Globally, second leading cause of death is cancer. Patients with cancer generally have a poor prognosis in developing countries, including India, because of lack of cancer awareness, delay in diagnosis and lack of patient affordable treatment services including targeted therapy, radiation therapy and chemotherapy [1]. The status report on the global burden of cancer worldwide by the International Agency for Research on Cancer using GLOBOCAN 2018 estimated 18.1 million newer cancer cases and 9.6 million cancer deaths in 2018 [2]. Particularly, breast cancer ranks second according to incidence of cancers in women in the world [2,3]. There is growing evidence that anaemia has an impact on treatment outcome, prognosis and survival of cancer patients.
Anaemia is an important and common problem adding substantial burden to the cancer patients besides affecting physical, functional, emotional well-being, and quality of life. It has negative impact on treatment outcome, prognosis and survival [4,5]. It has been reported that between 30-90% of patients with cancer have anaemia [6]. Literature suggests that Iron deficiency (ID) plays a major role in the pathogenesis of anaemia in cancer patients and has an estimated impact on 19–63 % patients of different cancer types [5]. In a meta-analysis anaemic patients had shorter survival time than those without anaemia. The overall estimated increase in risk was 65% (54-77% in patients with different types of malignant tumours) [6]. Iron Deficiency Anaemia (IDA) is diagnosed when Haemoglobin (Hb) levels are less than 13 g/dL in men and 12 g/dL in women according to World Health Organisation (WHO) limits for haemoglobin [7]. Chronic, tumour-related anaemia is diagnosed when Haemoglobin (Hb) levels are below 12 g/dL [8].
In this study we aimed to assess the prevalence of different types of cancers, frequency of breast cancer patients with respect to site of carcinoma, stage of carcinoma and receptor positivity and the frequency of cancer patient population with respect to pre-diagnosed haemoglobin levels.
Materials and Methods
Study Design and Participants
It was a cross-sectional study which was carried out for a two months period between September 2017 and October 2017 in a Tertiary cancer care hospital, City Cancer Centre, Vijayawada, Andhra Pradesh, India.
Ethical Consideration
The study protocol was approved by Institutional Ethics Committee of City Cancer Centre. All the participants were informed about study details and informed consent was obtained before the initiation of study. The protocol number was IEC/HCGCCC/333/ACD/05/17.
Inclusion and Exclusion Criteria
Inclusion criteria: The patients both males and females visited the hospital in two months specified period with age greater than 18-year-old. Patients laboratory data accompanied by haemoglobin levels prior to their diagnosis with cancer.
Exclusion criteria: Patients who were not willing to participate and patients with insufficient data were excluded.
Study Procedure
A total of 108 patients of different types of cancers were enrolled in two months period. Finally, 90 patients were recruited into the study based on inclusion criteria. The experimental study design is shown in [Table/Fig-1]. All the accessible data was analysed to estimate the frequency of different types of cancers in a tertiary cancer care hospital based on surgical pathology reports and Immunohistochemistry (IHC) reports. Based on surgical pathology reports the clinical grades of different cancer patients were performed according to the American Joint Committee on Cancer (AJCC) grading system. Grade I included (T1, N0, M0), Grade II included (IIA: T0-1, N1, M0 or T2, N0, M0 and IIB: T2, N1, M0 or T3, N0, M0) and Grade III included (IIIA: T0-2, N2, M0 or T3, N1-2, M0; IIIB: T4, N0-2, M0 and IIIC: any T, N3, M0). Grade IV the patients with metastases [6]. Most of the cases were diagnosed based on surgical pathology reports.
Study design, inclusion and exclusion of participants.
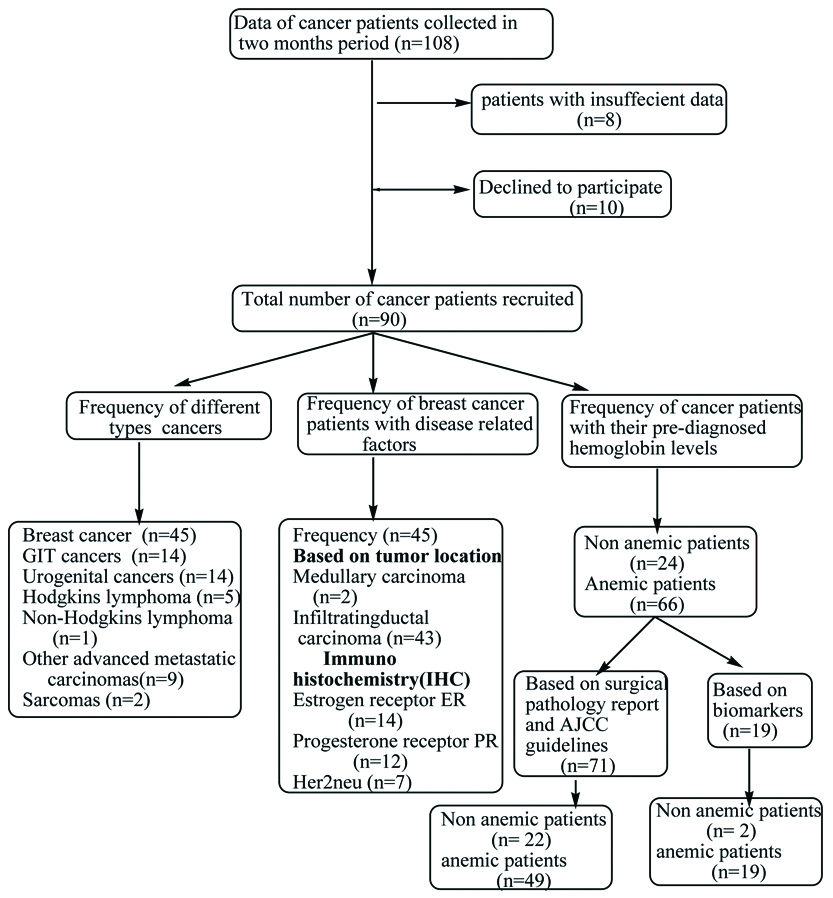
As the females with breast cancers account for the majority of the study (n=45, 50%). The data of breast cancer patients was assessed in detail to find the frequency of the disease based on surgical pathology reports, immunohistochemistry reports. Both, surgical pathology and immunohistochemistry diagnostic tests were performed in all breast cancer patients (n=45) and the reports of these diagnostic tests were used to diagnose the patients with breast cancer. Based on surgical pathology report the clinical grading of breast cancer patients was performed according to the American Joint Committee on Cancer (AJCC) grading system [4] and IHC reports of breast cancer patients included Estrogen Receptor (ER), Progesterone Receptor (PR), and Human Epidermal Growth Factor Receptor 2 (Her2-neu).
The collected data was also used to assess the frequency of pre-diagnosed haemoglobin levels to find out the frequency of anaemia in cancer patients. We defined Low pre-operative Haemoglobin (Hb) levels <12 g/dL found to be associated with a poor disease prognosis and increased morbidity and mortality rate as it shows correlation with nodal metastasis e.g., colorectal cancers, head and neck, ovarian carcinomas. The cancer patients were divided into two groups: anaemic patients group (Hb <12.0 g/dL) and the non-anaemic patients group (Hb ≥12 g/dL) based on the above definition.
Data Analysis
The collected data was described as analysed frequency of different cancers and the percentage of frequency.
Results
There were 90 patients included in this study. [Table/Fig-2] shows demographics of patient population and prevalence of various types of cancers. Females accounted for majority of study population. The frequency of various types of cancers patients based on the site of tumour occurrence. Breast cancer (n=45, 50%), gastrointestinal cancers (n=14, 16%), urogenital cancers (n=14, 16%), Hodgkin’s lymphoma (n=5, 6%), non-Hodgkin’s lymphoma (n=1, 1%), other advanced metastatic carcinomas (n=9, 10%), sarcomas (n=2, 2%). In our study, population of breast cancer patients was highly prevalent.
Demographics of patient population and prevalence of various types of cancers.
| Patient demographics | Frequency (Percent frequency) |
|---|
| Patients (n) | 90 (100) |
| Gender |
| Male | 19 (21.12) |
| Female | 71 (78.88) |
| Age |
| <65 years | 78 (86.66) |
| ≥65 years | 12 (12.2) |
| Primary tumour type |
| Breast cancer | 45 (50) |
| Gastrointestinal cancer | 14 (16) |
| Urogenital cancers | 14 (16) |
| Hodgkin’s lymphoma | 5 (6) |
| Non-Hodgkin’s lymphoma | 1 (1) |
| Other advanced metastatic carcinomas | 9 (10) |
| Sarcomas | 2 (2) |
As the breast cancer contributes half percentage of the study its clinical parameters were included in [Table/Fig-3]. In female breast cancer patients (n=45). The percent frequency of patients less than 65 years was found to be 84.4% while the percent frequency of patients greater than or equal to 65 years are found to be 15.5%. The surgical pathology report identifies tumour as medullary carcinoma or IDC. Based on the primary tumour type nodal involvement and metastasis scoring the patients were differentiated into Grades using standard AJCC guidelines, Grade-1 range (n=8, 17.7%), Grade-2 (n=34, 75.5%), Grade-3 (n=3, 6.66%). The Immunohistochemistry report gives information of expressed receptors on the tumours. The frequency distribution of hormonal receptor status was as follows: ER positive (n=4, 8.9%), PR positive (n=2, 4.4%), both ER and PR positive (n=10, 22.2%), human epidermal growth factor receptor 2 (Her-2-neu) positive (n=6, 13.3%). Both ER and Her-2-neu positive (n=1, 2.2%), hormonal receptor negative (n=22, 48.9%). The results indicate that frequency of patients diagnosed with IDC was high. In IDC patients, majority of patients were diagnosed in grade 2 IDC.
Frequency distribution of breast cancer patients with respect to disease related factors.
| Parameters | Frequency (Percent frequency) |
|---|
| Female (n) | 45 (100) |
| Age |
| <65 years | 38 (84.4) |
| ≥65 years | 7 (15.5) |
| Carcinoma based on location of the tumour |
| Medullary carcinoma | 2 (5) |
| Infiltrating ductal carcinoma | 43 (95) |
| Grade |
| Grade-1 | 8 (17.7) |
| Grade-2 | 34 (75.55) |
| Grade-3 | 3 (6.66) |
| Hormone receptor status |
| ER positive | 4(8.9) |
| PR positive | 2 (4.4) |
| ER and PR positive | 10 (22.2) |
| Human epidermal growth factor receptor 2 (Her 2-neu) positive | 6 (13.3) |
| PR and Her-2-neu positive | 1(2.2) |
| Hormonal receptor negative | 22 (48.9) |
[Table/Fig-4a] show the frequency distribution of cancer patients population with respect to their pre-diagnosed haemoglobin levels who are diagnosed and grading was done based on their surgical pathology report and AJCC guidelines (n=71). Our result clearly indicated that anaemic patients (n=49, 69%) were found to be high in comparison to frequency of non-anaemic patients is (n=22, 31%) and [Table/Fig-4b] shows the frequency distribution of cancer patients population with respect to their pre-diagnosed haemoglobin levels who are diagnosed based on different types of biomarkers. In this population, similar to the above, anaemic patients (n=19, 90.47%) were found to be high in comparison to non-anaemic patients (n=2, 9.5%).
Frequency distribution of cancer patient population (who diagnosed based on surgical pathology report, AJCC guidelines) with respect to their pre-diagnosed haemoglobin levels.
| Type of cancer (Patients diagnosed based on surgical pathology report) | (n=71) | Grade 1 | Grade 2 | Grade 3 | Grade 4 |
|---|
| Hb ≥12 | Hb <12 | Hb ≥12 | Hb <12 | Hb ≥12 | Hb <12 | Hb ≥12 | Hb <12 |
|---|
| Breast cancer | 45 | 5 | 3 | 7 | 27 | 1 | 2 | 0 | 0 |
| Gastrointestinal cancer | 14 | 1 | 1 | 3 | 5 | 1 | 2 | 0 | 1 |
| Hodgkin’s lymphoma | 5 | 0 | 1 | 0 | 1 | 1 | 0 | 0 | 2 |
| Non-Hodgkin’s lymphoma | 1 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| Urogenital cancers based on surgical pathology report | 6 | 1 | 2 | 1 | 0 | 1 | 1 | 0 | 0 |
Frequency distribution of cancer patient population with respect to their pre diagnosed haemoglobin levels.
| Types of cancers (patients diagnosed based on immunohistochemistry reports) | (n=19) | Hb ≥12 | Hb <12 |
|---|
| Urogenital cancers | 8 | 0 | 8 |
| Other advanced metastatic cancers | 9 | 2 | 7 |
| Sarcomas | 2 | 0 | 2 |
Discussion
Now-a-days, irrespective of the level of human development, cancer is an important cause of morbidity and mortality worldwide [2]. The diversity in cancers is may be due to the variations in the magnitude and profile of the disease between and within the world regions. There are 3 specific types of cancers that dominate globally: lung, female breast, colorectal cancers. These are explained as top 3 cancers in incidence and top 5 in terms of mortality [2,9]. A new cancer resolution unanimously adopted by governments at the world health assembly, noted the potential for cancer presentation in reducing the cancer burden in the future. This resolution follows WHO Global Action Plan for the Prevention and Control of non communicable diseases (NCD’s) 2013-2020 [2].
In India, the leading type of cancer(oral, pharynx, larynx, lung etc.,) is related to tobacco habits, along with prevalence of organ specific cancer such as stomach, esophagus, breast and uterine cervix [9,10]. The number of cases due to cancer were doubled in India from 1990-2016. The trends seen in sex specific and cancer type-specific incidence rate over time in India are multifactorial. The increased age-standardised death rate for cancer in males during this period suggest differences due to sex [1].
For breast cancer a substantial increase in age standardised incidence rate is consistent with changes in some risk factors over time in India such as late age at first birth, lower parity, increase in body weight, dietary changes, exogenous or endogenous changes, familial history of breast or ovarian cancer [1,9].
The interplay of the trends of the two risk factors to which the highest proportion of cancer DALY’s in India could be attributed, tobacco and alcohol, is interesting in relation to the trends of the leading cancers. The tobacco related (oral, pharynx, larynx, lung etc.,) cancers are due to smoking, pan chewing [1,9]. These cancers are decreased in India from 1990-2016 as the tobacco use in India has decreased while liver cancers are increased in this period as the alcohol consumption was increased [1].
Decrease in stomach cancer across the country might be due to diet, bile reflex, decreased smoking and the unlikely factor is the high persistence of Helicobacter pylori in Indians [1,9].
Colon and rectum was the third to fifth leading cause of cancer deaths [1]. Previous studies in India reported that incidence of colorectal cancer in younger individuals escalated in recent years [10]. Colorectal cancer may be the consequence of genetic mutation besides consumption of meat, alcohol, use of tobacco, junk foods and due to lack of exercise to the body [1,9,10].
The urogenital cancers are less due to lack of genital hygiene and practicing unsafe sex [1,11] penile cancer is common in patients with phimosis [11]. Carcinoma of ovary, uterine, cervix was late diagnosed because most of the female patients were less educated and lack of knowledge [9].
In consistent with previous findings, in our study, different type of cancers such as breast cancers, gastrointestinal tract cancers, urogenital cancers were more prevalent. Our study propose that maximum number of cancer patients in our study were diagnosed in Grade 2 due to lack of awareness, absence of screening programs, which are unanimously cost-effective and present further challenge in control program for these cancers (breast, gastrointestinal, non-hodgkins lymphoma, hodgkins lymphoma, urogenital cancers). It is believed that socioeconomic and life-style changes are responsible as rising risk factors in developing countries like India. Late childbearing, dietary changes and associated changes in menstrual patterns are responsible for rising risk factors for breast cancer and urogenital cancers in females of developed and developing countries, whereas breastfeeding and physical activity are known as protective factors [2]. Earlier reports suggest that screening by mammography can substantially reduce breast cancer mortality in the women of 50 years above [3,12]. The anaemia of chronic disease is seen in a wide variety of inflammatory states including acute systemic inflammatory response syndrome, chronic infections, inflammatory disorders, and some cancers. This iron-refractory anaemia is characterised by low serum iron (hypoferremia), reduced iron binding capacity, and subnormal transferrin saturation, while bone marrow iron is relatively preserved [13]. According to study, mediators of inflammation inhibits erythropoiesis mechanism such as interleukin-1, y-interferon and tumour necrosis factor, also plays a role in development of anemia [14]. It was clearly evident that the frequency distribution of cancer patients with Hb <12 are high in Grade 2 in our study. This could probably be explained by the supporting evidence that low haemoglobin levels are associated with the disease progression in the cancer patients. These findings were endorsed with the previous study findings that oxygen delivery to tumour depends on tissue perfusion and the oxygen carrying capacity of the blood. Decrease in oxygen carrying capacity of the blood caused by anaemia may be a major causative factor for development of tissue hypoxia. Anaemia is a major factor which induces hypoxia. The hypoxic tumours have poorer response to surgery and therapy than non-hypoxic tumours. Hypoxia promotes genomic instability which in turn increase the number of genetic variants in tumour contributed malignant phenotype and to aggressive behavior, including greater propensity for metastasis, angiogenesis and escape from apoptosis enhancing the metastatic ability of tumour cells [6,15-17].
Limitation
Since, we were dealing with all different types of cancers, we decided to conduct a study based on pathology and pre-diagnosed haemoglobin levels, we could not include the effects of pre-disposing factors such as smoking, chemical exposures and viruses in the present study. This was a very small study done in a tertiary level Hospital in Southern India over a very brief period which may not be representative of whole country though gives an evidence regarding the pattern.
Conclusion
The prevalence of breast cancer patients was high in our study population. Most of the patients diagnosed in grade II were found to have less haemoglobin levels. Our results implies that anaemia could be one of the poor prognostic factors for cancer and cancer progression probably is associated with anaemia.