperative day-1 to postoperative day-7. This method of music therapy was delivered along with the Phase I cardiac rehabilitation programme [14,17,27].
All the patients in control group received Phase I cardiac rehabilitation from postoperative day 1 to 7 with the help of multidisciplinary rehabilitation team [28]. Patients received 20 minutes of cardiac rehabilitation in a day and the protocol was purely individualised. The progression of the treatment was decided based on patient’s condition. Hospital anxiety and depression score was taken on postoperative day 2 by trained outcome assessor (co-operation of the patient was ensured). All the outcome measures were taken by a trained therapist on postoperative day 7. Hospital anxiety and depression scores were assessed on the postoperative day-2 and day-7 by an independent physiotherapist who was blinded to group and intervention allocation. All other outcome measures such as 6 minute walk test and SF-36 questionnaire were taken on postoperative day 7 by the same therapist [29-31].
Patients were discharged on postoperative day 6, patients who were not shifted from coronary care unit till postoperative day 7, patients who died during the study and who refused to participate after surgery were considered to be drop out from the study. Patients were discharged based on the functional outcome on postoperative day 7. Intention-to-treat analysis was done after data collection and drop out patients were also included in the analysis.
Statistical Analysis
The data were analysed using SPSS software version 16.0. The demographic data like age, gender were analysed using descriptive statistics. To compare the outcome measures before and after interventions paired t-test used and when <2 time measurement were there Bonferroni was used. To compare the effectiveness of interventions between the groups ’independent sample t-test’ used. When data did not follow normal distribution Mann-Whitney U test was used to compare between group variables or Wilcoxon sign rank test to compare variables within the group. The p-value less than 0.05 was considered significant.
Results
A total of 55 patients were screened for eligibility during the period of August 2017 to March 2018. Out of these, 40 patients were randomly allocated into two groups [Table/Fig-2]. The participants’ characteristics are summarised in [Table/Fig-3].
Participant baseline characteristics by using descriptive statistics.
| Variable | Control group | Intervention group | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| Age (years) | 59.85 | 7.92 | 60.8 | 7.75 | 0.970 |
| Gender |
| Male | 6 | | 6 | | 0.634 |
| Female | 14 | | 14 | |
| BMI (kg/m2) | 25.18 | 5.11 | 23.11 | 3.65 | 0.264 |
| HR (beats per minute) | 75.65 | 13.488 | 75.55 | 12.194 | 0.486 |
| RR (breaths per minute) | 21.65 | 4.998 | 22.15 | 5.040 | 0.754 |
| RPE | 7.97 | 2.377 | 7.35 | 2.153 | 0.396 |
| Systolic BP (mmHg) | 122.0 | 0.396 | 123.5 | 11.821 | 0.421 |
| Diastolic BP (mmHg) | 78.500 | 8.750 | 79.500 | 8.255 | 0.522 |
| 6 MWT (distance in metres) | 264.55 | 85.398 | 276.85 | 116.670 | 0.706 |
Hospital Anxiety and Depression Score (HADS) Depression
[Table/Fig-4] shows that there was a significant difference in POD-7 in depression component between groups.
Between group comparison of depression component of HADS by using independent sample t-test.
| Intervention (n=20) | Control (n=20) | “t” | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| PRE | 5.53 | 2.722 | 5.53 | 2.47 | 0.046 | 0.964 |
| POD-2 | 4.87 | 2.446 | 6.29 | 3.099 | -1.44 | 0.159 |
| POD-7 | 1.80 | 1.373 | 3.39 | 3.025 | -2.469 | 0.020* |
*indicates significant
[Table/Fig-5] shows, within the intervention group at preoperative day and postoperative day 7, and postoperative day 2 and 7 the p-values were <0.05 and hence there was a difference in depression. In control group at POD 2 and POD7 there was a difference (p<0.05).
Within group comparison of depression component of HADS by using Bonferroni test.
| Group | Pairs | Mean difference | p-value |
|---|
| Intervention (n=20) | PRE & POD2 | 0.667 | 1 |
| PRE & POD7 | 3.73 | 0.002* |
| POD2 & POD7 | 3.067 | 0.001* |
| Control (n=20) | PRE & POD2 | -0.857 | 0.985 |
| PRE & POD7 | 1.5 | 0.303 |
| POD2 & POD7 | 2.357 | 0.001* |
*indicates significant
Hospital Anxiety and Depression Score (HADS) Anxiety
Comparisons of anxiety component of HADS score showed no difference [Table/Fig-6].
Between group comparisons of anxiety component of HADS by using Mann-Whitney U test.
| Intervention (n=20) | Control (n=20) | Z value | p-value |
|---|
| Median | IQR | Median | IQR |
|---|
| PRE | 7.56 | 5 to 12.75 | 7.50 | 7 to 9 | 1.561 | 0.49 |
| POD-2 | 6 | 4 to 9 | 6 | 4 to 9 | -0.175 | 0.92 |
| POD-7 | 1 | 0 to 3 | 1.50 | 0.00 to 5 | -0.859 | 0.31 |
[Table/Fig-7] shows significant difference between preoperative day and postoperative day 7 and postoperative day 2 and 7 (intervention group) and postoperative day 2 and 7 (control group) in HADS anxiety component for the same.
Within group comparison of anxiety component of HADS by using Bonferroni test.
| Group | Pair | Z value | p-value |
|---|
| Intervention (n=20) | PRE & POD2 | -1.201 | 0.230 |
| PRE & POD7 | -3.186 | 0.001* |
| POD2 & POD7 | -3.304 | 0.001* |
| Control (n=20) | PRE & POD2 | -1.057 | 0.294 |
| PRE & POD7 | -1.724 | 0.085 |
| POD2 & POD7 | -3.221 | 0.001* |
*Indicates significant
Six Minute Walk Test (6 MWT)
The [Table/Fig-8] shows 6 minute walk test comparison between groups. The obtained p-values were >0.05 hence there was no difference in 6 MWT.
Between group comparison of 6 MWT by using independent sample t-test.
| Intervention (n=20) | Control (n=20) | “t” value | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| PRE | 276.85 | 116.670 | 264.55 | 85.398 | 0.380 | 0.706 |
| POD-7 | 290.40 | 71.173 | 229.57 | 100.505 | 1.891 | 0.069 |
The [Table/Fig-9] shows a significant difference in 6 MWT in control group.
Within group comparison of 6 MWT by using independent sample t test.
| | Mean difference | p-value |
|---|
| Intervention (n=20) | PRE & POD7 | 12.93 | 0.684 |
| Control (n=20) | PRE & POD7 | 58.999 | 0.024* |
*indicates significant
SF-36
Physical component summary: The [Table/Fig-10] shows the values of between group comparison of physical component summary of SF-36 score. It indicates that there was no significant difference in SF-36 scores.
Between group comparisons of physical component of SF-36 score by using independent sample t-test.
| Intervention (n=20) | Control (n=20) | t value | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| PRE | 40.69 | 6.813 | 40.232 | 6.867 | 0.214 | 0.628 |
| POD-7 | 46.99 | 6.311 | 43.372 | 8.23 | 1.321 | 0.355 |
The [Table/Fig-11] shows significant difference in intervention group for the physical component summary of SF-36 score.
Within group comparisons of PCS component of SF36 score by using Bonferroni test.
| | Mean difference | p-value |
|---|
| Intervention (n=20) | PRE & POD7 | -5.904 | 0.006* |
| Control (n=20) | PRE & POD7 | -2.089 | 0.534 |
*indicates significant
Mental Component Summary
The [Table/Fig-12,13] shows comparison of mental component summary of SF-36 score within group by using Bonferroni test. The obtained p-value was >0.05 within the groups and between the groups, hence there is no significant improvement.
Comparison of mental component of SF-36 score between the group by using independent sample t test.
| Intervention (n=20) | Control (n=20) | t value | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| PRE | 37.65 | 9.63 | 39.88 | 6.270 | -0.869 | 0.123 |
| POD-7 | 42.68 | 9.70 | 42.71 | 9.508 | -0.009* | 0.854 |
Within group comparison by using Bonferroni test.
| | Mean difference | p-value |
|---|
| Intervention (n=20) | PRE & POD7 | -4.273 | 0.210 |
| Control (n=20) | PRE & POD7 | -2.001 | 0.550 |
The [Table/Fig-14] shows within group comparison of physical component score of SF-36 score. The obtained p-value was <0.05 in PF, RP, GH, VT and RE in intervention group and PF component in control group. It shows that there is a difference in these components.
Within group comparison of eight components of SF-36 score by using paired t-test.
| | PRE | POST | “t” | p-value |
|---|
| Mean | SD | Mean | SD |
|---|
| PF | Intervention | 46.667 | 23.503 | 65.332 | 22.635 | -2.441 | 0.029* |
| Control | 45.000 | 25.343 | 57.885 | 20.726 | -1.419 | 0.179 |
| RP | Intervention | 37.083 | 31.112 | 51.666 | 26.142 | -3.205 | 0.006* |
| Control | 44.196 | 16.710 | 46.875 | 18.467 | -0.442 | 0.666 |
| BP | Intervention | 47.066 | 26.477 | 65.000 | 32.958 | -1.757 | 0.101 |
| Control | 45.500 | 26.258 | 53.214 | 26.873 | -0.652 | 0.526 |
| GH | Intervention | 54.466 | 18.360 | 66.066 | 14.404 | -2.054 | 0.059* |
| Control | 60.500 | 17.986 | 65.000 | 17.119 | -0.706 | 0.493 |
| VT | Intervention | 51.250 | 15.345 | 59.166 | 16.781 | -2.588 | 0.021* |
| Control | 53.571 | 20.904 | 59.375 | 19.107 | -0.756 | 0.463 |
| SF | Intervention | 54.166 | 23.464 | 48.333 | 23.081 | 0.959 | 0.354 |
| Control | 55.357 | 26.726 | 43.750 | 21.230 | 1.247 | 0.234 |
| RE | Intervention | 33.889 | 27.180 | 57.778 | 28.948 | -3.170 | 0.007* |
| Control | 51.190 | 23.763 | 52.975 | 25.235 | -0.225 | 0.825 |
| PF | Intervention | 61.000 | 19.838 | 66.666 | 23.196 | -0.732 | 0.476 |
| Control | 55.357 | 19.361 | 71.428 | 20.232 | -2.337 | 0.036* |
Discussion
This study primarily aimed at finding the effect of music therapy on postoperative anxiety. HADS score showed significant difference within each groups nevertheless there was no significant difference in the outcome between the groups. This result correlates with the study by Heidari S et al., which showed music therapy reduces anxiety in CABG patients. They had made the patients listen to music for 30 minutes and assessed the cardiovascular indices and anxiety immediately after the intervention [32]. Their study does not provide any information regarding the effect of music therapy on anxiety until the day of discharge. However, in the index research, we clarified that the music therapy effects could prolong till the 7th day. For further clarification regarding the prolonged impact of music therapy along with cardiac rehabilitation follow-up measurement should be included after discharge which was beyond the scope of the present study.
Change in anxiety and depression scores within the control group may be due to the improvement in the functional status of the patient as a result of Phase I cardiac rehabilitation. These results correlate with the quasi-experimental study conducted by Ku SL et al., [33]. In general, music has positive impact on anxiety and depression along with cardiac-rehabilitation and is the most advisable.
The secondary aim of the study was to identify the effect of music on health-related quality of life. A 6 MWT was the objective outcome which did not show significant difference within the intervention group as well as between the groups where p-value is >0.05. The mean difference was more in the cardiac rehabilitation group, suggesting that 6 MWT did not show any significant improvement in experimental group, however, no adverse events were found during the intervention so it can be administered as a useful therapy in patients after CABG. There was no obvious clinically significant difference between groups in physical and mental component score. Physical component of SF-36 outcome did not show significant difference between the groups with p-value was >0.05. Mental component of SF-36 has been established, no significant improvement between the groups and within the group was seen. There was significant improvement in Physical component of SF-36 within the intervention group.
Comparison of cardiovascular indices after treatment showed that there is a significant difference in heart rate and rate of perceived exertion; there was no significant difference in respiratory rate and systolic and diastolic BP within each group and between groups. The results does not correlates with the findings of research done by Heidari S et al., which state that there is no significant difference among cardiovascular indices after music therapy in patients following surgery [32].
Effect of music on health-related quality of life along with Phase I cardiac rehabilitation has not been evaluated in any of the studies to date to the best of authors’ knowledge. Kurfirst V et al., demonstrated that there is an improvement in health-related quality of life after one year by using the SF-36 score in cardiac surgery patients, our study showed that there is an improvement in HRQOL in CABG patients till discharge from hospital (Phase I cardiac rehabilitation) [9]. The prolonged effect is out of scope of the present study. Future studies can be done to find out the prolonged-effect on the quality of life in CABG patients after music therapy. This is the first study evaluating the effect of music therapy on health related quality of life.
Limitation
Patient received sedative music which is not of patient’s choice. The follow-up treatment outcomes has not been considered in the study, the effect of music therapy on functional outcomes after discharge is not known. The sample strength is not sufficient to provide an accurate result.
Conclusion
In conclusion, the present authors demonstrate that music therapy during Stage-I cardiac rehabilitation is found to be effective to reduce postoperative anxiety and improve quality of life in CABG patients. The present authors also suggest that it’s an effective and harmless means for the management of hospital induced anxiety.
*indicates significant
*indicates significant
*Indicates significant
Author Declaration:
Financial or Other Competing Interests: No
Was Ethics Committee Approval obtained for this study? Yes
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Aug 27, 2019
Manual Googling: Sep 23, 2019
iThenticate Software: Oct 10, 2019 (10%)
[1]. Gupta R, Joshi P, Mohan V, Reddy KS, Yusuf S, Epidemiology and causation of coronary heart disease and stroke in IndiaHeart 2008 94(1):16-26.10.1136/hrt.2007.13295118083949 [Google Scholar] [CrossRef] [PubMed]
[2]. Barquera S, Pedroza-Tobías A, Medina C, Hernández-Barrera L, Bibbins-Domingo K, Lozano R, Moran AE, Global overview of the epidemiology of atherosclerotic cardiovascular diseaseArchives of Medical Research 2015 46(5):328-38.10.1016/j.arcmed.2015.06.00626135634 [Google Scholar] [CrossRef] [PubMed]
[3]. Rashid MA, Edwards D, Walter FM, Mant J, Medication taking in coronary artery disease: a systematic review and qualitative synthesisThe Annals of Family Medicine 2014 12(3):224-32.10.1370/afm.162024821893 [Google Scholar] [CrossRef] [PubMed]
[4]. Mullany CJ, Coronary artery bypass surgeryCirculation 2003 107(3):e21-22.10.1161/01.CIR.0000048896.72317.4912551881 [Google Scholar] [CrossRef] [PubMed]
[5]. Nesami MB, Shorofi SA, Jafari A, Khalilian AR, Tabari SZ, The relationship between stressors and anxiety levels after CABG in Sari, IranIranian Red Crescent Medical Journal 2016 18(5)10.5812/ircmj.2540727437127 [Google Scholar] [CrossRef] [PubMed]
[6]. Hewitt J, Psycho-affective disorder in intensive care units: a reviewJournal of Clinical Nursing 2002 11(5):575-84.10.1046/j.1365-2702.2002.00638.x12201884 [Google Scholar] [CrossRef] [PubMed]
[7]. Rodrigues HF, Furuya RK, Dantas RA, Dessotte CA, Ansiedade e depressão em cirurgia cardíaca: diferenças entre sexo e faixa etáriaEscola Anna Nery Revista de Enfermagem 2016 20(3)10.5935/1414-8145.20160072 [Google Scholar] [CrossRef]
[8]. Tully PJ, Baker RA, Depression, anxiety, and cardiac morbidity outcomes after coronary artery bypass surgery: a contemporary and practical reviewJournal of geriatric cardiology: JGC 2012 9(2):19710.3724/SP.J.1263.2011.1222122916068 [Google Scholar] [CrossRef] [PubMed]
[9]. Kurfirst V, Mokráček A, Krupauerová M, Čanádyová J, Bulava A, Pešl L, Health-related quality of life after cardiac surgery–the effects of age, preoperative conditions and postoperative complicationsJournal of cardiothoracic surgery 2014 9(1):4610.1186/1749-8090-9-4624618329 [Google Scholar] [CrossRef] [PubMed]
[10]. Rantanen A, Tarkka MT, Kaunonen M, Tarkka M, Sintonen H, Koivisto AM, Health-related quality of life after coronary artery bypass graftingJournal of advanced nursing 2009 65(9):1926-36.10.1111/j.1365-2648.2009.05056.x19694856 [Google Scholar] [CrossRef] [PubMed]
[11]. Kidd T, Poole L, Leigh E, Ronaldson A, Jahangiri M, Steptoe A, Health-related personal control predicts depression symptoms and quality of life but not health behaviour following coronary artery bypass graft surgeryJournal of Behavioral Medicine 2016 39(1):120-27.10.1007/s10865-015-9677-726341356 [Google Scholar] [CrossRef] [PubMed]
[12]. Niebauer J, Is there a role for cardiac rehabilitation after coronary artery bypass grafting? Treatment after coronary artery bypass surgery remains incomplete without rehabilitationCirculation 2016 133(24):2529-37.10.1161/CIRCULATIONAHA.116.02134827297345 [Google Scholar] [CrossRef] [PubMed]
[13]. Sendelbach SE, Halm MA, Doran KA, Miller EH, Gaillard P, Effects of music therapy on physiological and psychological outcomes for patients undergoing cardiac surgeryJournal of Cardiovascular Nursing 2006 21(3):194-200.10.1097/00005082-200605000-0000716699359 [Google Scholar] [CrossRef] [PubMed]
[14]. Comeaux T, Steele-Moses S, The effect of complementary music therapy on the patient’s postoperative state anxiety, pain control, and environmental noise satisfactionMedsurg Nursing 2013 22(5) [Google Scholar]
[15]. Allred KD, Byers JF, Sole ML, The effect of music on postoperative pain and anxietyPain Management Nursing 2010 11(1):15-25.10.1016/j.pmn.2008.12.00220207324 [Google Scholar] [CrossRef] [PubMed]
[16]. Fayazi S, Babashahi M, Rezaei M, The effect of inhalation aromatherapy on anxiety level of the patients in preoperative periodIranian Journal of Nursing and Midwifery Research 2011 16(4):278 [Google Scholar]
[17]. Voss JA, Good M, Yates B, Baun MM, Thompson A, Hertzog M, Sedative music reduces anxiety and pain during chair rest after open-heart surgeryPain 2004 112(1-2):197-203.10.1016/j.pain.2004.08.02015494201 [Google Scholar] [CrossRef] [PubMed]
[18]. Menon V, Levitin DJ, The rewards of music listening: response and physiological connectivity of the mesolimbic systemNeuroimage 2005 28(1):175-84.10.1016/j.neuroimage.2005.05.05316023376 [Google Scholar] [CrossRef] [PubMed]
[19]. Nilsson U, The anxiety-and pain-reducing effects of music interventions: a systematic reviewAORN Journal 2008 87(4):780-807.10.1016/j.aorn.2007.09.01318395022 [Google Scholar] [CrossRef] [PubMed]
[20]. Nilsson U, Soothing music can increase oxytocin levels during bed rest after open-heart surgery: A randomised control trialJournal of Clinical Nursing 2009 18(15):2153-61.10.1111/j.1365-2702.2008.02718.x19583647 [Google Scholar] [CrossRef] [PubMed]
[21]. Lippi D, di Sarsina PR, D’Elios JP, Music and medicineJournal of Multidisciplinary Healthcare 2010 3:13710.2147/JMDH.S1137821197362 [Google Scholar] [CrossRef] [PubMed]
[22]. Kemper KJ, Danhauer SC, Music as therapySouth Med J 2005 98(3):282-88.10.1097/01.SMJ.0000154773.11986.3915813154 [Google Scholar] [CrossRef] [PubMed]
[23]. Twiss E, Seaver J, McCaffrey R, The effect of music listening on older adults undergoing cardiovascular surgeryNursing in Critical Care 2006 11(5):224-31. [Google Scholar]
[24]. Emami Zeydi A, Jafari H, Khani S, Esmaeili R, Gholipour Baradari A, The effect of music on the vital signs and SpO2 of patients after open heart surgery: a randomized clinical trialJournal of Mazandaran University of Medical Sciences 2011 21(82):73-82.10.1111/j.1478-5153.2006.00174.x16983853 [Google Scholar] [CrossRef] [PubMed]
[25]. Hatem TP, Lira PI, Mattos SS, The therapeutic effects of music in children following cardiac surgeryJornal de Pediatria 2006 82(3):186-92.10.2223/JPED.147316680285 [Google Scholar] [CrossRef] [PubMed]
[26]. Ciğerci Y, Özbayır T, The effects of music therapy on anxiety, pain and the amount of analgesics following coronary artery surgeryTurkish Journal of Thoracic and Cardiovascular Surgery 2016 24(1)10.5606/tgkdc.dergisi.2016.12136 [Google Scholar] [CrossRef]
[27]. Ashok A, Soman A, Efficacy of music therapy on hospital induced anxiety and health related quality of life in Coronary Artery bypass graft patients: Study protocol for a randomized controlled trialInt J Pharma Bio Sci 2018 9(2):68-72.10.22376/ijpbs.2018.9.2.b68-72 [Google Scholar] [CrossRef]
[28]. Babu A, Noone M, Haneef M, Naryanan S, Protocol-guided phase-1 cardiac rehabilitation in patients with ST-Elevation myocardial infarction in a rural hospitalHeart Views 2010 11(2):5210.4103/1995-705X.7320921187997 [Google Scholar] [CrossRef] [PubMed]
[29]. Stafford L, Berk M, Jackson HJ, Validity of the hospital anxiety and depression scale and patient health questionnaire-9 to screen for depression in patients with coronary artery diseaseGeneral Hosp Psychiatry 2007 29(5):417-24.10.1016/j.genhosppsych.2007.06.00517888808 [Google Scholar] [CrossRef] [PubMed]
[30]. ATS statement: guidelines for the six-minute walk test. ATS Committee on Proficiency Standards for Clinical Pulmonary Function LaboratoriesAm J Respir Crit Care Med 2002 166(1):111-17.10.1164/ajrccm.166.1.at110212091180 [Google Scholar] [CrossRef] [PubMed]
[31]. Brazier JE, Harper R, Jones NM, O’Cathain A, Thomas KJ, Usherwood T, Validating the SF-36 health survey questionnaire: new outcome measure for primary careBMJ 1992 305(6846):160-64.10.1136/bmj.305.6846.1601285753 [Google Scholar] [CrossRef] [PubMed]
[32]. Heidari S, Babai A, Abbasinia M, Shamali M, Abbasi M, Rezaei M, The effect of music on anxiety and cardiovascular indices in patients undergoing coronary artery bypass graft: a randomized controlled trialNursing and Midwifery Studies 2015 4(4)10.17795/nmsjournal3115726835471 [Google Scholar] [CrossRef] [PubMed]
[33]. Ku SL, Ku CH, Ma FC, Effects of phase I cardiac rehabilitation on anxiety of patients hospitalized for coronary artery bypass graft in TaiwanHeart & Lung 2002 31(2):133-40.10.1067/mhl.2002.12282011910388 [Google Scholar] [CrossRef] [PubMed]