Adrenal Ganglioneuroma- A Rare Site Entity
Byna Syam Sundara Rao1, Vissa Shanthi2, Nandam Mohan Rao3, Bhavana Grandhi4, R Sujitha5
1 Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
2 Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
3 Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
4 Associate Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
5 Assistant Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Byna Syam Sundara Rao, Professor, Department of Pathology, Narayana Medical College, Chintareddy Palem, Nellore-524002, Andhra Pradesh, India.
E-mail: syam.byna@gmail.com
Ganglioneuroma is a rare lesion reported in many organs including adrenal gland. Adrenal ganglioneuroma is a rare benign sympathetic tumour which originates from Adrenal medulla. The adrenal gland tends to be unusual site but few cases have been reported in the literature. Here, the present authors report a case of Adrenal ganglioneuroma in 35-year-old male. He presented with complaints of diarrhoea and mild pain in abdomen. After abdominal CT scan, the patient underwent laparoscopic right adrenalectomy. Diagnosis was confirmed by histopathological examination as adrenal ganglioneuroma.
Adrenal gland, Benign, Sympathetic tumour
Case Report
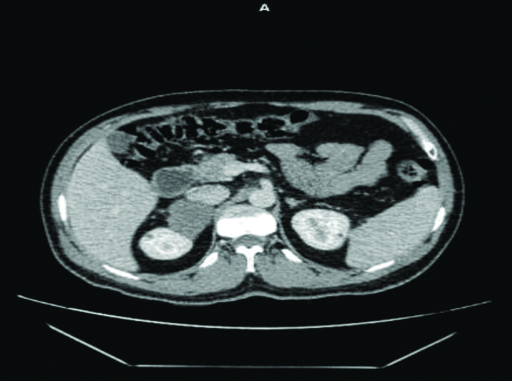
A 35-year-old male patient came to urology outpatient department with chief complaints of diarrhoea and mild pain in right side of abdomen since one month. He had no significant past medical history, Haematological investigations, liver function tests and renal function tests were normal. Ultrasound of abdomen revealed 7 cm × 5.5 cm well encapsulated mass noted in the superior aspect of adrenal gland. Contrast Enhanced Computer Tomography (CECT) Abdomen revealed large well defined smoothly marginated hypodense lesion involving the right adrenal gland measuring 6.2 cm × 5.3 cm × 4 cm [Table/Fig-1]. A biochemical profile revealed that serum cortisol was 9.69 μg/dL (6.02-18.4 μg/dL), 24 hour urinary metanephrine level was 34.37 μg/dL (24-96 mcg/24 hours) and non metanephrine 90.53 μg/dL (75-375 μg/24 hours). Routine urine examination and serum electrolytes revealed no abnormalities.
Contrast enhacned computer tomography shows large well defined hypodense lesin arising from right adrenal gland.
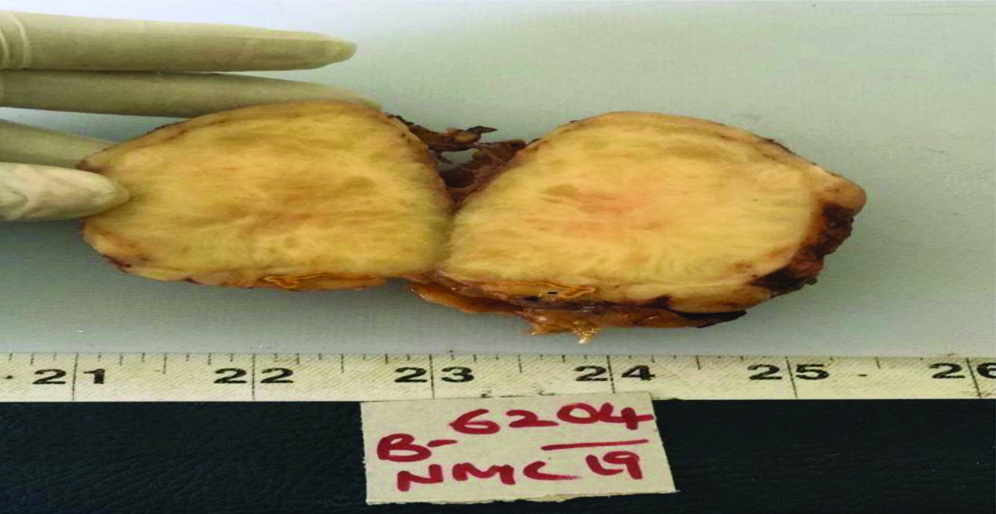
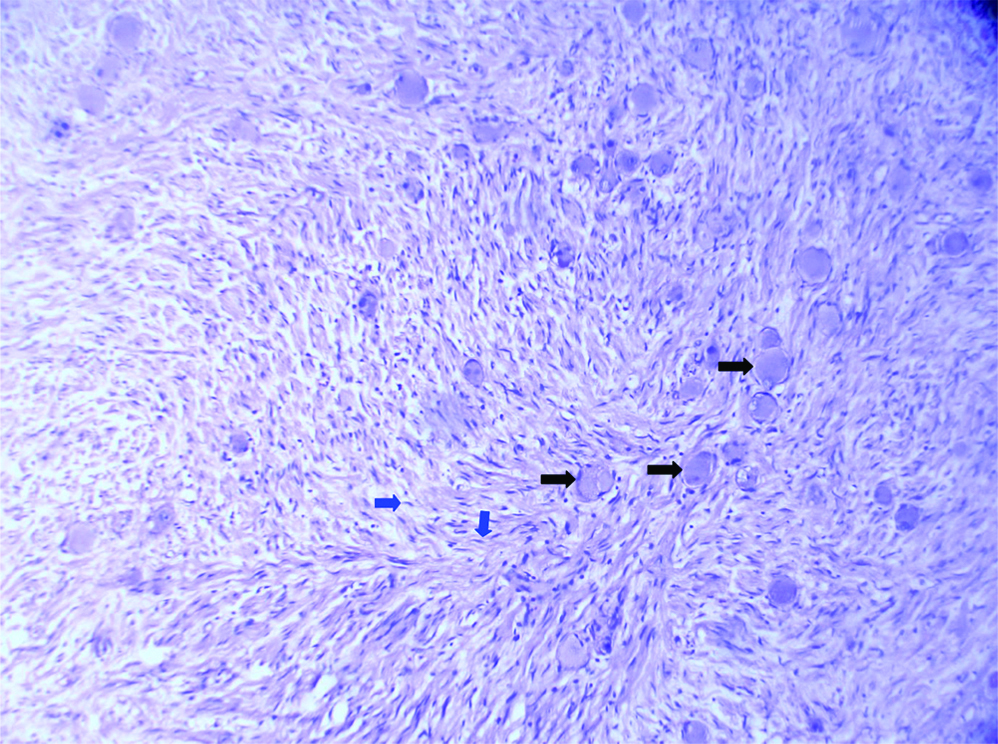
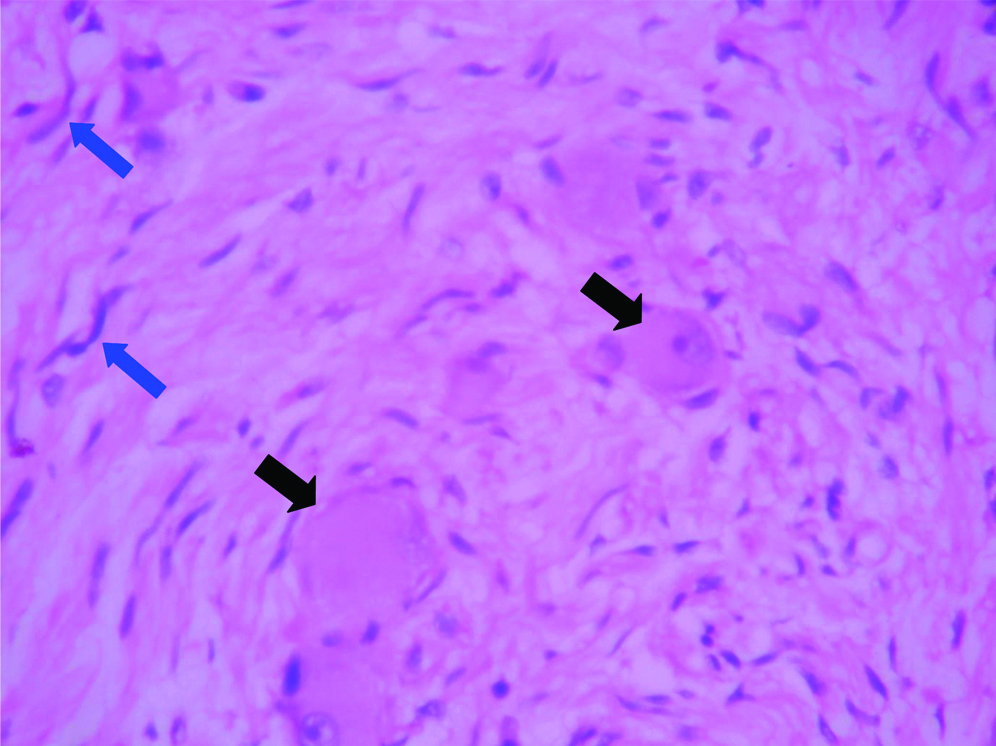
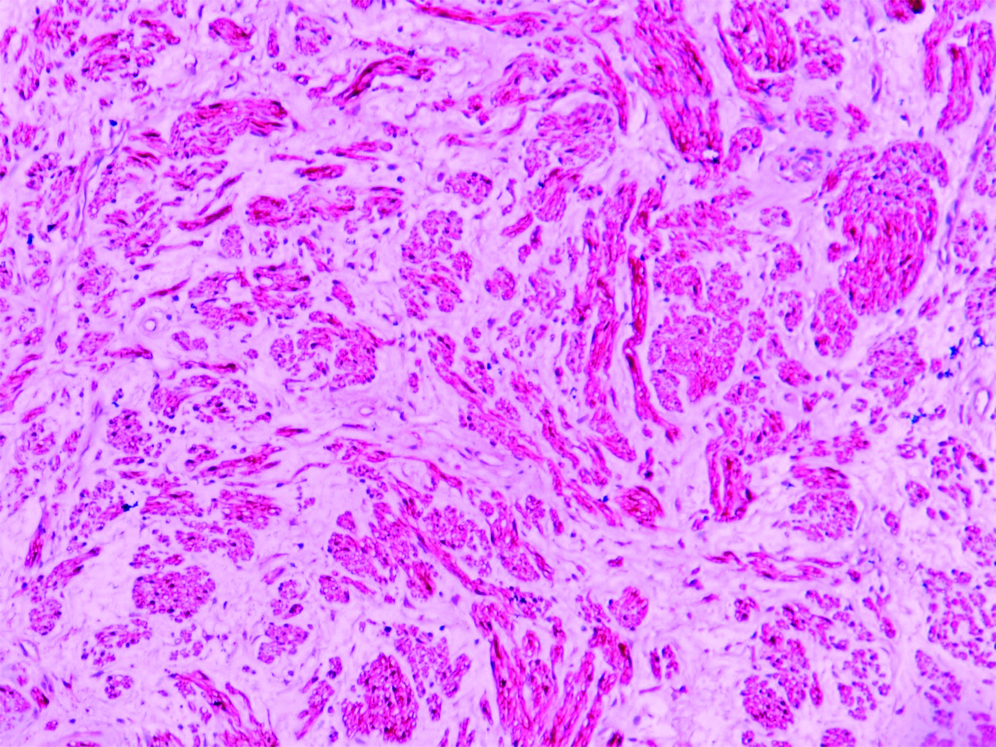
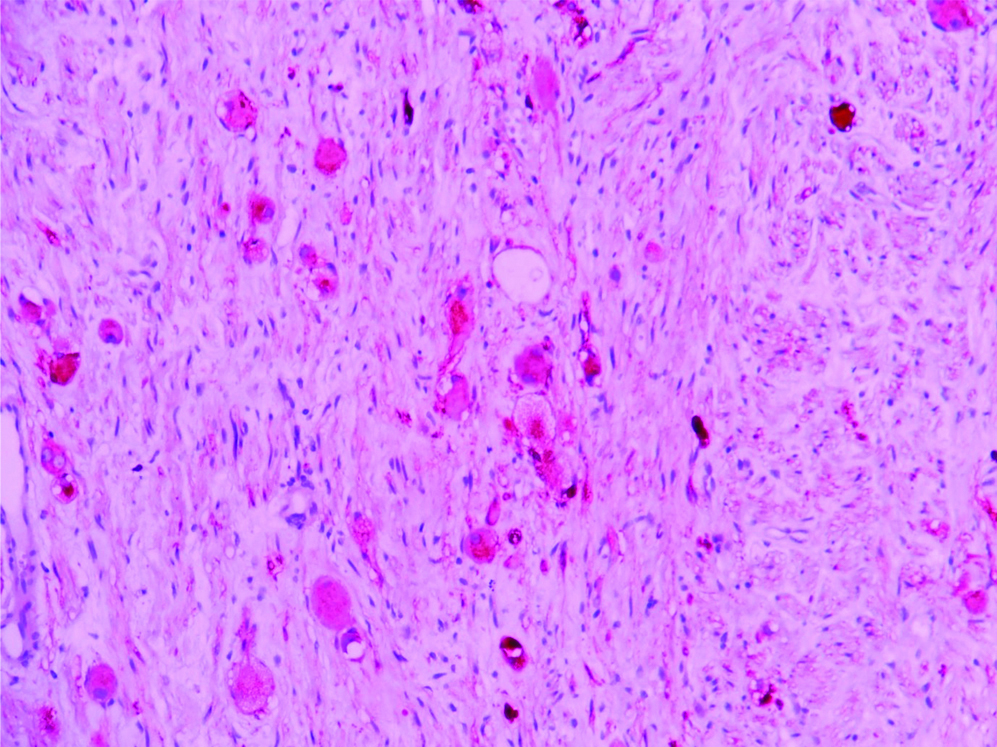
Differential diagnosis of atypical adrenal adenoma and ganglioneuroma was given in CECT abdomen. Right laparoscopic adrenalectomy was performed and specimen was sent to department of pathology for histopathogical examination. Macroscopic findings showed single grey white nodular mass along with perinephric fat measuring 8 cm × 7 cm × 4 cm. External surface was grey white nodular with grey brown areas. Cut section shows grey white circumsubsricbed nodule measuring 6 cm × 5 cm [Table/Fig-2]. Microscopic examination revealed structure of adrenal cortical parenchyma along with adjacent tumour tissue. Tumour tissue showed ganglion cells, Schwann cells and fibrous stroma [Table/Fig-3,4]. Ganglion cells were distributed in dispersed pattern within fibrous stroma. Ganglion cells have compact eosinophilic cytoplasm with distinct cell borders, single eccentric nucleus and prominent nucleoli. Schwann cells were arranged in small interlacing fascicles. These spindle cells exhibited wavy nuclei, eosinophilic cytoplasm and were separated by loose stroma. Differential diagnosis considered were neurofibroma, neuroblastoma and ganglioneuroblastoma based on microscopic features. On immunohistochemistry tumour cells were positive for S-100 [Table/Fig-5] and ganglion cells were positive for Synaptophysin [Table/Fig-6]. Postoperative state was uneventful and 3 months follow-up showed good recovery.
Gross picture shows cut section of specimen with tumour nodule measuring 6×5 cm.
Microscopic examination shows (100X) (H&E stain) schwann cells and ganglion cells in fibrous stroma. Schwann cell (blue arrow) and ganglion cell (black arrow).
Microscopic examination shows (400X) (H&E stain) schwann cells (blue arrow) and ganglion cells (black arrow) in fibrous stroma.
Shows schwann cells are positive for S-100 (IHC, 100X).
Shows multifocal ganglion cells are positive for Synaptophysin (IHC, 100X).
Discussion
Ganglioneuroma is a rare benign differentiated tumour which originates from the primitive neural crest cells and is composed of Schwann cells and ganglion cells [1]. They are rarely found in the adrenal gland [1,2]. Ganglioneuroma are usually located in posterior mediastinum, retroperitoneum, neck, adrenal glands and the region of the paravertebral sympathetic plexus. Adrenal ganglioneuroma is an infrequent slow growing neoplasm accounting for 20-30% all of ganglioneuroma [3]. Ganglioneuromas of posterior mediastinum and retroperitoneum are seen in children and younger people, however, Adrenal ganglioneuroma occurs commonly in the 4th to 5th decades of life [4]. This tumour is usually asymptomatic and hormonally silent even when the lesion is of substantial size [5]. Mixed hormone secretion results in symptoms like diarrhoea, virilization and hypertension. Histopathological examination is needed for definitive diagnosis of ganglioneuroma.
It is one of the members of family of a neurogenic tumour group that include benign Ganglioneuroma, malignant Gangiloneuroblastoma and malignant neuroblastoma. It differs with other neurogenic tumour by its benign nature [6]. Adrenal Ganglioneuroma commonly occurs in patient’s age ranging 10-40 years and it most commonly affects in right sided adrenal gland. According to literature few cases of Ganglioneuroma were reported in right adrenal gland [3].
Ganglioneuroma is a benign entity that originates from sympathetic nerve ganglion of neural crest cells or adrenal medulla. It occurs more frequently in young adults and some other studies revealed it may also be seen between the ages 40 and 50 years [7]. Ganglioneuroma is most frequently found in the retroperitoneum, posterior mediastinum and the involvement of adrenal gland is rare [8]. According to review literature only 15-30% all reported ganglioneuromas arise in the adrenal gland [9]. Macroscopic ganglioneuroma appear as encapsulated mass; firm in consistency, solid homogenous grey white to tan yellow. Cut surface show whorled appearance. Microscopic examination shows mature ganglion cells and schwann cells distributed among fibrous stroma [1]. The mature type is composed of mature Schwann cells, ganglion cells and perineural cells. Immunohisto chemistry staining of tumour cells of ganglioneuroma showed Schwann cells positive for S-100, vimentin and Synaptophysin positive for ganglion cells [10]. Neurogenic tumours are associated with sympathetic chain and commonly located in the mediastinum, neck, retroperitoneum and rarely in adrenal medulla. It has to be differentiated from neuroblastoma, neurofibroma and ganglioneuroblastoma. Histopathological examination of ganglioneuroma is required to exclude from other entities. Microscopy of the neurofibroma showing schwann cells, fibroblasts and perineural cells and lacks ganglion cell differentiation on microscopy. On microscopy presence of ganglion cells is distinguishing feature from neurofibroma. Microscopy of the neuroblastoma shows small blue round cells arranged in Homer wright pseudo rosettes pattern [6]. Cells are round to oval with high nuclear to cytoplasmic ratio and scanty cytoplasm. On microscopy Ganglioneuroma can be differentiated from neuroblastoma by the absence of blastemal component and later does not show ganglion cells and Schwann cells [6]. Microscopy of the gangiloneuroblastoma shows histological features similar to neuroblastoma except for presence of ganglion cells. Ganglioneuroblastoma shows a mixture of ganglion cells and undifferentiated tumour cells, whereas ganglioneuroma shows absence of undifferentiated tumour cells [6]. These tumours may undergo malignant transformation. Malignant peripherial nerve sheath tumour and Rhabdomyosarcoma may arise these tumours [11]. Adrenal ganglioneuroma is rare tumour and its presentation in adrenal gland is even rare the present authors report the case during presentation in the adrenal gland.
Conclusion
An adrenal ganglioneuroma is an uncommon benign tumour which originates from neural crest cells. An endocrine tests and imaging procedure are helpful for accurate diagnosis. Histopathological examination is gold standard for diagnosis. Adrenalectomy is the treatment of choice. Prognosis of adrenal ganglioneuroma is very good after surgical excision.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
PLAGIARISM CHECKING METHODS: [Jain H et al.]
Plagiarism X-checker: Jul 19, 2019
Manual Googling: Sep 06, 2019
iThenticate Software: Sep 26, 2019 (14%)
[1]. Geoerger B, Hero B, Harms D, Grebe J, Schelidhauer K, Berthold F, Metabolic activity and clinical features of primary ganglioneuromasCancer 2001 91(10):1905-13.10.1002/1097-0142(20010515)91:10<1905::AID-CNCR1213>3.0.CO;2-4 [Google Scholar] [CrossRef]
[2]. Erem C, Ucuncu O, Nuhoglu L, Cinel A, Cobanoglu U, Demirel A, Adrenal ganglioneuroma: report of a new caseEndocrine 2009 35(3):293-96.10.1007/s12020-009-9180-419367379 [Google Scholar] [CrossRef] [PubMed]
[3]. Yu Y, Zeshen W, Jiaha Z, HongWei W, Bentao S, Adrenal Ganglioneuroma: A rare case report and literature reviewUrol Nephrol Open Access 2017 5(5):01-02.10.15406/unoaj.2017.05.00185 [Google Scholar] [CrossRef]
[4]. Smylonas K, Schizas D, Economopoulous KP, Adrenal ganglioneuroma: What you need to knowWorld J Clin Cases 2017 5(10):373-77.10.12998/wjcc.v5.i10.37329085827 [Google Scholar] [CrossRef] [PubMed]
[5]. Allende DS, Hansel DE, Maclennan GT, Ganglioneuroma of the adrenal glandJ Urol 2009 182(2):714-15.10.1016/j.juro.2009.05.03619539319 [Google Scholar] [CrossRef] [PubMed]
[6]. Joshi W, Peripherial neuroblastic tumours: pathologic classification based on recommendations of international neuroblastoma pathology committee (modifications of himada classificationPediatr Dev Pathol 2000 3(2):184-89.10.1007/s10024005002410679039 [Google Scholar] [CrossRef] [PubMed]
[7]. Rhondeau G, Nolet S, Latour M, Braschi S, Gaboury L, Lacroix A, Clinical and biochemical features of seven adult adrenal ganglioneuromasJ Clin Endocrinol Metab 2010 95(7):3118-25.10.1210/jc.2009-277520427489 [Google Scholar] [CrossRef] [PubMed]
[8]. Jain M, Shubha BS, Sethi S, Banga V, Bagga D, Retroperitoneal ganglioneuroma: report of a case diagnosed by fine needle aspiration cytology, with review of literatureDiagn Cytopathol 1999 21(3):194-96.10.1002/(SICI)1097-0339(199909)21:3<194::AID-DC9>3.0.CO;2-B [Google Scholar] [CrossRef]
[9]. Felix EL, Wood DK, Das Gupta TK, Tumours of the retroperitoneumCurr Probl Cancer 1981 6(1):417-32.10.1016/S0147-0272(81)80011-6 [Google Scholar] [CrossRef]
[10]. Adas M, Koc B, Adas G, Ozulker F, Aydin T, Ganglioneuroma presenting as an adrenal incidentaloma: A case reportJ Med Case Rep 2014 8(1):01-05.10.1186/1752-1947-8-13124779851 [Google Scholar] [CrossRef] [PubMed]
[11]. Kimura S, Kawaguchi S, Wada T, Nagoya S, Yamashita T, Kikuchi K, Rhabdomyosarcoma arising from a dormant dumb bell ganglioneuroma of the lumbar spine: A case reportSpine 2002 27(23):513-17.10.1097/00007632-200212010-0001912461409 [Google Scholar] [CrossRef] [PubMed]