Obesity is a chronic disease that ruins one’s physical and mental health including the risk factors to acquire other diseases [1] such as hypertension, high cholesterol including the risk for ischemic stroke [2]. Obesity is associated with a higher risk of type 2 diabetes [3], respiratory problem during state of sleep apnea and asthma, joint injury and painful muscles and bones, fatty liver diseases, gallstones and gastro-esophageal reflux diseases [4], mental stress like major depression disorder, personal behaviour problem and low health-related quality of life [5,6]. Obesity has an important impact to reduce quality of life [7], low self-esteem and low quality of life [8,9].
The estimation for the global prevalence of overweight and obesity in 2016 over was 340 million children and adolescents aged between 5 to 19 years were overweight. This prevalence has risen dramatically from 4% in 1975 to over 18% in 2016 in both boys (19%) and girls (18%) [10]. Around 80% of obese adolescents become obese during adulthood, and around 70% becomes obese during the age of 30 years [11]. According to the Data Center Bureau of Policy and Strategy, and Ministry of Public Health Thailand in 2017 survey, children nutritional condition at aged 6-14 years-old showed that children seem to gain weight and overweight at 10.61% in 2014, 11.73% in 2015, 12.89% in 2016 and 12.77% in 2017 [12]. With all information gathered, the rate of obesity in children and adolescents has increased which indicated that an urgent administration to correct this action would be essentially needed by using the PRECEDE-PROCEED Model and health literacy as the key determinant for weight evaluation. This study used the PRECEDE framework model in educational research and health literacy.
PRECEDE-PROCEED Model is one of the successful models to do any planning designing, implementing and evaluating which helps us to be more knowledgeable and better [13].
The PRECEDE-PROCEED model is a cost-benefit evaluation framework proposed in 1974 by Green L that can aid health program planners, policy makers and other evaluators scrutinise situations and propose health programs competently [14,15]. The PRECEDE acronym stands for Predisposing, Reinforcing, Enabling Constructs in Educational/Environmental Diagnosis and Evaluation [16]. Predisposing factors include knowledge, attitude, beliefs, values and perceptions. Enabling factors include availability and accessibility to services and skills in achieving the behaviour. Reinforcing factors include incentives and ways to maintain the behavioural change. These could include both positive and negative reinforces [17]. There are many studies that support the PRECEDE-PROCEED model in a positive way. The model is quite efficient in promoting health. It also motivates people to work out increasingly [18]. Health literacy represents a specific set of cognitive and social skills related to health decision-making whether this is making best use of health services, adopting healthy lifestyles, or taking an active role in addressing the social determinants of health [19]. The relationship between poor literacy skills and health status is now well recognised and better understood. The studies using Health literacy six skills include cognitive, access, communication, self-management, media literacy and decision skills [20]. In Thailand, health literacy has been promoted as a mechanism for the national development which responds to the 20-year National Strategic Framework and the 12th National Economic and Social Development Plan B.E. 2560-2564 (2017-2021) under the new the Constitution of the Kingdom of Thailand B.E. 2560-2579 (2017-2036), thus leading the country to greater wealth, prosperity, and sustainability over the next 20 years [21]. It shows that the populations still don’t have much understanding of health literacy to prevent any health risk factors [22]. The research found that the obesity in adolescents was strongly associated with health literacy of the adolescents [23]. The health literacy is one factor to promote and maintain health.
The researcher realises the importance of the obesity problems in adolescents, so the ways to solve this problem is to analyse the factors that cause obesity, focusing on their health literacy so that they can control their weight loss in the correct ways. But the study about obesity in adolescence and prevalence of obesity in the Northeast of Thailand has not been conducted yet. Therefore, this study was aimed to investigate the prevalence and determinants of PRECEDE Framework Model, health literacy and other covariates of overweight and obesity among adolescents in the Northeast of Thailand.
Materials and Methods
A cross-sectional study was conducted from September 2017 to March 2018 among adolescent students at the secondary schools in the Northeast of Thailand. Ethical approval for this study was obtained from Khon Kaen University considerations Ethic Committee for Human Research (reference no. HE602200). The inclusion criteria were the students who studied at Mattayom 1 to Mattayom 6 of both gender aged 12-19 years old, were included in this study; students who had permission from their parents and voluntarily participate in the study were also included. The sample size was calculated by using multiple logistic regression formula of Hsieh [24].
The sample size of 234 was initially calculated and was further adjusted for over-fitting control, using rho (ρ) of 0.80 and Variance Inflation Factor (VIF) sample size of 903 finally preventing missing data or loss of 20% sample size was adjusted by using formula of Lachin J, the total sample was 1,129 [25]. They were selected using multi-stage random sampling. First, 4 out of 20 provinces in the Northeast of Thailand were randomly selected. (Ubon Ratchathani, UdonThani, Kalasin and Nakhon Ratchasima) Next, simple random sampling was used to select randomly 12 out of 227 secondary schools in these 4 provinces and were classified into extra-large, large, middle and small schools. Then using stratified random sampling students were then divided according to their educational level from Secondary School, Mattayom 1 to Mattayom 6. Finally, simple random sampling was applied to select the sample proportion number of all students to the size of the samples added to the total of 1,129 samples.
Bivariate data analysis and multivariable data analysis in the study were 1,026 samples. The researchers wanted to conduct a study to identify the risk factors for overweight and obesity with normal weight. Therefore, excluding underweight of 103 samples. The questionnaire was modified from the PRECEDE framework model [15] and was modified from the health literacy six skills include cognitive, access, communication, self-management, media literacy and decision skills set by the Health Education Division, Department of Health Service Support, Ministry of Public Health [19]. The questionnaire’s content validity was confirmed by five experts and pre-tested for clarity, timing, and validity with a similar group of the same age range and education level and the tool had high level of reliability with Cronbach’s alpha of 0.90.
Instrument
The questionnaire consisted of: 1) Demographic Characteristics consisted of gender, age, current education, highest education of parents, monthly income, time to watch TV, surfing the internet and sleeping time; 2) Evaluation of overweight and obesity consisted of BMI for age. The outcome of overweight and obesity rating using BMI for age (CDC, 2000) calculated by gender, age, weight, and height. (Less than the 5th percentile is Underweight, 5th percentile to less than the 85th percentile is Normal or Healthy Weight, 85th to less than the 95th percentile is overweight and equal to or greater than the 95th percentile is obesity) [26]; 3) Three factors; Predisposing factors consisted of knowledge and attitude of obesity, enabling factors consisted of supermarkets, other food stores and received public health services and reinforcing factors consisted of incentives, either tangible or in the form of social support [27]. Evaluation of knowledge calculated and analysed [27] had 10 questions with a correct answer=1 and an incorrect answer=0, and they were interpreted to a high level, 80% (≥8 points), a moderate level, 60%-79% (6-7 points) and a low level, 0-59% (<6 points). Predisposing factors of attitude has 5 rating scales that is 5=Strongly Agree, 4=Agree, 3=Neutral, 2=Disagree, 1=Strongly Disagree. The attitude level had 10 questions and was interpreted as high level, X̄+SD (42-50 points); moderate level, X̄±SD (30-41 points) and low level, X̄-SD (5-29 points). The enabling factors and reinforcing factors had 5 rating scales that is 5=Most, 4=Much, 3=Moderate, 2=Little, 1=Least. The enabling level had 10 questions and was interpreted as high level, X̄+SD (35-50 points); moderate level, X̄±SD (27-34 points) and low level, X̄-SD (5-26 points). The reinforcing level had 10 questions and was interpreted as high level, X̄+SD (35-50 points); moderate level, X̄±SD (27-34 points) and low level, ̄-SD (5-26 points) [28]; 4) Health Literacy to prevent obesity disease. Evaluation of health literacy skills for the cognitive were calculated and analysed [27] had 10 questions and they were interpreted to a high level, 80% (≥8 points), a moderate level, 60%-79% (6-7 points) and a low level, 0-59% (<6 points). Health literacy skills for access, communication, self-management, media literacy, decision were calculated and analysed [27].
Statistical Analysis
Stata version 10.0 (StataCorp, College Station, TX) was used for data analyses. Descriptive statistical analysis was presented in numbers and percentages for categorical variables and mean standard deviations, and min-max for continuous variables. Inferential statistics, simple logistic regression, was used for bivariate analysis to identify factors associated with overweight and obese teenagers. The factors that had p-value <0.25 were processed into the multivariable analysis using multiple logistic regression and reported a 95% confidence interval (95% CI) and considered significant at p<0.05.
Results
A total of 1,129 adolescents took part, the majority of whom were females accounting for 63.86% and 36.14% were males, average monthly income, spending time watching TV, spending time to surf the internet and sleeping duration [Table/Fig-1].
Demographic characteristics of adolescents.
| Characteristics | Number | Percent |
|---|
| 1. Gender | | |
| Male | 408 | 36.14 |
| Female | 721 | 63.86 |
| 2. Age (years) | | |
| 12-15 | 601 | 53.23 |
| 16-19 | 528 | 46.77 |
| 3. Current education | | |
| Grade 1-3 | 556 | 49.24 |
| Grade 4-6 | 573 | 50.76 |
| 4. Highest education of parents | | |
| Greater than or equal high school | 538 | 47.66 |
| Less than high school | 591 | 52.34 |
| 5. Monthly income (Bath/Month) | | |
| Mean (SD) | 2,150 (1396.57) | |
| Median (Min: Max) | 2,000 (300:35,000) | |
| 6. Time to watch TV (Hr./Day) | | |
| Mean (SD) | 2.57 (1.81) | |
| Median (Min: Max) | 2 (0:15) | |
| 7. Surfing the internet (Hr./Day) | | |
| Mean (SD) | 4.97 (3.24) | |
| Median (Min: Max) | 4 (0:16) | |
| 8. Sleeping time (Hr./Day) | | |
| Mean (SD) | 7.52 (1.18) | |
| Median (Min: Max) | 2 (8:12) | |
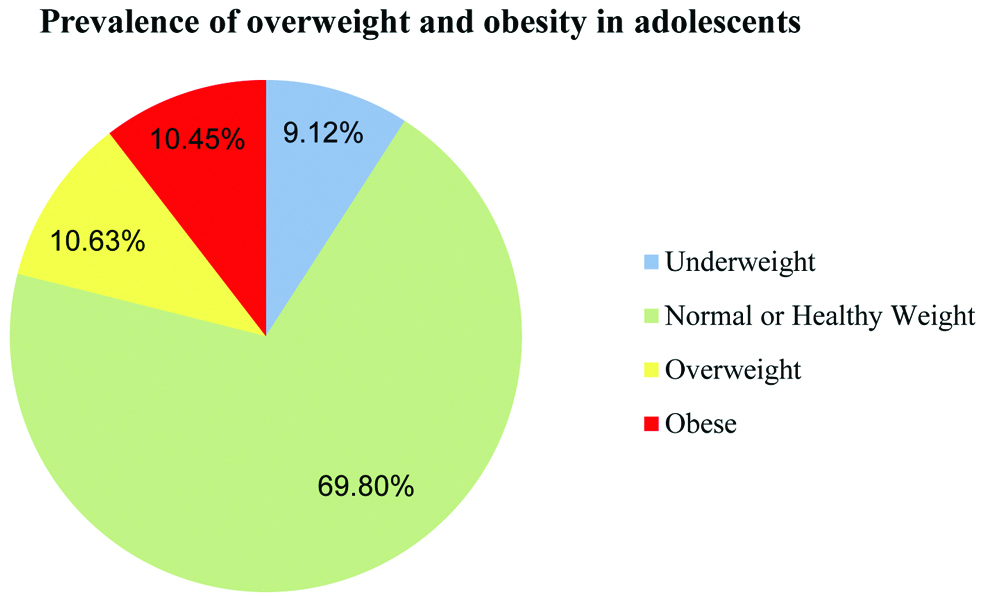
The prevalence of underweight was 9.12%, overweight was 10.63, obesity was 10.45 and normal or healthy weight was 69.80 [Table/Fig-2].
Prevalence of overweight and obesity in adolescents: a population-based survey of 12-19 years old of both sexes in the Northeast of Thailand.
Out of all the adolescents in this study, 70.27% had high level of knowledge, 66.57% had moderate level of attitude, 74.46% had moderate level of enabling factors, 67.84% had moderate level of reinforcing factors, 40.16% had moderately correct cognitive skills, 59.84% had moderate level of access skills, 46.78% had moderate level of communication skills, 56.14% had moderate level of self-management skills, 47.66% had moderate level of media literacy skills, and 45.71% had moderate level of decision skills [Table/Fig-3].
Levels of each factor of PRECEDE Framework and Health Literacy.
| Level of factor | Number | Percent % | (95%CI) |
|---|
| PRECEDE framework | | | |
| 1. Predisposing factors | | | |
| 1.1 Knowledge of obesity | | | |
| High | 721 | 70.27 | 67.37-73.05 |
| Moderate | 239 | 23.29 | 20.73-26.00 |
| Low | 66 | 6.43 | 5.00-8.11 |
| Mean±SD: 8.38±1.49, Median (Min: Max): 8 (2:10) |
| 1.2 Attitude of obesity | | | |
| High | 199 | 19.40 | 17.01-21.95 |
| Moderate | 683 | 66.57 | 63.58-69.45 |
| Low | 144 | 14.04 | 11.96-16.31 |
| Mean±SD: 36.46 (6.23), Median (Min: Max): 37 (17:50) |
| 2. Enabling factors | | | |
| High | 146 | 14.23 | 12.14-16.51 |
| Moderate | 764 | 74.46 | 71.67-77.10 |
| Low | 116 | 11.31 | 9.43-13.40 |
| Mean±SD: 30.76 (3.72), Median (Min: Max): 31 (18:44) |
| 3. Reinforcing factors | | | |
| High | 192 | 18.71 | 16.37-21.23 |
| Moderate | 696 | 67.84 | 64.88-70.68 |
| Low | 138 | 13.45 | 11.42-15.69 |
| Mean±SD: 30.92±4.23, Median (Min: Max): 31 (16:46) |
| Health literacy | | | |
| 1. Cognitive skills | | | |
| High | 317 | 30.90 | 28.07-33.82 |
| Moderate | 412 | 40.16 | 37.13-43.22 |
| Low | 297 | 28.95 | 26.18-31.82 |
| Mean±SD: 6.45±1.90, Median (Min: Max): 7 (1:10) |
| 2. Access skills | | | |
| High | 90 | 8.77 | 7.11-10.67 |
| Moderate | 614 | 59.84 | 56.77-62.86 |
| Low | 322 | 31.38 | 28.55-34.32 |
| Mean±SD: 15.67±2.76, Median (Min: Max): 15 (7:25) |
| 3. Communication skills | | | |
| High | 83 | 8.09 | 6.49-9.92 |
| Moderate | 480 | 46.78 | 43.69-49.89 |
| Low | 463 | 45.13 | 42.05-48.23 |
| Mean±SD: 18.05±3.45, Median (Min: Max): 18 (9:29) |
| 4. Self-management skills | | | |
| High | 200 | 19.49 | 17.11-22.05 |
| Moderate | 576 | 56.14 | 53.04-59.20 |
| Low | 250 | 24.37 | 21.76-27.11 |
| Mean±SD: 16.46±3.58, Median (Min: Max): 16 (5:25) |
| 5. Media literacy skills | | | |
| High | 228 | 22.22 | 19.71-24.89 |
| Moderate | 489 | 47.66 | 44.56-50.76 |
| Low | 309 | 30.12 | 27.32-33.02 |
| Mean±SD: 16.23±3.80, Median (Min: Max): 16 (5:25) |
| 6. Decision skills | | | |
| High | 305 | 29.73 | 26.94-32.62 |
| Moderate | 469 | 45.71 | 42.63-48.81 |
| Low | 252 | 24.56 | 21.95-27.31 |
| Mean±SD: 11.17±2.50, Median (Min: Max): 11 (4:16) |
In the bivariate analysis using simple logistic regression, the individual factors that were statistically significant with overweight and obesity were: had age, Surfing the internet >5 Hr/Day and Sleeping time <8 Hr/Day [Table/Fig-4]. The PRECEDE Framework model and health literacy factors at the low level of each skill were significantly associated with overweight and obesity among adolescents in the Northeast of Thailand were: attitude, reinforcing factors, cognitive skills, access skills, communication skills, self-management skills, media literacy skills and decision skills [Table/Fig-5].
Factors associated with overweight and obesity among adolescents a bivariate analysis.
| Factors | Number | % Obesity | Crude OR | (95% CI) | p-value |
|---|
| 1. Age (years) | | | | | 0.003 |
| 12-15 | 559 | 26.83 | 1 | | |
| 16-19 | 467 | 18.84 | 0.63 | 0.46-0.85 | |
| 2. Gender | | | | | 0.201 |
| Male | 361 | 25.48 | 1 | | |
| Female | 665 | 21.95 | 0.82 | 0.60-1.10 | |
| 3. Highest education of parents | | | | | 0.420 |
| Greater than or equal high school | 493 | 22.11 | 1 | | |
| Less than high school | 533 | 24.20 | 1.12 | 0.84-1.51 | |
| 4. Monthly income (Bath/Month) | | | | | 0.564 |
| ≤2000 | 652 | 23.77 | 1 | | |
| >2000 | 374 | 22.19 | 0.91 | 0.67-1.23 | |
| 5. Time to watch TV (Hr./Day) | | | | | <0.001 |
| <3 | 570 | 17.89 | 1 | | |
| ≥3 | 456 | 29.82 | 1.95 | 1.45-2.61 | |
| 6. Surfing the internet (Hr./Day) | | | | | 0.010 |
| 0-2 | 248 | 18.55 | 1 | | |
| 3-5 | 451 | 21.73 | 1.21 | 0.82-1.80 | |
| >5 | 327 | 28.75 | 1.77 | 1.18-2.64 | |
| 7. Sleeping time (Hr./Day) | | | | | 0.043 |
| 8 | 472 | 20.55 | 1 | | |
| <8 | 428 | 27.10 | 1.43 | 1.05-1.95 | |
| >8 | 126 | 19.84 | 0.95 | 0.58-1.56 | |
Factors associated with overweight and obesity among adolescents a bivariate analysis.
| Factors | Number | % Obesity | Crude OR | (95% CI) | p-value |
|---|
| PRECEDE framework | | | | | |
| 1. Predisposing factors | | | | | |
| 1.1 Knowledge of obesity | | | | | 0.475 |
| High | 561 | 22.19 | 1 | | |
| Moderate | 179 | 25.10 | 1.75 | 0.83-1.65 | |
| Low | 48 | 27.27 | 1.31 | 0.74-2.32 | |
| 1.2 Attitude of obesity | | | | | <0.001 |
| High | 168 | 15.58 | 1 | | |
| Moderate | 524 | 23.28 | 1.64 | 1.07-2.50 | |
| Low | 96 | 33.33 | 2.70 | 1.64-4.54 | |
| 2. Enabling factors | | | | | 0.089 |
| High | 114 | 21.92 | 1 | | |
| Moderate | 584 | 23.56 | 1.09 | 0.71-1.68 | |
| Low | 90 | 22.41 | 1.02 | 0.57-1.85 | |
| 3. Reinforcing factors | | | | | 0.005 |
| High | 147 | 23.44 | 1 | | |
| Moderate | 550 | 20.98 | 0.86 | 0.59-1.26 | |
| Low | 91 | 34.06 | 1.68 | 1.03-2.74 | |
| Health literacy | | | | | |
| 1. Cognitive skills | | | | | <0.001 |
| High | 262 | 17.35 | 1 | | |
| Moderate | 320 | 22.33 | 1.36 | 0.94-1.98 | |
| Low | 206 | 30.64 | 2.10 | 1.43-3.08 | |
| 2. Access skills | | | | | 0.072 |
| High | 75 | 16.67 | 1 | | |
| Moderate | 478 | 22.15 | 1.42 | 0.79-2.55 | |
| Low | 235 | 27.02 | 1.85 | 1.00 to 3.39 | |
| 3. Communication skills | | | | | 0.001 |
| High | 70 | 15.66 | 1 | | |
| Moderate | 386 | 19.58 | 1.31 | 0.69-2.47 | |
| Low | 332 | 28.29 | 2.12 | 1.13-3.97 | |
| 4. Self-management skills | | | | | 0.009 |
| High | 163 | 18.50 | 1 | | |
| Moderate | 450 | 21.88 | 1.23 | 0.82-1.85 | |
| Low | 175 | 30.00 | 1.88 | 1.20-2.95 | |
| 5. Media literacy skills | | | | | <0.001 |
| High | 200 | 12.88 | 1 | | |
| Moderate | 384 | 21.47 | 1.95 | 1.24-3.06 | |
| Low | 204 | 33.98 | 3.67 | 2.32-5.82 | |
| 6. Decision skills | | | | | <0.001 |
| High | 226 | 12.79 | 1 | | |
| Moderate | 374 | 20.26 | 1.73 | 1.15-2.59 | |
| Low | 148 | 41.27 | 4.79 | 3.15-7.28 | |
The data for association between all potential factors using multiple logistic regressions are shown in [Table/Fig-6]. The researcher found that the duration of watching TV ≥3 Hr/Day has a risk to be obese 1.94 times of the ones who watch TV <3 Hr/Day, surfing internet >5 Hr/Day they has a risk to be obese 1.82 times of the ones who spent time lesser than 0-2 Hr/Day, low level of attitude to obesity is risky 2.61 times of the persons who had a higher level of attitude to obesity, the reinforcing factors, the one who was in low level is riskier 1.79 times, low level of media literacy skills would have chance to be obese 3.64 times, low level of decision skills has more chance to be obese 5.12 times.
Factors associated with overweight and obesity among adolescents: a multivariable analysis.
| Factors | Number | % of Obesity | Crude OR | Adjusted OR | 95% CI | p-value |
|---|
| 1. Time to watch TV (Hr./Day) | <0.001 |
| <3 | 570 | 17.89 | 1 | 1 | | |
| ≥3 | 456 | 28.82 | 1.95 | 1.94 | 1.39-2.64 | |
| 2. Surfing the internet (Hr./Day) | 0.007 |
| 0-2 | 248 | 18.55 | 1 | 1 | | |
| 3-5 | 451 | 21.73 | 1.21 | 1.32 | 0.86-2.02 | |
| >5 | 327 | 28.75 | 1.77 | 1.82 | 1.17-2.81 | |
| 3. Predisposing factors | |
| 3.1 Attitude of obesity | 0.001 |
| High | 168 | 15.58 | 1 | 1 | | |
| Moderate | 524 | 23.28 | 1.64 | 1.44 | 0.91-2.27 | |
| Low | 96 | 33.33 | 2.70 | 2.61 | 1.49-4.57 | |
| 4. Reinforcing factors | 0.030 |
| High | 147 | 23.44 | 1 | 1 | | |
| Moderate | 550 | 20.98 | 0.86 | 0.83 | 0.55-1.26 | |
| Low | 91 | 34.06 | 1.68 | 1.79 | 1.05-3.06 | |
| 5. Media literacy skills | <0.001 |
| High | 200 | 12.88 | 1 | 1 | | |
| Moderate | 384 | 21.47 | 1.95 | 1.79 | 1.11-2.87 | |
| Low | 204 | 33.98 | 3.67 | 3.64 | 2.23-5.93 | |
| 6. Decision skills | <0.001 |
| High | 226 | 12.79 | 1 | 1 | | |
| Moderate | 374 | 20.26 | 1.73 | 1.74 | 1.13-2.66 | |
| Low | 148 | 41.27 | 4.79 | 5.12 | 3.28-8.00 | |
Discussion
Obesity is a serious chronic disease which affects one’s physical and mental health, it increases the risk for other diseases. The prevalence of overweight and obesity worldwide is high and tend to be on increase [10]. Therefore, it is needed to change the health behaviour. This study investigated the prevalence and determinants of PRECEDE Framework and health literacy associated with overweight and obesity among adolescents.
The study shows that the sampling group aged 10-19 years, the prevalence of overweight is 10.63% and obesity is 10.45%. This result is consistent with the study of Mazidi M et al., who studied the prevalence of overweight and obesity of the adolescent in Asia by systematic review and Meta analysis by base on CDC standard; they found out that the prevalence of obesity is 8.9%, the prevalence of overweight is 14.6% [28]. The results from this study show that the provenance of both issues is the main problem to the adolescent, should be solved immediately.
Multivariable analysis showed factors associated with the obesity in the adolescent after control other covariate factors, it was found that the adolescents spent more time watching TV over or equal 3 hours per day, their surfing internet over than 5 hours per day that is consistent with the study of Tomar S et al., which showed that teenagers’ behaviour such as surfing the internet video game playing time over 5 hours per day and watching TV while eating, these behaviour are relevant factors for overweight and obesity [29]. Therefore, teenagers should not spend time watching TV and surfing the internet over 2 hours per day.
Factor of PRECEDE Framework model which includes predisposing factors that are attitude and reinforcement associated with obesity were at low level. This result is consistent with the study of Sai Mueang S, which showed that awareness about the health beliefs and behaviour were associated with obesity (p=0.026) and social support also were correlated with obesity (p<0.001) during the 1-3 year period of study. These were statistically significant at 0.05 level [30]. Social support is also related to obesity’s behaviour condition that is similar to the study of Walker N, her study data stated that the best factors predicting healthy meal and physical activities of the adolescent are an attitude [31]. Both their studies showed that theories of behavioural sciences are one of the factor which can be considered to support the population’s health behaviour, therefore if the adolescent gets the good health to have a better attitude and reinforcing factors to the obesity, it influences to reduce obesity.
In addition, findings showed that a low level of media literacy and low level of decision skills associated with overweight and obesity. This result is consistent with the findings of Tipwong A and Numpoon J [32]. The results show health literacy regarding the decision skills had a positive relationship with their consumption behaviour at the significant level of 0.05. In addition, self-management skills and media literacy skills had a positive relationship with their exercise behaviour at the significant level of 0.01 and 0.05 respectively [32].
However, if a healthy useful alternative determination is adopted and review it reasonably before actual practice, it gives good direction to the health that conforms to the study of Chari R et al., [23]. The results showed that health literacy is associated with obesity in teenagers. This effects on strategies of prevention and remedial treatment to the obesity disease [23], thus, they should focus on their health literacy as a main point so that the motivation to adjust their behaviour in the better ways can be done and they will become more confident to practice it, like changing their lifestyle and their state of living in order to be healthier by their own-selves by using the six skills which reflect their characteristics and their behaviour. The association of occurrence of obesity to the adolescent according to the statistical significance. The results from this study suggest adolescents who still lack attitude, reinforcing factors and health literacy, especially relating to media literacy skills and decision skills which lead them to incorrect practices.
Limitation
Limitations of the study include the cross-sectional study design, thus, causal relationships cannot be concluded. There are nevertheless some limitations the database does not include information on the prevalence of overweight or obesity amongst parents may be associated with result. Conversely, this study is based on a large sample size and used standardised methods for all its measures. It is suggested that further studies should apply a prospective cohort or experimental study for a causal relationship.
Conclusion
From the results of this study, the factors associated with overweight and obesity include spending time on the TV, surfing the internet, the PRECEDE Framework Model including: low levels of attitude and low levels of reinforcing factors. Also, low levels of literacy health literacy which tends to increase the risk factors to the obesity in the adolescents in North Eastern of Thailand, especially, the low levels of media literacy skills and the low levels of decision skills. Therefore, the PRECEDE Framework Model and health literacy may be a desirable strategy for informing and Behavioural Modification for Weight Control among Overweight and Obesity. There is an urgent need for a comprehensive integrated intervention program to ameliorate the problem of obesity of Adolescents in the Northeast of Thailand.