Depression is a chronic relapsing disorder with recurrent episodes of disabling depressive symptomatology and is considered as one of the major public health problems in low and middle-income countries [1,2]. It is one of the most common mental disorders that affect feeling, thinking, and behaviours with the symptoms of persistent sadness, loss of interest in activities, impaired ability to carry out daily activities such as sleeping, eating as well as working for at least two weeks [3-5]. Depressive symptoms have long been used to screen for clinical depression in various populations. Depression has interaction with other chronic diseases [6]. Stress and depression were positively associated with occupation injury [7]. Depression imposes an immense social burden which leads to functional impairment, decreased quality of life, low productivity and impaired interpersonal relationship [8]. The social living and working environments or social environments encompasses a variety of concepts of potential relevance for depression, such as socio-economic status, geographical location and cultural factors that caused stressful life situation when faced with unfortunate things in life [9].
Thailand economic growth has attracted an increasing number of migrant workers from neighbouring countries [10]. Migrant workers have contributed to the economic growth of the country [11]. Migrant workers in Thailand are mostly involved in the “3Ds” jobs (Dangerous, Dirty and Degrading jobs). These 3Ds conditions push them at risk for health problems. One notable health hazard of migrant workers is the deterioration of mental health including; suicide; living in a small, different and overcrowded housing conditions; dissatisfaction of neighbours; inability to adapt in living conditions and insecurity [12-16]. Furthermore, psychosocial factors such as lacking social and emotional supports from relatives and friends and getting much involved with peers having mental health problems were identified as contributing factors of depression [15,17]. Some studies indicated that migrant workers were refused by local citizens and lack of legal migration status in migration processes. Especially, almost 40 percent of migrants experienced discrimination in their workplace related to worse self-perceived health and increased risk of mental health problems [11,18-21].
The Office of Foreign Worker Administration of Thailand reported that in September 2018, there were 2.31 million migrants residing in Thailand, and about 1.2 million were from Myanmar. About 230,000 Myanmar migrant workers were in the South region. Most of these migrants worked in the rubber plantation, fishery, construction, and manufacturing sectors. Many of them did not earn enough to be able to live in proper living conditions. In addition, almost all of them had to spend most of their earnings back to family members in Myanmar. Some might not be able to adapt to the environments and suffering physical and mental problems.
A little is known about the association between depressive symptoms and living and working environments. However, a previous study investigated an association between depression and living status in the central region of Thailand [22], where its different in economics and living condition contexts. In addition, its limitations of living and working environment factors were not covered and mentioned. The small sample size was detected to be low potential generalizability to the Myanmar migrant workers. Thus, this study focused on living and working environments among Myanmar migrant workers in the south of Thailand and there were large enough sample sizes to detect the association between living and working environments and depressive symptoms by appropriate statistical approaches. Therefore, this study aimed to determine the prevalence of depressive symptoms and the influences of living and working environment factors on the depressive symptoms among Myanmar migrant workers in the South of Thailand.
Materials and Methods
Study Population
A cross-sectional analytical study was conducted between May and July 2018. The populations of this study were Myanmar migrant workers in the South of Thailand. The inclusion criteria were a Myanmar nationality, working permit, has been working in the South for at least 3 months, aged 18 years-old or above, able to verbally communicate with researchers, and agreed to participate in the study with written informed consent. The exclusion criteria were having a critical illness. The sample size was calculated by using the formula of Hsieh FY et al., to estimate the sample size for a logistic regression analysis [23]. The estimated sample size was 1,022, of which Myanmar migrant workers were recruited from 2 provinces of the South by using multi-stage random sampling method.
Research Instruments
A structured questionnaire was developed based on the research questions and relevant literatures. The structured questionnaire consisted of 6 parts:
Part A: Demographic and socio-economic characteristics: gender, age, marital status, education, occupation, personal monthly incomes (Baht), personal monthly expenditures (Baht) and health insurance.
Part B: Living and working environments: residential area, housing, workplaces, transportation, living conditions, working conditions, peer involvement, relationship with family, co-workers, and employers.
Part C: Health behaviours: adequacy of food intake, exercise, smoking, and alcohol consumption.
Part D: Physical health status: chronic diseases, received health information, and physical check-up.
Part E: the Perceived Stress Scale (PSS) of Cohen S et al., was used to assess the stress. The scores were categorised into three groups: a) low (0-13 points); b) moderate (14-26 points); and c) high (27-40 points) [24].
Part F: Depression (CES-D): The Center for Epidemiologic Studies Depression Scale (CES-D) of Radloff LS was used to assess the depressive symptoms [25]. The scores were categorised into four groups: a) normal (0-9 points), b) mild level (10-15 points), c) moderate level (16-24 points) and d) severe level (≥25 points) [26].
The questionnaire was undergone content validation by 5 experts and was revised to improve its validity. The Cronbach’s alpha coefficient of PSS and CES-D were 0.78 and 0.70, respectively. A structured questionnaire interview was conducted to collect the data from 2 interviewers who were trained and standardised for data collection skills.
Ethical Consideration
This research proposal and tool got approval from the Khon Kaen University Ethics Committee in Human research; the approval number was HE 602370. Participants received a hard copy of the dissertation information and verbal explanation. After fully understanding, the written informed consent was requested and signed before data collection.
Statistical Analysis
Demographic and socioeconomic characteristics of the participants were described by using frequency and percentage for categorical data as well as the mean and standard deviation for continuous data. A simple logistic regression was used for bivariate analysis to identify factors associated with depressive symptoms. In the bivariate and multivariable analysis, depressive symptoms were classified into 2 groups using the standard cutoff score of ≥16 points which meant ‘had depressive symptoms’ [25]. At the cut-off ≥16, its sensitivity was 0.87 (95%CI: 0.82-0.92) with the specificity of 0.70 (95%CI: 0.65-0.75) and had diagnostic OR=16.2 (95% CI: 10.49-25.10) [27]. The independent factors that had p-value <0.25 [28] were processed into the multilevel logistic regression analysis to identify the association between living and working environments with depressive symptoms when controlling the effect of other covariates. Multilevel logistic regression was administered to control the clustering effects of the selected seven districts from two provinces [29] with the goodness of fit model based on Bayesian Information Criterion (BIC) presenting adj.OR, 95% Confidence Interval (CI) and p-value <0.05 as the magnitude of effect and statistically significant. All analyses were performed using Stata version 10.0 (StataCorp, College Station, TX).
Results
More than half of the Myanmar migrant workers were male (57.63%) with the mean age of 32.94 years-old (±9.28), 70.36% were married and 36.99% finished only primary school. Most of them were in an urban setting (83.20%), 76.42% lived with family and 48.14% lived in rental house. The highest proportion worked in manufacturing (29.84%) followed by agriculture and animal husbandry, fishery and construction. Their average personal monthly income was 9,130.14 (±2,604.73) Baht, of which 3,187.32 (±1,619.71) Baht were personal monthly expenditures. Almost all had health insurance (99.71%) [Table/Fig-1].
Demographic and socioeconomic characteristics among Myanmar migrant workers (n=1,022).
| Demographic and socioeconomic characteristics | Number | Percentage |
|---|
| Gender |
| Male | 589 | 57.63 |
| Female | 433 | 42.37 |
| Age (years) |
| <25 | 205 | 20.06 |
| 25-34 | 395 | 38.65 |
| 35-44 | 284 | 27.79 |
| ≥45 | 138 | 13.50 |
| Mean±SD | 32.94±9.28 |
| Median (Min: Max) | 32(18:71) |
| Marital status |
| Married | 719 | 70.36 |
| Single | 240 | 23.48 |
| Divorced/Widowed/Separated | 63 | 6.16 |
| Education |
| No formal education | 56 | 5.48 |
| Primary school | 378 | 36.99 |
| Secondary school | 377 | 36.89 |
| High school/equivalence or higher | 211 | 20.64 |
| Occupation |
| Manufacturing | 305 | 29.84 |
| Agriculture and animal husbandry | 180 | 17.61 |
| Fishery | 172 | 16.83 |
| Construction | 164 | 16.04 |
| Service | 71 | 6.95 |
| Housework | 58 | 5.68 |
| Other | 72 | 7.04 |
| Personal monthly incomes (Baht) |
| <7,500 | 224 | 21.92 |
| 7,500-9,999 | 433 | 42.37 |
| 10,000-12,499 | 288 | 28.18 |
| ≥12,500 | 83 | 7.53 |
| Mean±SD | 9,130.14±2,604.73 |
| Median (Min: Max) | 9,000 (3,000:22,000) |
| Personal monthly expenditures (Baht) |
| <2,500 | 363 | 35.52 |
| 2,500-4,999 | 468 | 45.79 |
| 5,000-7,499 | 169 | 16.54 |
| ≥7,500 | 22 | 2.15 |
| Mean ±SD | 3,187.32±1,619.71 |
| Median (Min: Max) | 3,000 (600:15,000) |
| Health insurance |
| No | 3 | 0.29 |
| Yes | 1,019 | 99.71 |
Most of the workers worked both indoor and outdoor (64.19%) and the rest (35.81%) worked only indoor. Most of them were satisfied with their living and working conditions as well as the relationship with others, except that 61.45% had a limitation on traveling [Table/Fig-2].
Living and working environments among Myanmar migrant workers (n=1,022).
| Living and working environments | Number | Percentage |
|---|
| Residential area |
| Rural | 182 | 17.80 |
| Urban | 840 | 83.20 |
| Housing |
| Labor camp | 484 | 47.36 |
| Rental house | 492 | 48.14 |
| Apartment | 31 | 3.03 |
| Workplaces |
| Indoor and outdoor | 656 | 64.19 |
| Indoor | 366 | 35.81 |
| Lived with |
| Family | 781 | 76.42 |
| friends | 100 | 9.78 |
| Alone | 72 | 7.05 |
| Relatives | 43 | 4.21 |
| Parents | 26 | 2.54 |
| Problem on living conditions |
| Low | 899 | 87.96 |
| Moderate | 112 | 10.96 |
| Severe | 11 | 1.08 |
| Problem on working conditions |
| Low | 736 | 72.02 |
| Moderate | 255 | 24.95 |
| Severe | 31 | 3.03 |
| Involvement with peers |
| Low | 27 | 2.64 |
| Moderate | 564 | 55.19 |
| High | 431 | 42.17 |
| Relationship with co-workers |
| Low | 7 | 0.68 |
| Moderate | 556 | 54.41 |
| High | 459 | 44.91 |
| Relationship with family |
| Low | 10 | 0.98 |
| Moderate | 277 | 27.10 |
| High | 735 | 71.92 |
| Relationship with employers |
| Low | 50 | 4.89 |
| Moderate | 554 | 54.21 |
| High | 418 | 40.90 |
| Limitation in traveling |
| No | 394 | 38.55 |
| Yes | 628 | 61.45 |
About one-third were smokers (35.13%), 14.87% were drinkers. More than half of the migrant workers (55.28%) had a physical check-up and 11.35% had chronic diseases. Most of them had a moderate level of stress (89.43%) [Table/Fig-3].
Health behaviours and physical health status among Myanmar migrant workers (n=1,022).
| Health behaviours and physical health status | Number | Percentage |
|---|
| Food intake |
| Adequate | 986 | 96.48 |
| Inadequate | 36 | 3.52 |
| Exercise during the past one month |
| No | 302 | 29.55 |
| Yes | 720 | 70.45 |
| Smoking |
| Nonsmoker | 639 | 62.52 |
| Former smoker | 24 | 2.35 |
| Smoker | 359 | 35.13 |
| Alcohol consumption |
| Nondrinker | 840 | 82.19 |
| Former drinker | 30 | 2.94 |
| Drinker | 152 | 14.87 |
| Chronic diseases |
| No | 906 | 88.65 |
| Yes | 116 | 11.35 |
| Received health information |
| No | 555 | 54.31 |
| Yes | 467 | 45.69 |
| Physical check-up |
| No | 457 | 44.72 |
| Yes | 565 | 55.28 |
| Stress |
| Low | 83 | 8.12 |
| Moderate | 914 | 89.43 |
| High | 25 | 2.45 |
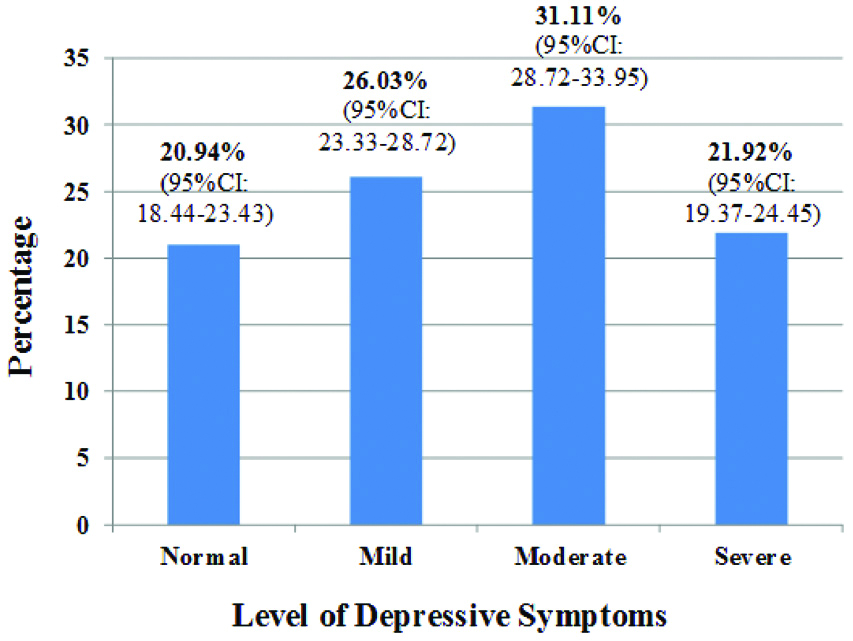
Concerning depressive symptoms, 21.92% of the migrant workers suffering severe depressive symptoms, 31.11% had moderate depressive symptoms and 26.03% had mild depressive symptoms [Table/Fig-4].
Bar chart of the prevalence of depressive symptoms among Myanmar migrant workers (n=1,022).
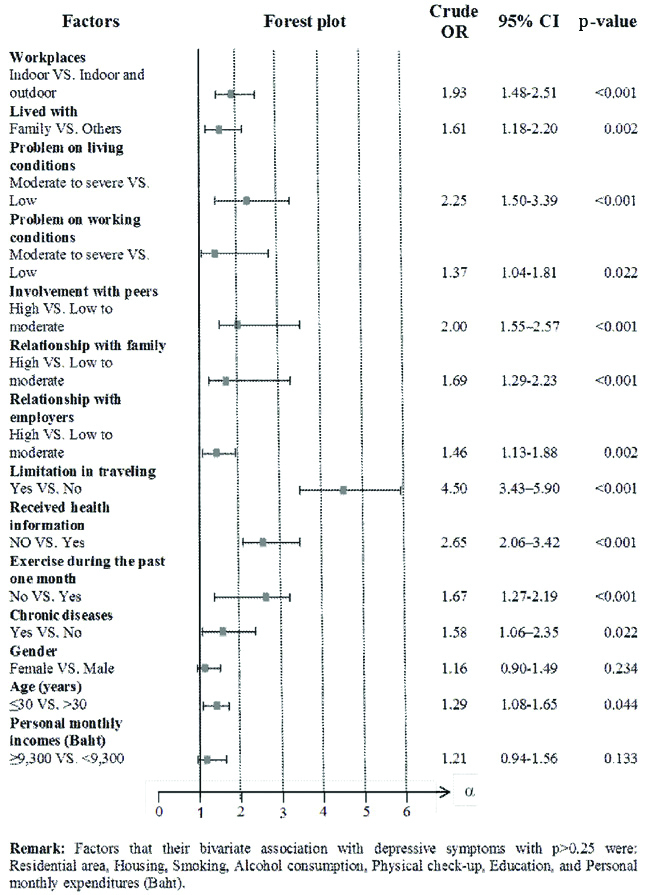
The bivariate analysis results indicated that the independent variables that were associated with depressive symptoms were; workplaces, working condition problems, peer involvement, relationship with employers, lived with a family, relationship with family, living condition problems, social support on health information and limitation in traveling, exercise, had chronic diseases and age [Table/Fig-5].
Forest plot of bivariate analyses for factors associated with depressive symptoms among Myanmar migrant workers by using simple logistic regression (n=1,022).
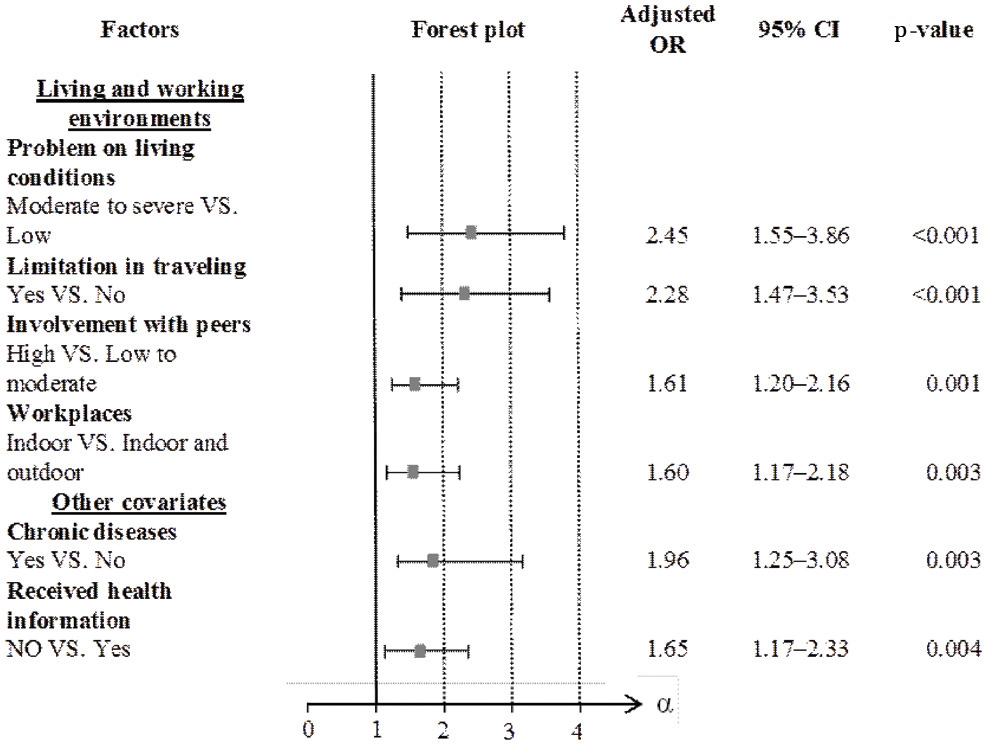
Multilevel logistic regression results indicated that some living and working environments were associated with depressive symptoms [Table/Fig-6].
Forest plot of multilevel logistic regression analysis on the influence of living and working environments on depressive symptoms when controlling covariates among Myanmar migrant workers (n=1,022).
Discussion
The findings indicated that majority of the Myanmar migrant workers were suffering from moderate (31.11%) to severe depressive symptoms (21.92%) or overall depressive symptoms prevalence of 53.03% and some living and working environments, health problems and health information were associated with depressive symptoms. This finding was consistent with a previous study among Myanmar migrant workers in Thailand found that the prevalence of the depressive symptoms was 52.40% [22]. The findings might have shared similar socio-economic factors since they were Myanmar migrant workers in Thailand. However, this study shows that the prevalence of depressive symptoms was higher compared to other studies in migrants of Peru and China [30,31].
This study indicated that those who had moderate to severe levels of living condition problems had significantly more severe depressive symptoms in comparison with those who had a low level of living condition problems, of which similar with other studies conducted in the US [15,16]. The rationales might be that most of the Myanmar migrants in our study lived in the overcrowded shelter since 47.36% of them lived in labor camps and another (48.14%) were in rental houses. In addition, their shelters might be situated in a polluted area that caused poor living condition since more than half of them worked in construction, fishery, and agricultural and animal husbandry sectors. These unpleasant conditions could have influenced their mood disorders.
This study also illustrated that those who have limitation in traveling had significantly higher severe depressive symptoms. Limitation of traveling may lead to lack of relaxation and the previous study stated similar condition that adopting a healthy lifestyle such as leisure activities and exercises can reduce the risk of depression [32,33].
This study indicated that those who worked only indoor had significantly higher severe depressive symptoms, which was similar to the finding explaining that the contact with outdoor natural environments can facilitate stress reduction [34].
However, the current study observed that those who had a high level of peer involvement had significantly more severe depressive symptoms than those with low to moderate levels of peer involvement, similar with a study in the US explaining that close relationship or stronger association with a neighbour with the same ethnic was related to poor mental health [15].
Concerning physical health status, this study indicated that those who suffered from chronic diseases were most likely to have severe depressive symptoms. A study conducted in Jordan had also observed a similar finding [35]. This is a very logical consequence that chronic diseases could have an impact on their ability to work, comfort and economic burden that could reduce their well-being.
Finally, migrant workers who never received health information were more likely to have more severe depressive symptoms. Migrants were usually accessed with health information through social networks more than formal health service providers due to language and access barriers [36].
Health information could help to reduce suffering from both physical and mental problems. Lack of or limited access to health information could worsen their conditions. These results could help Myanmar migrant communities, employers, health sectors and local administrations to increase their understanding of depressive symptoms and to develop effective interventions for prevention and managing the depressive symptoms.
Limitation
CES-D was designed to assess for depressive symptoms in the general population and has been used to identify a person as having depressive symptoms and not depression which needs a clinical diagnosis. This cross-sectional study was conducted among Myanmar migrant workers in the South of Thailand; therefore, it might not represent other locations or other migrants in Thailand. The exposure and outcome are simultaneously assessed; no causal relationship can be identified.
Future Recommendations
It is an important suggestion for a further study which could identify the causal relationship by using other study designs such as a cohort study.
Conclusion
This present study observed that more than half of Myanmar migrant workers in the South of Thailand had depressive symptoms. After adjusting for other covariates which had chronic diseases and access to health information, the living and working environments, had moderate to severe levels of living condition problems, limitation in traveling, and high level of peer involvement and worked indoor was found significantly associated with depressive symptoms.