Globus pharyngeus is a condition known to man since the time of Hippocrates. The term globus hystericus was first given by Purcell in the 18th century [1]. Later on, in the year 1968, Malcolmson suggested a change in the term to globus pharyngeus as it was not always seen in hysterical patients [2].
Globus pharyngeus is a chronic painless condition in which patient complains of constant feeling of lump in the throat or foreign body sensation in the throat [3]. The word globus comes from a Latin word meaning ‘Ball’ [4]. It is a fairly common condition reported by patients consulting Ear, Nose and Throat (ENT) clinics seen in around 4% of new cases. It is reported by about 46% of healthy individuals [5,6]. The incidence of the disease has been found to be similar in men and women [7]. The most common complaint with which the patient visits an ENT clinic is feeling of lump in the throat, foreign body sensation in the throat, sticking sensation in the throat or throat pain. The aetiopathogenesis of this condition is still not known for certain but it appears to be multifactorial. Some of the factors considered to cause symptoms of globus pharyngeus are gastroesophageal reflux disease, abnormal upper oesophageal sphincter function, oesophageal motor disorders, inflammatory causes like pharyngitis, tonsillitis, sinusitis, hypertrophy of the lymphoid follicles of tongue base, retroverted epiglottis, psychological factors and stress [3].
Even though finding a serious disease in patients with symptoms of globus pharyngeus is rare, a thorough work up is needed to rule out any life-threatening condition. The term globus was defined in the Oxford University Dictionary as ‘a choking sensation as of a lump in the throat to which hysterical persons are subject’. However, patients suffering from globus sensation have been found to have no higher scores for hysteria than healthy subjects and the term globus hystericus has been abandoned. Another term which has been used for this condition is globus pharyngis. Such patients require blood investigations like complete blood counts, erythrocyte sedimentation rate, general blood picture, throat endoscopy and radiological investigations. Barium swallow is one of the investigations which can rule out any organic pathology (like a mass lesion in the pyriform sinus or post cricoid region). It is a safe procedure with rare complications, like aspiration, if performed in inadequately assessed individuals. Another issue involved with this procedure is that of radiation exposure (approximately, 1.5 milliSieverts) and its subsequent sequela.
This study was conducted to assess the utility of barium swallow in patients with globus like symptoms and a normal ear, nose, throat examination.
Materials and Methods
A prospective study was conducted in the Department of ENT and Radiodiagnosis of a tertiary care hospital in the state of U.P. in India. Period of study was 12 months (October 2017 to September 2018). Ethical clearance was obtained from the Institute Ethics Committee (IEC number: 18/18; dated: 11/09/2018). Patients attending ENT OPD with complaints of lump in the throat, pain and sticking sensation for more than one month, of either gender, between the age of 18 and 60 years were included in the study after taking informed consent. Purposive sampling was done and all patients who fulfilled the inclusion criteria and consented to participate in the study were enrolled in the study. Recruitment of study participants was done in the defined study period of data collection. So, 100 patients were enrolled during the defined study period. All the patients underwent a detailed ENT examination. Patients with any abnormal finding on indirect laryngoscopy, patients with known pharyngeal, laryngeal or oesophageal disease, all those patients with previous contraindication to use of barium were also excluded. The selected subjects underwent barium swallow examination. This examination was done by a senior radiologist, of the designation of Associate Professor, have >15 years of experience. Throat endoscopy, complete blood counts and Erythrocyte Sedimentation Rate (ESR) estimation were done for all the patients.
Radiographic evaluation was done under digital fluoroscopy unit, Opera T 90 Ce (Prognosys). Initial screening of the pharynx was done in frontal and lateral projections in static and dynamic modes for symmetry, to rule out an abnormal displacement, adjacent abnormal soft tissue or radio-opaque foreign body. Dynamic manoeuvre consisted of modified valsalva in frontal and prolonged phonation “eee” in lateral projection. This was followed by barium swallow examination. Procedure was recorded with a fast cine loop for review afterwards. Examination begun in an upright position followed by a recumbent position for evaluation of the cricopharyngeal sphincter and oesophageal motility. Additional view, like an oblique view, was taken as per the findings. Barium suspension of 100 W/V was used. Higher density was preferred if double contrast examination was required.
Procedure
The patient holds a cup of barium, with a straw inside it. The barium is kept in the mouth till further instructions. On instruction, the patient swallows the barium and the procedure is recorded in cine mode, both in frontal and lateral projections. Spot films are taken. Evaluation of oesophagus is done in right anterior oblique position followed by evaluation in recumbent position.
Patients were started on empirical treatment based on the symptoms and examination findings.
Statistical Analysis
The data were analysed using statistical package SPSS version 23.0. Descriptive summary using frequencies, percentages and cross tabs were used to present the study results. Two tailed probability (p) was calculated to test the statistical significance at the 5% level of significance. Association between predictors (lump in throat, sticking sensation in throat, foreign body sensation in throat, throat pain) and outcome variables (normal barium swallow and abnormal barium swallow) was determined using chi-square test.
Results
Over a period of one year 100 subjects were studied. All subjects underwent barium swallow examination. Out of 100 patients, 43% were males and 57% were females. Mean age was 39.95 years. Barium swallow was found to be normal in 91 subjects and abnormal in nine subjects [Table/Fig-1]. Out of the cases with normal barium swallow, 36 had throat pain, 21 had sticking sensation in throat, 31 had feeling of lump in throat and 14 had burning sensation in throat. Majority of these were diagnosed with globus. Few had pharyngitis/ laryngitis and GERD.
Characteristics of patients and barium swallow results (n=100).
| Parameter | Frequency | Percentage | |
|---|
| Mean age (Years) | | | 39.95±11.94 |
|---|
| Gender | Male | 43 | 43.0 | |
| Females | 57 | 57.0 | |
| Barium swallow | Normal | 91 | 91.0 | |
| Abnormal | 9 | 9.0 | |
Most common complaint was feeling of lump in the throat. This was reported by 38 subjects followed by throat pain which was present in 36. Sticking sensation in the throat was complained by 21 and burning sensation was the complaint of 14 subjects.
Out of the 9 subjects with an abnormal finding on barium swallow, 6 (66.7%) had sticking sensation, 7 (77.8%) had feeling of lump while none of the subjects had burning sensation in the throat or pain. There was a statistically significant association (p<0.05) between barium swallow and clinical symptoms like throat pain, sticking sensation and feeling of lump in the throat [Table/Fig-2].
Association of clinical symptoms with barium swallow findings (n=100).
| Symptoms | Barium swallow findings | p-value |
|---|
| Normal | Abnormal |
|---|
| Throat pain | Present | 36 (39.6) | 0 (0) | 0.024 |
| Absent | 55 (60.4) | 9 (100) |
| Sticking sensation in the throat | Present | 21 (23.1) | 6 (66.7) | 0.011 |
| Absent | 70 (76.9) | 3 (33.3) |
| Feeling of lump | Present | 31 (34.1) | 7 (77.8) | 0.025 |
| Absent | 60 (65.9) | 2 (22.2) |
| Burning sensation | Present | 14 (15.4) | 0 (0) | 0.352 |
| Absent | 77 (84.6) | 9 (100) |
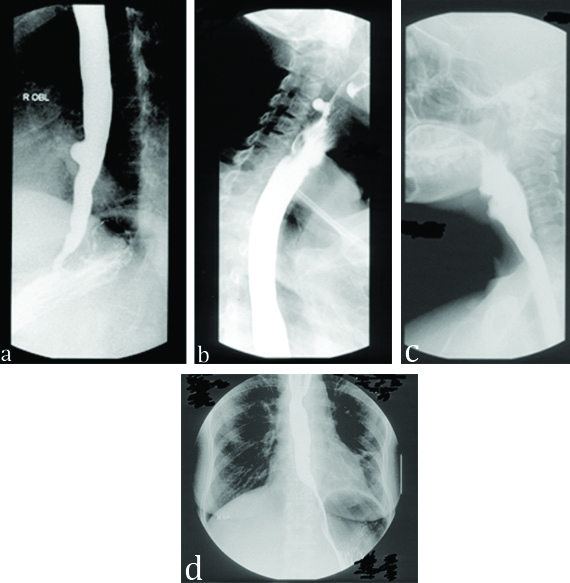
The most common barium swallow finding was epiphrenic diverticula which were seen in 3 individuals; 2 had pulsion diverticula, 1 subject each had an incomplete mitotic stricture, filling defect in post cricoid region, narrowing in mid oesophagus and post cricoid web. The [Table/Fig-3] shows few of the findings in patients with an abnormal barium swallow. These patients were referred to gastro-medicine department for further management.
a) Pulsion diverticulum; b) Pharyngeal pouch; c) Post cricoid web; d) Mid oesophagus incomplete stricture, which turned out to be mitotic.
Discussion
Globus pharyngeus is a painless and chronic condition, which is difficult to treat. Symptoms are usually relieved while eating. It is not commonly accompanied by odynophagia or dysphagia [8]. Even though it is a relatively common condition, no definite aetiology has been found. Various aetiological factors have been suggested, viz.
Psychosomatic problems: Certain psychological disturbances like depression, anxiety and stress can be present in patients with globus pharyngeus. Studies by Harris MB et al., and Thompson WG and Haeton KW, have shown globus symptoms to be preceded by a stressful life event [9,10]. As a patient with complaint of lump in the throat is first seen by an ENT specialist, psychological factor must be kept in mind and patient should be referred to a psychiatrist if needed
Gastroesophageal Reflux Disease (GERD): Several studies have indicated GERD as a causative factor in globus pharyngeus. Hill J et al., and Chevalier JM et al., have suggested that around 23%-68% cases of globus also suffer from reflux [11,12]. Malcomson KG, was the first to find a relation between GERD and feeling of lump in the throat [2].
Hypertonicity of Upper Oesophageal Sphincter (UES): Increased upper oesophageal sphincter pressure is also associated with globus symptoms [13].
Structural abnormalities: Hypertrophy of follicles over tongue base or a retroverted epiglottis touching the tongue base can also cause globus like symptoms [14,15]. Partial epiglottectomy relieves the patient [16].
Pharyngitis, tonsillitis and chronic sinusitis are some of the causes that need to be ruled out in patients complaining of lump in the throat.
There is a lack of consensus on any protocol for the diagnosis and management of globus pharyngeus. Many physicians prefer to judge clinically and prescribe symptomatic treatment like proton pump inhibitors, mood elevators and multi-vitamins. Some others perform a battery of tests to rule out any serious disease before starting treatment. In the present study Pantoprazole (40 mg) and Amitriptyline (10 mg) were given to the patients having globus, and the patients with an abnormal finding in barium swallow (nos. 9) were referred to the department of gastro-medicine for further management.
Barium swallow is an invaluable tool to study the anatomy and function of oral cavity, pharynx and oesophagus. It is a safe, easily available, inexpensive, non-invasive technique to assess the motility and morphological abnormalities of upper Gastrointestinal (GI) tract [17]. It also acts as a guide for further investigating a patient.
The earliest contrast study of GI tract was by Rumpel T, in the year 1897 [18]. He suggested the use of bismuth sub nitrate, but this contrast material was discarded as it converted to toxic bismuth sub nitrite. Later in the year 1904, Cannon WB, described the use of barium sulphate for GI fluoroscopy [19]. Barium sulphate is found in the natural mineral barite and is a white, odourless and crystalline substance. It has low water solubility and therefore can be used safely as a contrast agent for GI tract. Since 1910, barium has been the most widely used contrast agent for GI studies.
In this study female preponderance was seen which is similar to studies by Wall BF and Hart D, and Harar RP et al., [20,21]. In 1968, Malcomson KG, first observed a link between GERD and globus [2]. He reported that 63% patients of globus showed reflux in barium studies. Caylakli F et al., described in their study that 32% of patients of globus had cervical osteophytes, 7.2% had an oesophageal traction diverticulum and 5.7% had hiatus hernia [22]. These studies have reflected the importance of barium swallow in globus patients. In the present study, out of 100 subjects, 9 had an abnormal barium swallow. There was a significant association between barium swallow and clinical symptoms of globus pharyngeus after applying chi-square test and this is in concordance with the study of Caylakli F et al., [22]. This suggests that patients with symptoms of globus should undergo barium swallow to rule out other structural abnormalities as it is a simple, non-invasive and cost-effective modality.
Several studies have indicated GERD as a causative factor for globus pharyngeus [2,11,12]. Nevertheless, pH studies will be more useful in such cases. Other studies have stated psychomatic problems [9,10], hypertonicity of UES [13] and structural abnormalities [14,15] as a cause of globus.
This study has demonstrated the usefulness of barium swallow in patients of globus. It is suggested that barium swallow investigation should be done in patients of globus and then further management can be planned accordingly. Though the investigation involves radiation exposure and chance of aspiration, yet barium swallow helps in reassuring the patient and alleviating the anxiety of the patient.
Limitation
The results of this study underline the need for further high-quality evidence-based research especially from the developing world so that a better understanding of the role of this investigation in globus can be established. There is paucity of literature in this domain and this study generates important findings. However, the small sample size and selection of patients from one hospital limits the generalisation of results. With the rising problem of patients with globus, the issue needs to be addressed upon and this study indeed gave some useful information.
Conclusion
Globus pharyngeus is a chronic condition with a considerable burden in the developing world. The results of this study indicate that barium swallow can be used as an important tool in the management of patients with globus pharyngeus.