Carcinosarcoma of Uterus with Left Adnexal Metastasis: A Rare Case Report
Ruchi Agarwal1, Kulwant Singh2, Monika Gathwal3, Yudhvir Singh4, Swarn Kaur5
1 Associate Professor, Department of Pathology, Bhagat Phool Singh, Government Medical College for Women, Khanpur Kalan, Sonipat, Haryana, India.
2 Associate Professor, Department of Pathology, Bhagat Phool Singh, Government Medical College for Women, Khanpur Kalan, Sonipat, Haryana, India.
3 Associate Professor, Department of Pathology, Bhagat Phool Singh, Government Medical College for Women, Khanpur Kalan, Sonipat, Haryana, India.
4 Senior Resident, Department of Pathology, Bhagat Phool Singh, Government Medical College for Women, Khanpur Kalan, Sonipat, Haryana, India.
5 Professor and Head, Department of Pathology, Bhagat Phool Singh, Government Medical College for Women, Khanpur Kalan, Sonipat, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Ruchi Agarwal, Associate Professor, Department of Pathology, Bhagat Phool Singh, Government Medical College for Women, Khanpur Kalan, Sonepat-131305, Haryana, India.
E-mail: pg.ruchi@gmail.com
Carcinosarcomas are rare and aggressive tumour consisting of both carcinomatous and sarcomatous elements within same tumour. These tumours are supposed to arise from monoclonal proliferation of epithelial component. Carcinosarcoma of the uterus account for 2-5% of all uterine malignancies. They typically present with abnormal vaginal bleeding and may present with bloody discharge, abdominal pain or abdominal mass. Hereby a case report of a 60-year-old post-menopausal female presenting with painless lump abdomen progressively increasing in size has been described. Ultrasonography revealed a large solid-cystic mass in left adnexa. Total hysterectomy with bilateral salpingo-oophorectomy was performed. Histological examination of specimen revealed carcinosarcoma of uterus with left adnexal metastasis and left ovarian endometriotic cyst.
Biphasic tumour, Chondrosarcoma, Corpus uteri, Malignant mixed müllerian tumour, Ovarian cyst
Case Report
A 60-year-old post-menopausal female presented in Out Patient Department with complaint of a progressively increasing painless abdominal lump and fullness for two months. There was no history of any discharge or bleeding per vagina, weight loss or loss of appetite. General examination was unremarkable. Abdominal examination revealed a large lump palpable in umbilical, left iliac and suprapubic region. The lump was hard, non tender, smooth surface and non mobile. On per vaginum examination, a cystic mass approximately 20×18 cm felt in the left adnexal region. Also, uterus and ovaries are not palpable separately. Per speculum examination shows normal vagina and flushed cervix.
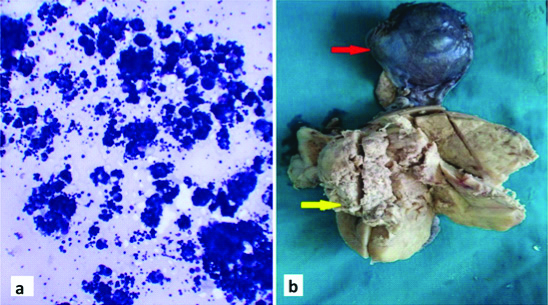
Hematological investigations of patient were within normal limits. Serum CA 125 level which was highly raised (122.7 U/mL). Radiological evaluation by USG showed a 17×14×12 cm mass lesion in pelvic cavity extending up to umbilicus. Mass showed 10×5 cm solid component along the posteromedial aspect and 7.5×3.5 cm cystic area along superolateral aspect. Mass is well out lined and well encapsulated. Solid component show mild internal vascularity. Both ovaries and uterus could not be separately visualised from the mass by transvaginal and transabdominal scanning. Cytological examination of ultrasound guided aspiration from mass revealed cellular smears with groups and overlapping clusters of atypical round to oval cells. Clinical diagnosis of carcinoma left ovary was made.
Patient underwent total abdominal hysterectomy with bilateral salpingo-oophorectomy, omentectomy and left pelvic lymph node dissection. On serial sectioning, a grey white, irregular, friable growth was identified filling the uterine cavity and invading inner half of the myometrium. Cervix, endocervical canal, right tube and ovary appeared grossly unremarkable. On opening, left adnexa shows a well-defined solid mass identified just medial to left lateral wall of uterus measuring 9×6 cm. Cut surface was grey white, friable with bluish glistening areas. Another already cut and collapsed cystic mass is identified adhering to solid mass and lateral uterine wall. Wall of cystic mass was reddish brown in colour and 0.2 to 0.5 cm thick [Table/Fig-1]. Left ovary and left tube could not be identified grossly. Piece of omentum measured 32×15 cm and grossly appeared unremarkable. Specimen labelled as left pelvic lymph node dissection was a single grey yellow fibrofatty soft tissue piece measuring 1.1×0.6×0.2 cm. Grossly no lymph nodes were identified.
(a) USG guided aspiration from mass showing groups and clusters of atypical cells (Leishman X40); (b) Photograph of hysterectomy along with bilateral salpingo-oophorectomy specimen showing a grey white growth filling the uterine cavity (yellow arrow) with a collapsed left adnexal cyst (red arrow).
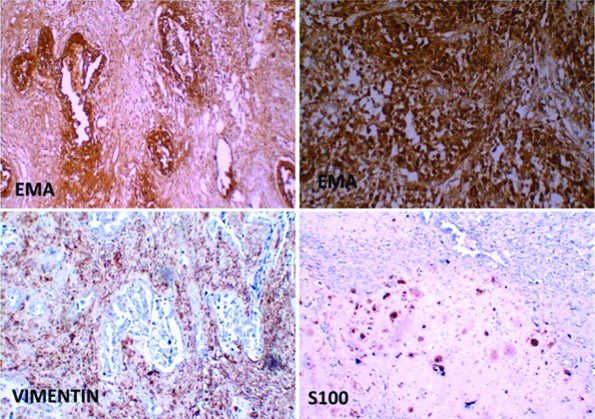
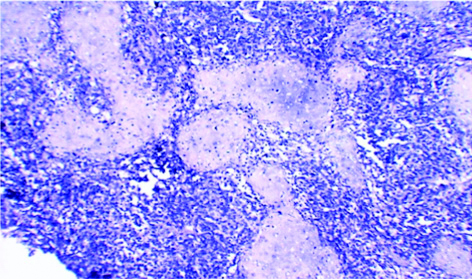
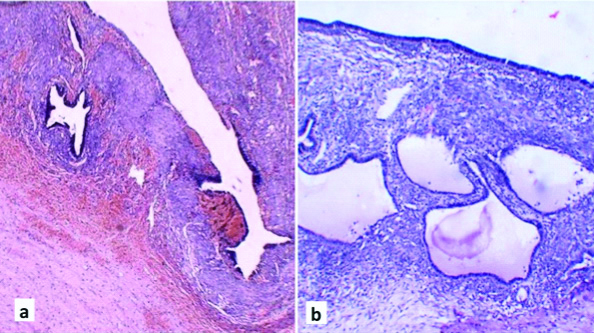
Haematoxylin and eosin stained sections from uterine growth revealed a biphasic tumour having sheets and acini of atypical epithelial cells showing pleomorphic large nucleus, prominent nucleoli and ill-defined pale cytoplasm. In between, sheets of atypical spindle cells and malignant cartilaginous tissue also seen. Areas of necrosis and frequent mitosis also identified. Epithelial component resembles endometrioid adenocarcinoma with diffuse sheets and acini of atypical epithelial cells. Myometrial invasion was seen up to inner half of myometrium [Table/Fig-2]. Left tube identified on microscopy and shows tumour infiltration in its serosal surface. Right ovary, right fallopian tube and omentum are free from tumour infiltration. No lymph nodes were identified in the tissue received. Immunohistochemistry performed on representative sections showed strong EMA positivity in carcinomatous areas. Sarcomatous component show weak positivity to both EMA and Vimentin. chondrosarcomatous areas show S-100 positivity [Table/Fig-3]. Sections studied from adnexal solid mass showing areas of adenocarcinoma surrounded by malignant cartilaginous component without any evidence of ovarian stroma [Table/Fig-4]. Sections examined from left adnexal cystic mass showing features of ovarian endometriotic cyst [Table/Fig-5]. Final diagnosis of uterine carcinosarcoma with left adnexal metastasis and left ovarian endometriotic cyst was given. In the present case, patient presented clinically due to large endometriotic ovarian cyst while she was later on diagnosed as a case of uterine carcinosarcoma with adnexal metastasis (FIGO stage IIIA). Postoperative period was uneventful. Patient was referred to another centre for radiotherapy and lost for follow-up.
Microphotograph from uterine growth showing: (a) areas of endometrioid carcinoma (H&E; x40); (b) areas of endometroid adenocarcinoma surrounded by chondrosarcomatous component (H&E; x100); (c) chondrosarcomatous component (H&E; x100), and (d) Myometrial invasion by carcinosarcoma (H&E; x20).

Immunohistochemistry show positivity in tumour cells for EMA, Vimentin and S100.
Microphotograph from adnexal solid mass showing areas of adenocarcinoma surrounded by malignant cartilaginous component (H&E; x40).
Microphotograph from left adnexal cystic mass showing features of ovarian endometriotic cyst (H&E; x20).
Discussion
Carcinosarcoma is also known as Malignant mixed mullerian tumour (MMMT), consists of both malignant epithelial and mesodermal components. It has highly malignant behaviour and generally has a poor prognosis [1]. It accounts for 2-5% of all uterine malignancies. This tumour shows preponderance in postmenopausal women [2]. Most patients presented between 5th-7th decades [3]. The median age of diagnosis is 62-67 years [4]. Previously, four main theories were suggested for origin of carcinosarcoma, namely: (i) collision; (ii) combination; (iii) conversion; and (iv) composition theory. However, now it is regarded as tumour of monoclonal origin being derived from single stem cell of epithelial origin [5,6].
They are classified into two histological subtypes based on their sarcomatous component, namely homologous or heterologous; homologous type- fibrosarcoma, endometrial stromal tumour or leiomyosarcoma, while heterologous type- rhabdomyosarcomas, chondrosarcomas, osteosarcomas and liposarcomas [5]. In both subtypes, the carcinomatous component is mainly composed of endometrioid, serous or clear-cell type adenocarcinoma. Homologous and heterologous carcinosarcomas arise with approximately equal frequencies [7].
Clinically, most patients present with abnormal vaginal bleeding that may be slight or profuse. Less frequently, bloody or watery discharge, weakness, weight loss, anorexia, lower abdominal pain or mass, urinary and gastrointestinal symptoms may be the presenting symptom [8].
Grossly, the tumour is usually polypoid or mass filling the endometrial cavity, with variable areas of necrosis, haemorrhage and cystic change. Microscopically, there is a diffuse admixture of both epithelial and mesodermal neoplastic components. Endometroid carcinoma is the most common epithelial component. However, clear cell, mucinous, serous or anaplastic pattern may be present. Endometrial stromal sarcoma and rhabdomyosarcoma are the most frequently occurring mesodermal component homologous and heterologous carcinosarcoma respectively [8].
FIGO staging of carcinosarcomas is same as for endometrial carcinoma. Local extension, lymphatic or haematogenous spread may occur. Extent of tumour and depth of myometrial invasion by the tumour is considered as the two most important prognostic indicators [8].
Carcinosarcoma must be carefully differentiated with other biphasic tumours during histopathological examination. Tumours with malignant epithelial with benign mesenchymal component (carcinofibroma), malignant mesenchymal component with benign epithelial component (adenosarcoma), and both components benign (adenofibroma, adenomyoma, and atypical polypoid adenomyoma) should be ruled out. Teratoma exhibits components of three germ layers but predominantly contain skin, appendages and neuroectodermal components. Carcinosarcomas, although biphasic, may reveal predominance of one component and need extensive sampling for differentiation from rhabdomyosarcoma and adenocarcinoma [8].
A combination therapy of surgery, radiotherapy and chemotherapy was used at many centres. Surgery including total abdominal hysterectomy and bilateral salpingo-oophorectomy with or without pelvic lymph node dissection is the choice of treatment. Adjuvant therapy with radiation therapy and/or chemotherapy is recommended depending on the clinical and pathological factors, including tumour stage, histological subtype, grade, lymph vascular invasion and distant metastasis [8]. The average five-year survival was 21% with most of the tumour related deaths occuring within 18 months of diagnosis [9].
Silverberg SG et al., studied 203 cases of endometrial carcinosarcoma and found that higher grade of epithelial tumour was associated with increased frequency of metastasis [1]. In an another study conducted by Iwasa Y et al., in 1998 on 25 patients, they reported 62.3% survival for stage I and 0% for Stages II-IV [10]. They concluded that stage appears to be vital independent prognostic indicator of survival of patients with uterine carcinosarcoma. Only few case reports were published in India in past [Table/Fig-6]. A study on 20 patients by Rajshekar SK et al., observed that median age of patients was 56 years and post menopausal bleeding was the most common presenting symptom [12]. They concluded that a negative endometrial biopsy does not rule out the diagnosis. Event free survival was 30% after median 16 months follow-up and poor prognosis is seen in patients with advanced-stage disease and myometrial invasion.
Review of cases of uterine carcinosarcoma from India.
| Authors | No. of cases | Year | Age (Years) | Clinical presentation |
|---|
| Barani K, Padmavathi R, [11] | 2 | 2013 | 68 | Abdominal pain, weight loss |
| 70 | Excessive vaginal discharge and abdominal pain |
| Rajshekhar SK et al., [12] | 20 | 2013 | 56 (mean) | Post menopausal bleeding |
| Bamniya J et al., [13] | 1 | 2015 | 65 | Post menopausal bleeding |
| Sarangi S et al., [14] | 1 | 2015 | 65 | Post menopausal bleeding |
| Rajshree DK [15] | 1 | 2016 | 55 | Abdominal lump+patient is known case of carcinoma cervix |
Conclusion
In present case, patient presented clinically with large endometriotic cyst which masked the clinical and radiologic evaluation of this rare uterine tumour. Early diagnosis and treatment can improve patient survival of this highly aggressive tumour. In all cases of high grade uterine tumours, extensive sampling and histological examination should be performed to rule out carcinosarcoma. Due to its low incidence, there is a need of multicentric trials of this rare neoplasm to develop a optimal treatment regime to achieve better outcome for patients.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
PLAGIARISM CHECKING METHODS: [Jain H et al.]
Plagiarism X-checker: Jul 13, 2019
Manual Googling: Jul 22, 2019
iThenticate Software: Sep 17, 2019 (11%)
[1]. Silverberg SG, Major FJ, Blessing JA, Fetter B, Askin FB, Liao SY, Carcinosarcoma (malignant mixed mesodermal tumor) of the uterus. A Gynecologic Oncology Group pathologic study of 203 casesInt J Gynecol Pathol 1990 9:01-19.10.1097/00004347-199001000-00001 [Google Scholar] [CrossRef]
[2]. Olah KS, Dunn JA, Gee H, Leiomyosarcoma have a poorer prognosis than mixed mesodermal tumours when adjusting for known prognostic factors the result of a retrospective study of 423 cases of uterine sarcomaBr J Obstet Gynecol 1992 99:590-94.10.1111/j.1471-0528.1992.tb13827.x1326319 [Google Scholar] [CrossRef] [PubMed]
[3]. Robboy SJ, Mutter GL, Prat J, Bentley RC, Russel P, Anderson MC, Robboy’s pathology of the female reproductive tract 2009 2ndedChinaChurchill Livingstone Elsevier:443 [Google Scholar]
[4]. Gadduci A, Cosio S, Romanini A, Genazzani AR, The management of patients with uterine sarcoma: A debated critical challengeCrit Rev Oncol Hematol 2008 65:129-42.10.1016/j.critrevonc.2007.06.01117706430 [Google Scholar] [CrossRef] [PubMed]
[5]. Jin Z, Ogata S, Tamura G, Katayama Y, Fukase M, Yajima M, Carcinosarcomas (malignant mullerian mixed tumors) of the uterus and ovary: A genetic study with special reference to histogenesisInt J Gynecol Pathol 2003 22:368-73.10.1097/01.pgp.0000092134.88121.5614501818 [Google Scholar] [CrossRef] [PubMed]
[6]. Ablen EC, Smit VT, Wessels JW, de Deleeuw WJ, Cornelisse CJ, Fleuren GJ, Molecular genetic evidence for the conversion hypothesis of the origin of malignant mixed mullerian tumoursJ Pathol 1997 183:424-31.10.1002/(SICI)1096-9896(199712)183:4<424::AID-PATH949>3.0.CO;2-L [Google Scholar] [CrossRef]
[7]. Spaziani E, Picchio M, Petrozza V, Briganti M, Ceci F, Di Filippo A, Carcinosarcoma of the uterus: A case report and review of the literatureEur J Gynaecol Oncol 2008 29:531-34. [Google Scholar]
[8]. Ali S, Wells M, Mixed Müllerian tumors of the uterine corpus: a reviewInt J Gynecol Cancer 1993 3:01-11.10.1046/j.1525-1438.1993.03010001.x [Google Scholar] [CrossRef]
[9]. Piver MS, Lurain JR, Uterine sarcomas: Clinical features and management. In: Coppleson M (ed.)Gynecologic Oncology. Fundamentals principals and Clinical practice 1981 Vol 2EdinburghChurchill Livingstone:608-18. [Google Scholar]
[10]. Iwasa Y, Haga H, Konishi I, Kobashi Y, Higuchi K, Kaysuyama E, Prognostic factors in uterine carcinosarcoma: a clinicopathologic study of 25 patientsCancer 1998 82(3):512-19.10.1002/(SICI)1097-0142(19980201)82:3<512::AID-CNCR13>3.0.CO;2-4 [Google Scholar] [CrossRef]
[11]. Barani K, Padmavathi R, Two rare cases of malignant mixed mullerian tumorInt J Pathol 2013 15(1) [Google Scholar]
[12]. Rajshekhar SK, Guruprasad B, Shakunthala PN, Rathod P, Devi U, Bafna UD, Malignant Mixed Mullerian tumour (MMMT) of uteruse-Cancer 2013 7:302(DOI:10.3332/ecancer.2013.302) [Google Scholar]
[13]. Bamniya J, Shah A, Dayal A, Kothari S, Shah M, A rare case of Malignant Mixed Mullerian tumour (MMMT) of uterusInt J Res Med 2015 4(3):64-68. [Google Scholar]
[14]. Sarangi S, Sarangi S, Mahata M, Mukherjee S, Datta J, Das T, Uterine malignant mixed mullerian tumour - revisited in newer lights: A case report from a tertiary care centreIJBR [Internet] 30 Sep.2015 [cited 3 Aug 2019] 6(9):743-46.10.7439/ijbr.v6i9.2517 [Google Scholar] [CrossRef]
[15]. Rajshree DK, A rare case of uterine carcinosarcoma in a patient who had received radiotherapy 14 years back for carcinoma cervixJ Gynecol 2016 1(3):00011410.23880/OAJG-16000114 [Google Scholar] [CrossRef]