Successful Transradial Coronary Angioplasty in a Patient with Dextrocardia
Suindu Keshari Narayan Dash1, Krishna Sekhar Patri2, Mantravadi Sai Sudhakar3
1 Consultant, Department of Cardiologist, Gleneagles Global Hospital, Lakdi Ka Pul, Hyderabad, Telangana, India.
2 Consultant, Department of Cardiologist, Gleneagles Global Hospital, Lakdi Ka Pul, Hyderabad, Telangana, India.
3 Consultant, Department of Cardiologist, Director Cath Lab, Gleneagles Global Hospital, Lakdi Ka Pul, Hyderabad, Telangana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Suindu Keshari Narayan Dash, Flat No. 104, Vishnu Sadan Apartment, Road No 3, Shanti Nagar Colony, Masab Tank, Hyderabad-500028, Telangana, India.
E-mail: suindu1978@gmail.com
Even though dextrocardia occurs rarely, these people have similar incidence of coronary artery disease like normal population. Because of unfamiliarity with the reverse anatomy transradial coronary angiography and angioplasty is seldom tried in these patients. Here the authors present a case report of successful transradial angiography and angioplasty in a patient with dextrocardia with myocardial infarction.
Coronary intervention, Drug eluting stent, Percutaneous transluminal
Case Report
A 49-year-old male with known dextrocardia presented to casuality with severe retrosternal chest pain with sweating for last 2 hours. Pain was radiating to right arm. He was having Type 2 DM for last 5 years.
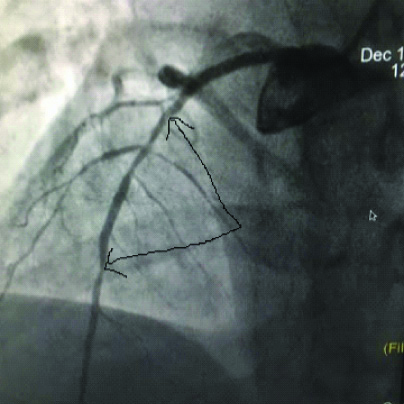
ECG showed acute anterior wall ST elevated myocardial infarction. He was thrombolysed with streptokinase. His chest pain was relieved. Chest X-Ray showed rightward displaced cardiac apex. His echocardiogram showed mirror image dextrocardia, regional wall motion abnormality in Left anterior descending artery territory with moderate Left ventricle dysfunction. Coronary angiogram was done from right radial approach. Left system was hooked with Tiger 5F catheter. Right coronary artery was hooked with JR 5 F diagnostic catheter. LAD and Left circumflex artery coronary arteries had separate origins. LAD showed long 80% stenotic lesion from proximal to distal segment. The dominant LCX and non-dominant RCA were normal [Table/Fig-1].
Antero-posterior cranial view showing LAD with significant long segment stenosis.
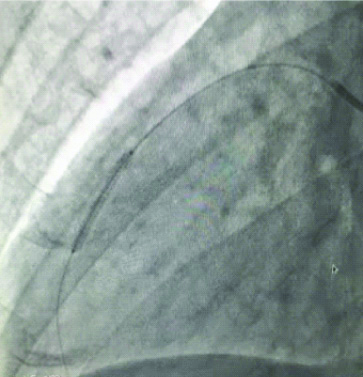
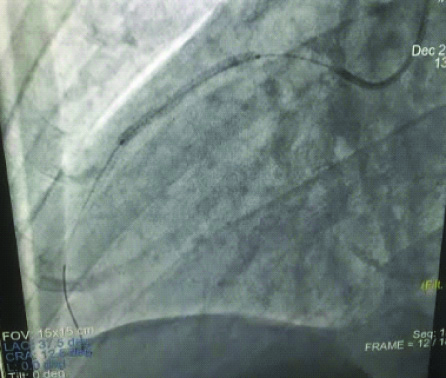
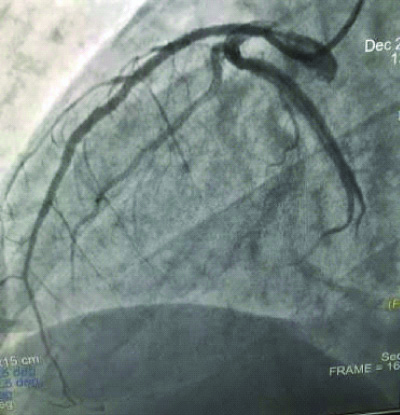
Percutaneous Transluminal Coronary Angioplasty (PTCA) with stenting to LAD was planned. Through right radial approach, LAD was hooked with EBU 3.0 5F guide catheter. The lesion was crossed with BMW guide wire. Then it was stented with 2 overlapping sirolimus Drug Eluting Stents (DES) 2.25×24 mm proximally and 2.5×37 mm distally with good result. Patient was discharged on third post-procedure day without any complication [Table/Fig-2,3 and 4].
Deployment of 2.25×24 mm sirolimus drug eluting stent in distal lad lesion.
Deployment of 2nd sirolimus drug eluting stent 2.5×37 mm overlapping the distal stent.
Final result after stent deployment.
Discussion
According to a previous study, general population and dextrocardia patients share the same risk of cardiac disease [1]. Performing percutaneous coronary intervention in these patients presents multiple challenges to the interventional cardiologist because of abnormal anatomy and unfamiliar radiological orientation [2]. In a patient with dextrocardia, it is very challenging to perform interventional procedures and coronary angiography because of its anatomical variation in alteration of heart and vessels and of rarity [3]. The portions of coronary ostia and vessels are mirror image of normal anatomy in situs inversus totalis dextrocardia. To avoid potential errors, selective cannulation of coronaries and interpreting properly along with modification in angiographic image acquisition, is necessary [4].
The first reported case of diagnostic cardiac catheterization in a patient with dextrocardia was done in 1973 by Hynes KM [1]. Moreyra AE et al., performed the first balloon angioplasty in a patient with dextrocardia and single-vessel CAD [2]. The first stent deployment in a patient with dextrocardia in situs inversus was performed by Patti G et al., in 1999 [5]. In 2005, Goel PK et al., described the advantage of the “double inversion technique” which could correct the unfamiliar angulated pictures of the coronary tree in dextrocardia into the familiar conventional angiographic pictures of a normally located heart [6].
Compared to normal heart, guide catheter, guide wire, balloon, including angiographic catheter, selection of interventional inventories and stent should be adjusted to the expected anatomy for Percutaneous transluminal coronary angioplasty in patients with mirror-image dextrocardia. In this case with some difficulty, multifunctional Tiger catheter could hook the left system for angiography but RCA was successfully hooked with Judkins Right 5.0 catheter. For PTCA, EBU Left 3.0 5F guide catheter was used, successfully to hook the LAD. Previous case reports have shown successful hooking of left coronary system with Judkins left, XB and EBU [7]. Judkins right catheter, multifunctional guiding catheters and extra support guiding catheters have been used for hooking right coronary artery. In present case, despite separate origin of LAD and LCX, we could manage to hook the left system with EBU Left 3.0 5F guiding catheter and successfully completed the procedure.
Percutaneous coronary intervention could be accomplished through trans-femoral and trans-radial route in patients with dextrocardia [8]. Prior case reports of PCI in MI patient with typical mirror image dextrocardia have been described through femoral access [9]. The first reported case of trans-radial case in stable angina patient with dextrocardia has been reported by Mc Donald JE et al in 2008 [10]. This is one of the few cases of dextrocardia with Myocardial Infarction (MI) where transradial angiography and angioplasty was done successfully through trans-radial route.
Conclusion
As trans-radial route may be convenient for the patient, this approach could be viewed as the prime route for vascular access for a patient of dextrocardia for coronary intervention.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: Aug 28, 2019
Manual Googling: Sep 09, 2019
iThenticate Software: Oct 07, 2019 (15%)
[1]. Hynes KM, Gau GT, Titus JL, Coronary heart disease in situs inversus totalisAm J Cardiol 1973 31(5):666-69.10.1016/0002-9149(73)90341-X [Google Scholar] [CrossRef]
[2]. Moreyra AE, Saviano GJ, Kostis JB, Percutaneous transluminal coronary angioplasty in situs inversusCathet Cardiovasc Diagn 1987 13:114-16.10.1002/ccd.18101302082953432 [Google Scholar] [CrossRef] [PubMed]
[3]. Blankenship JC, Ramires AF, Coronary arteriography in patients with dextrocardiaCathet Cardiovasc Diagn 1991 23:103-06.10.1002/ccd.18102302072070392 [Google Scholar] [CrossRef] [PubMed]
[4]. Jolly SS, Yusuf S, Cairns J, Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomized, parallel group, multicentre trialLancet 2011 377:1409-20.10.1016/S0140-6736(11)60404-2 [Google Scholar] [CrossRef]
[5]. Patti G, D’Ambrosio A, Di Sciascio G, Coronary stenting in patients with situs viscerum inversusG Ital Cardiol 1999 29:304-07. [Google Scholar]
[6]. Goel PK, Moorthy N, Trans-radial primary percutaneous coronary intervention in dextrocardia using double inversion techniqueJournal of Cardiology Cases 2013 8:e31-e33.10.1016/j.jccase.2013.03.01030546734 [Google Scholar] [CrossRef] [PubMed]
[7]. Galgani R, Gabos K, Sangani BH, Coronary angioplasty in a patient with dextrocardiaCathet Cardiovasc Diagn 1989 17(1):45-47.10.1002/ccd.18101701112524262 [Google Scholar] [CrossRef] [PubMed]
[8]. Agostoni P, Biondi-Zoccai CG, de Benedictis MI, Rigattieri S, Turri M, Radial versus femoral approach for percutaneous coronary diagnostic and interventional procedures; systematic overview and meta-analysis of randomized trialsJ Am Coll Cardiol 2004 44(2):349-56.10.1016/j.jacc.2004.04.03415261930 [Google Scholar] [CrossRef] [PubMed]
[9]. Yamazaki T, Tomaru A, Wagatsuma K, Kudo M, Baba J, Takikawa K, Percutaneous transluminal coronary angioplasty for morphologic left anterior descending artery lesion in a patient with dextrocardia: A case report and literature reviewAngiology 1997 48:451-56.10.1177/0003319797048005099158389 [Google Scholar] [CrossRef] [PubMed]
[10]. Macdonald JE, Gardiner R, Chauhan A, Coronary angioplasty via the radial approach in an individual with dextrocardiaInt J Cardiol 2008 131(1):e10-12.10.1016/j.ijcard.2007.07.03517935803 [Google Scholar] [CrossRef] [PubMed]