Introduction
Lack of quick and easy techniques to handle human identification devices during mass disasters like Indian Ocean earthquake and Tsunami (2004), Kedarnath landslide (2013), Kolkata market fire (2013), Chennai flood (2015), and Kerala flood (2018), emphasised on the necessity to develop this tool.
Aim
To develop a simple, yet reliable tool that can serve the purpose as a potential forensic record as well as patient data retrieval system.
Materials and Methods
In-vitro experiment was carried out by incorporation of passive radio frequency identification microchips into a cavity on lingual surface of 3 unit metal ceramic fixed partial denture models and sealing the cavity using ceramic repair kit. These thirty six fixed partial denture samples were divided into 12 samples of each three groups as group 1 -100°C, group 2 -200°C and group 3 -300°C. Viability of microchips before and after heat treatment using RenfertMagma Pre heating furnace of each group with a temperature holding time of 15 minutes was assessed using radio frequency identification device reader and values were computed. Statistics was computed using Pearson chi-square analysis. Scanning Electron Microscopic (SEM) analysis at a resolution of 500 μm was carried to study surface characteristics before and after heat treatment.
Results
In group 1 (100°C) and group 2 (200°C) microchips were found to be 100% viable before and after heat treatment. In case of group 3 (300°C), 100% of samples failed to read out after heat treatment. Since the values obtained in all the three groups before firing was constant; no statistical difference was computed. Likewise cross tabulation of values between before and after firing were constant; so no statistical differences were computed. Pearson chi-square analysis of after firing group values computed p-value <0.001 which is statistically significant. SEM analysis revealed disrupted composite-ceramic interface, disintegrated microchips with carbonization in group 3 samples.
Conclusion
Within constraints, successful development of limited heat resistant (up to 200°C) Radio Frequency Identification Device (RFID) incorporated fixed partial dentures was established. Further prospective studies are needed to improvise the heat resistance of this device.
Introduction
Human identification, whether in case of forensic or patient identification has always been a cumbersome process due to the condition of the remains such as advanced state of putrefaction, skeletonization, carbonization, incineration, defacement and so on, which leads to alteration of soft tissue, the abolition of fingerprints and DNA (Deoxyribonucleic acid) sequences or the lack of other essentials that clue to the positive or steadfast identification of the victims/personnel [1].
In India, some massive natural and man-made disasters have been witnessed in past decades, which lead to massive life loss, like in case of Indian heat wave (1998, 2009) there is 146% increase in the probability of mortality rate [2,3], Aircraft accident in Haryana (1996) lead to 80% death of passengers [4], Bhuj earthquake (2001) [5], Indian ocean earthquake and Tsunami caused more than 50% of mortality of victims (2004) [6], Kedarnath landslide (2013) [7], Kolkata market fire (2013) [8], Chennai flood (2015) [9], Gujarat flood (2017) [10], Kerala flood (2018) [11], Gaja cyclone (2018) [12] and so on.
During most of the massive life loss disasters, cumbersome forensic identification methods were followed and some victims even left unidentified as there was neither precise method of rapid human identification nor proper preservation or refrigeration facilities [6]. Rapid decomposition of victim’s body makes identification almost impossible within 24-48 hours of disaster. Most of the dead victims were buried without identification or noted as missing. This emergency situation despite the already existing distress adds more emotional distress to the surviving victims due to inappropriate disposal of the dead. The right of survivors to pay a final respect to their dead ones is deceived in such cases. This is an eye-opener for many forensic experts as such a challenging scenario required development of better and rapid human identification method in future for rapid recognition of an individual not merely to comply or for social responsibility to the deceased individual’s family but also to streamline the case from the judicial view point.
For decades forensic odontology has played a vital role in human identification. Teeth are well known to be the reliable forensic tool due to their ability to withstand extreme conditions and also due to protective nature of oral cavity [13]. There are numerous studies pertaining to human and dental identification like bite marks, palatal rugae pattern, salivary and teeth DNA analysis, denture markers (such as surface markers, inclusion method, lenticular card methodic band method, laser strip method, T bar method, laser etching, electronic microchips, Radio frequency identification microchips, lead foil…etc.,) [14-16].
RFIDs have been used for decades for purposes like shipment tracking, animal tracing [17] and also to monitor the diabetic blood glucose level in humans by injecting these chips sub dermally [18] and also researchers like Thevissen PW et al., [19,20] and Moreno F et al., [1] have earlier attempted to incorporate RFID microchips in human molars. Although these are in usage, there are studies pertaining to carcinogenic potential of these devices being in direct contact to the human or animal tissues [21]. Rather than invasively incorporating it into human tooth structure attempt was made to incorporate the microchips into FPDs thereby preserving natural tooth structure and also preventing unwanted pathological reactions.
On thorough looking into the history it is evident that studies pertaining to markers are predominantly limited only to removable prosthesis. However, in case of Fixed Partial Dentures (FPDs), there are not many documented studies apart from surface markers and micro etching. The smaller size of FPD and various heat processes such as casting during fabrication of FPD, have prevented incorporation of forensic tools in FPD by researchers over the years [22].
Materials used for removable prosthesis are mostly not heat stable under extreme temperatures. Removable prosthesis is readily dislodged from the oral structures during a natural calamity. Rather Fixed partial dentures are more stable and resistant to dislodgement forces and are comparatively heat resistant.
FPDs would also afford greater protection against extreme temperatures, acidic, damp and brackish salty environments. This would be useful in case of inhumation of cadavers or dismemberment of several individuals, done deliberately by crime committers to hinder the identification of victims. RFIDs implanted inside FPDs would stay in place even after dormant cadaveric phenomena and would decrease the likelihood of misperception among several RFIDs and their loss in the scene.
Based on the literatures available, it is also evident that in the recent years fixed treatment modalities are preferred over other treatment modalities and are more commonly practiced in majority of populace [23].
Hence the aim of the study was to develop a viable rapid human identification tool for forensic purpose as well as to serve as a patient data retrieval tool.
Objectives of the study were to fabricate a Human identification tool by incorporating passive RFID into 3-unit metal ceramic FPD. To check the viability and heat resistance of these devices under various temperatures before and after heat treatment and also to analyse the surface characteristics of these samples using SEM.
Materials and Methods
Sample Preparation
This in vitro study was carried out at the Department of Prosthodontics at SRM Dental College, Ramapuram, Chennai, Tamil Nadu, India during the period of December 2017-December 2018. Study was conducted after Institutional Review Board approval (IRB NO: SRMDC/IRB/2017/MDS/NO.201).
Pilot study was initially carried out to determine the sample size. Since this is a qualitative in vitro study, thirty six samples were found to be adequate with 2% margin of error, 99% confidence interval, and 50% sample size proportion. Randomization was done by random assignment of samples to the three groups.
Thirty six samples of three unit Metal ceramic FPD’s samples in relation to tooth regions 35, 36 and 37 keeping 36 as pontic was prepared for incorporation of microchips of dimension 1.25*7 mm. The microchips were incorporated inside a class V type cavity of dimension 1.5 mm depth 9 mm wide 1.5 mm length in lingual side of pontic in relation to 36 region.
Standardisation of samples was done by digital Computer Aided Designing (CAD) system. Teeth preparation was done on a typodont model (D18FE200-M-QF, Nissin, Kyoto, Japan) in relation to mandibular 35, 36 and 37 region keeping 36 as pontic. This was scanned using extra oral digital scanner (D2000, 3Shape, Copenhagen, Denmark).
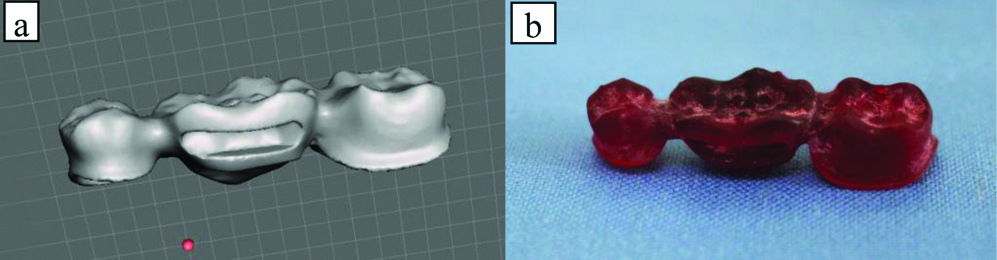
Designing was done using Fixed Partial Design Module (3Shape, Copenhagen, Denmark) [Table/Fig-1a]. This design was 3D printed using Sol Flex 350 with Sol Flex light curing premium cast resin [Table/Fig-1b].
(a) Computer-Assisted Designing (CAD) of FPD. (b) 3D printed castable resin pattern of FPD.
Printed resin pattern was conventionally casted. Sprue wax (Blue GEO Wax wire medium-hard, 2.0 mm, article no: 6783020) (Renfert, Germany) was attached to the 3D printed resin pattern. Phosphate bonded investment material (Bellavest® SH LOT: 0208547 (BEGO, Germany)) was used for investing the pattern.
After cooling of the invested pattern preheating was done in Renfert Magma (Pre heating furnace Ref: 230005000) starting at room temperature till it reaches the maximum temperature and then casted in Centrifugal Induction Melting Casting Machine (Fornax® T MPN: 26300).
Casted metal FPD’s were finished and polished followed by conventional ceramic overlaying done with IPS d.SIGN- (Ivoclar North America, Inc.) Dentin (Ref # 558216 Lot – v45262), Deep Dentin (Ref # 560512 Lot – W29689), Occlusal (Ref # 556587 Lot – U48501) Effect (Ref # 556594 Lot – w31675) Glaze (Lot: U23401). IvoclarVivadent furnace was used for ceramic firing. Finishing was done according to manufacturer instructions.
Cavity was sealed with commercially available Ceramic Repair Kit {(Ivoclar North America, Inc.)- Ceramic Repair N System Kit reference # 649118 AN Lot W31727 Exp 2019-03-01} after incorporation of microchips {CMRFID Microchip ISO 11784 / 11785, China} inside it [Table/Fig-2a-c].
(a) Casted and finished FPD metal substructure. (b) RFID placed inside Metal ceramic FPD. (c) RFID incorporated inside FPD and sealed with ceramic repair.

Methodology
Total of thirty six FPD samples were fabricated and included in the study. Heat treatment was carried out in RenfertMagma Pre heating furnace Ref: 230005000.
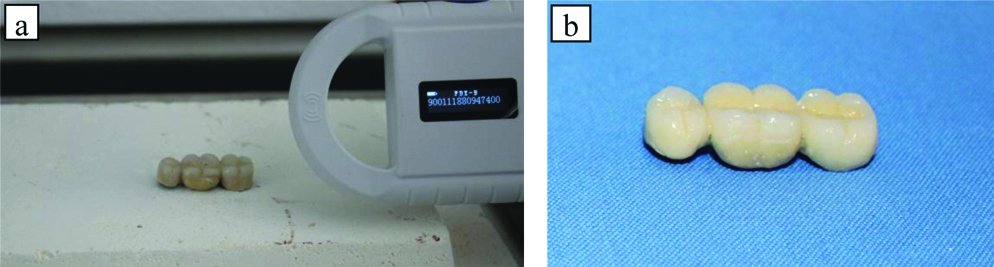
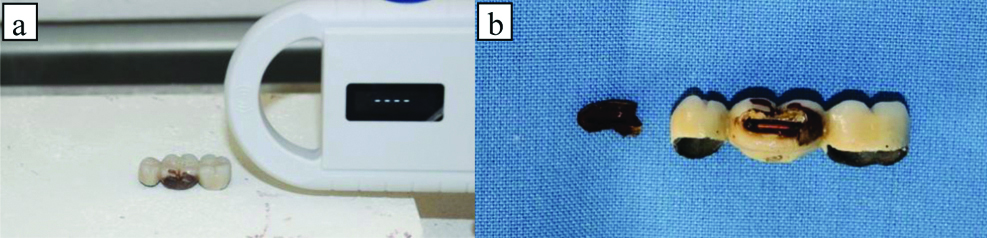
Impedance of all these samples was calculated before subjecting to heat treatment and also surface analysis was done using Scanning electron microscopy. The samples were divided into 3 groups as such Group 1- subjected to 100°C [Table/Fig-3], Group 2- subjected to 200°C [Table/Fig-4]. Group 3- subjected to 300°C [Table/Fig-5]. All these 3 groups were checked for sensitivity using radio frequency identification device reader at a distance of 4 inches [Table/Fig-6a,b,7a,b] and examined using SEM at a resolution of 500 μm after heat treatment with a holding time of 15 minutes.
Group 1: Readability at 100°C.
| Sample numbers | Encrypted numbers | Before firing | After firing |
|---|
| 1-12 | 900111880947361-72 | Read out | Read out |
Group 2: Readability at 200°C.
| Sample numbers | Encrypted numbers | Before firing | After firing |
|---|
| 13-24 | 900111880947373-84 | Read out | Read out |
Group 3: Readability at 300°C.
| Sample numbers | Encrypted numbers | Before firing | After firing |
|---|
| 25-36 | 900111880947385-96 | Read out | Failed to read out |
(a) Checked for viabilty before heat treatment. (b) FPD sample before firing.
(a) Checked for viability after heat treatment. (b) FPD sample after firing at 300°C.
Statistical Analysis
Statistics was computed using Pearson chi-square analysis separately for before firing [Table/Fig-8] and after firing [Table/Fig-9a,b] groups values. Values obtained for before firing was constant, so no statistical difference was computed. Pearson chi-square analysis of after firing group values computed p-value ≤0.001 [Table/Fig-9b] which was statistically significant. This signifies the successful development of device within constraints. Software used for statistical analysis was SPSS for windows (version 17.0).
Consolidated outcome of all three groups before firing.
| Group | Total |
|---|
| Group 1: At 100°C | Group 2: At 200°C | Group 3: At 300°C |
|---|
| Before firing read out count% Within group | 12100.0% | 12100.0% | 12100.0% | 36100.0% |
| Total count% Within group | 12100.0% | 12100.0% | 12100.0% | 36100.0% |
Consolidated outcome of all three groups after firing.
| Group | Total |
|---|
| Group 1: At 100°C | Group 2: At 200°C | Group 3: At 300°C |
|---|
| After firing read out count% Within group | 12100.0% | 12100.0% | 0.0% | 2466.7% |
| Failed to read out count% Within group | 0.0% | 0.0% | 12100.0% | 1233.3% |
| Total count% Within group | 12100.0% | 12100.0% | 12100.0% | 36100.0% |
After firing groups Pearson Chi-Square test value.
| Value | Df | Asymp. Sig (2-sided) |
|---|
| Pearson Chi-square | 36.000 | 2 | <0.001 |
| Likelihood ratio | 45.829 | 2 | <0.001 |
| Linear-by-Linear association | 26.250 | 1 | <0.001 |
| N of valid cases | 36 | | |
Results
Qualitative analysis to check viability of microchips before and after heat treatment using (RenfertMagma Pre heating furnace Ref: 230005000) was carried out. In group 1 (100°C) [Table/Fig-3] and group 2 (200°C) [Table/Fig-4] microchips were found to be 100% viable before and after heat treatment. In case of group 3 (300°C) [Table/Fig-5] 100% of samples failed to read out after heat treatment.
SEM at a resolution of 500 μm was carried out to analyse the surface characteristics of samples before and after heat treatment. Comparing the surface characteristics of samples before and after firing at 300°C, there is significant surface deterioration of composite and microchip after firing. Likewise disrupted composite and ceramic interface, exposure of the inner components of the microchip with carbonization of samples was also evident [Table/Fig-10a-d,11a-d]. This signifies the reason for deactivation of the microchip at 300°C.
(a) Before firing composite surface 0°C. (b) Before firing microchip surface 0°C. (c) Before firing composite ceramic interface 0°C. (d) Before firing metal surface 0°C.

(a) After firing composite surface 300°C. (b) After firing microchip surface 300°C. (c) After firing composite ceramic interface 300°C. (d) After firing metal surface 300°C.

Discussion
This study aimed to develop a viable rapid human identification tool for forensic as well as patient data retrieval applications. This tool was developed by incorporating passive RFID into 3-unit metal ceramic Fixed Partial Dentures. Viability and heat resistance of these devices under various temperatures before and after heat treatment were evaluated and also the surface characteristics of these samples were analysed by SEM.
In order to fabricate this RFID incorporated fixed partial denture tool, passive RFID are preferred rather than active to avoid potential pathological complication and radiation hazard due to constant active state. If active RFIDs are used there are chances of leaching out of ions due to active state whereas passive RFIDs will get activated only when its antenna comes in contact with specific electromagnetic field with low power and modulated amplitude with a resonance electronic artifact made up of a receptor, a capacitor and an antenna for transmission. Once activated with a frequency range of 134.2 KHZ the code stored in microchip is amplified to be converted to a decrypted digital format which is shown on liquid crystal screen display of scanner [24,25]. This passive nature of RFID until activated eliminates the risk of unnecessary radiation hazards. The RFIDs are incorporated within the metal ceramic FPD pontic in class V type cavity and filled with composite resin. Fracture of metal ceramic FPD or debonding of composite resin in such region (class V cavity of pontic) under occlusal load is an extremely unlikely event. However, accidental swallowing of RFID chip due to breakdown of composite resin bond will not lead to leach of harmful compounds in stomach as this RFID is encapsulated in acid-insulation and hence will not get disintegrated by gastric juices. Further research is required in future to investigate the bio-inertness of these chips under various in vivo scenarios.
RFID capsule has laser engraved 15 digit code for Identification (ID) stored on the microchip prior to its assembly. It can also be customised with numbers like national identification number and patient registration number during manufacturing. RFID antenna is made of ferrite core wrapped by copper wire coil which receives and transmits signals to and fro the reader. RFID capacitor receives the necessary voltage from the scanner to allow the microchip to actuate and transmit the ID code [26,27]. Burnout furnace was preferred to test the heat resistance of microchip incorporated FPD since they are standardised instruments with standard specifications and also they maintain uniform temperature cycle.
Temperatures withstand ability of various dental restoration according to literature for composites, metal and metal ceramic restorations range from room temperature to 1100°C [28].
The RFID microchip manufactures proposed operation temperature in range of -45°C to +85°C [29]. However, results of the study revealed much higher heat resistance of the microchips and its readability. Until 200°C the microchip was viable without any compromise in readability and also there was no drastic visible change in the appearance of surface of composite and ceramic overlaying the microchip. However, after the end of 300°C firing cycle, there was visible surface deterioration along with detachment of composite from the ceramic surface exposing the microchip directly to the heat thereby visible alteration in the surface characteristics of microchips was observed and they failed to read out at the end of 300°C. SEM analysis comparing before and after samples showed failure of bonding of ceramic and composite after firing. Exposure of the inner carbonised components of the microchips was also evident after heat treatment. Deterioration of the surface of composite and microchip was observed with intact metal and ceramic surfaces. Failure of the chip was inferred to be mainly due to exposure of microchip to direct heat after breakage of ceramic composite interface.
Statistical analysis was not so significant for before firing group since the values obtained were constant. However Pearson chi-square analysis after heat treatment inferred significant p-value less than 0.001.
Limitation
Heat resistance of microchips achieved is only up to 200°C. Failure of readability of microchip seems to be predominantly due to disintegration of bonding between composite and metal interface which lead to dispersion of heat onto the implanted microchip and dislodgement. Further prospective studies like coating the chip with biocompatible fire insulators, incorporation of insulated microchip within wax pattern before casting are needed to improvise the device. Continued research is needed to develop a more heat resistant RFID Human Identification Tool.
Future Recommendation
This is an in vitro study. Further in vivo studies are needed to further validate this tool before its use in humans. The current in vitro study results are encouraging in the aspects of readability and data retrieval. Also, the use of the device in massive fire situations is still questionable. Materials used for fixed partial denture fabrication are scientifically proven to be resistant to solubility, compressive, tensile and flexural forces [30,31]. Hence, this device can effectively be used in all kinds of natural and man-made disasters. Fire disaster scenarios involving extensive/complete destruction of human remains require much more heat resistant chip. And hence this device needs improvisation in terms of thermal insulation. Following the validation through in vivo studies for bio-inertness of the tool, this device can be used as a forensic tool for humans in future.
Conclusion
Successful development of potential Human identification tool was done by incorporating RFID in 3 unit metal ceramic fixed partial denture. Under laboratory conditions within limitations, heat testing of samples revealed temperature resistance of up to 200°C with better readability which is comparatively higher than the manufacturer specified operation temperature range of -45°C to +85°C.
Heat treatment at 300°C resulted in failure of the readability of the chips. SEM analysis revealed definitive surface alteration at 300°C with deterioration of composite and microchips with increased carbonization when compared to lesser heat treatment images.
Within limitations these RFID incorporated fixed partial dentures can serve as a potential forensic human identification as well as effective patient data retrieval tool.
[1]. Moreno F, Vallejo D, Garzón H, Moreno S, In vitro evaluation of a passive radio frequency identification microchip implanted in human molars subjected to compression forces, for forensic purposes of human identificationJ Forensic Dent Sci 2013 5(2):77-84.10.4103/0975-1475.11976624255554 [Google Scholar] [CrossRef] [PubMed]
[2]. De US, Mukhopadhyay RK, Severe heat wave over the Indian subcontinent in 1998, in perspective of global climateCurr Sci 1998 75(12):1308-11. [Google Scholar]
[3]. Mazdiyasni O, AghaKouchak A, Davis SJ, Madadgar S, Mehran A, Ragno E, Increasing probability of mortality during Indian heat wavesSci Adv 2017 3(6):01-05.10.1126/sciadv.170006628630921 [Google Scholar] [CrossRef] [PubMed]
[4]. Jenamani RK, Kumar A, Bad weather and aircraft accidents-global vis-à-vis Indian scenarioCurr Sci 2013 104(3):316-25. [Google Scholar]
[5]. Rastogi BK, Gupta HK, Mandal P, Satyanarayana HV, Kousalya M, Raghavan R, The deadliest stable continental region earthquake occurred near Bhuj on 26 January 2001J Seismol 2001 5(4):609-15.10.1023/A:1012228507533 [Google Scholar] [CrossRef]
[6]. Morgan OW, Sribanditmongkol P, Perera C, Sulasmi Y, Van Alphen D, Sondorp E, Mass fatality management following the South Asian tsunami disaster: case studies in Thailand, Indonesia, and Sri LankaPLoS Med 2006 3(6):19510.1371/journal.pmed.003019516737348 [Google Scholar] [CrossRef] [PubMed]
[7]. Sridharan R, Das TP, Ahmed SM, Bhardwaj A, Lessons from Kedarnath tragedy of Uttarakhand Himalaya, IndiaCurr Sci 2013 105(11):1472 [Google Scholar]
[8]. Albis KA, Radhwi MN, Gawad AF, Fire dynamics simulation and evacuation for a large shopping center (Mall): Part I, fire simulation scenariosAmerican Journal of Energy Engineering. Special Issue: Fire, Energy and Thermal Real-life Challenges 2015 3(4-1):52-71.http://www.journalenergy.org/article/168/10.11648.j.ajee.s.2015030401.1410.11648/j.ajee.s.2015030401.14 [Google Scholar] [CrossRef]
[9]. Jameson S, Baud IS, Varieties of knowledge for assembling an urban flood management governance configuration in Chennai, IndiaHabitatin 2016 54:112-23.10.1016/j.habitatint.2015.12.015 [Google Scholar] [CrossRef]
[10]. Samaddar S, Okada N, Choi J, Tatano H, What constitutes successful participatory disaster risk management? Insights from post-earthquake reconstruction work in rural Gujarat, IndiaNat Hazards 2017 85(1):111-38.10.1007/s11069-016-2564-x [Google Scholar] [CrossRef]
[11]. Mishra V, Aaadhar S, Shah H, Kumar R, Pattanaik DR, Tiwari AD, The Kerala flood of 2018: combined impact of extreme rainfall and reservoir storageHydrol Earth Syst Sci Discuss 2018 :01-13.10.5194/hess-2018-480 [Google Scholar] [CrossRef]
[12]. Thomas M, Cyclone Gaja leaves at least 45 dead in southern IndiaQuartz India 2019 [Google Scholar]
[13]. Prajapati G, Sarode SC, Sarode GS, Shelke P, Awan KH, Patil S, Role of forensic odontology in the identification of victims of major mass disasters across the world: A systematic reviewPLoS One 2018 13(6):0199791https://journals.plos.org/plosone/article?id=10.1371/journal.pone.019979110.1371/journal.pone.019979129953497 [Google Scholar] [CrossRef] [PubMed]
[14]. Barua DR, Changmai A, Gaurav A, Role of a prosthodontist in forensic dentistry-a step towards evolutionJ Clin Diagn Res 2018 12(9):ZE01-03.10.7860/JCDR/2018/35881.11988 [Google Scholar] [CrossRef]
[15]. Kareker N, Aras M, Chitre V, A review on denture marking systems: a mark in forensic dentistryJ Indian Prosthodont Soc 2014 14(1):04-13.10.1007/s13191-014-0363-126199485 [Google Scholar] [CrossRef] [PubMed]
[16]. Millet C, Jeannin C, Incorporation of microchips to facilitate denture identification by radio frequency taggingJ Prosthet Dent 2004 92(6):588-90.10.1016/j.prosdent.2004.07.02515583569 [Google Scholar] [CrossRef] [PubMed]
[17]. Iserbyt A, Griffioen M, Borremans B, Eens M, Müller W, How to quantify animal activity from radio-frequency identification (RFID) recordingsEcol Evol 2018 8(20):10166-74.10.1002/ece3.449130397456 [Google Scholar] [CrossRef] [PubMed]
[18]. Podaima BW, Friesen M, McLeod RD, A review of emerging smart RFID in healthcareCMBES Proceedings 2018 33(1) [Google Scholar]
[19]. Thevissen PW, Poelman G, De Cooman M, Puers R, Willems G, Implantation of an RFID-tag into human molars to reduce hard forensic identification labor. Part I: Working principleForensic Sci Int 2006 159:S33-39.10.1016/j.forsciint.2006.02.02916563681 [Google Scholar] [CrossRef] [PubMed]
[20]. Thevissen PW, Poelman G, De Cooman M, Puers R, Willems G, Implantation of an RFID-tag into human molars to reduce hard forensic identification labor. Part 2: Physical propertiesForensic Sci Int 2006 159:S40-46.10.1016/j.forsciint.2006.02.03016554132 [Google Scholar] [CrossRef] [PubMed]
[21]. Vascellari M, Mutinelli F, Cossettini R, Altinier E, Liposarcoma at the site of an implanted microchip in a dogVet J 2004 168(2):188-90.10.1016/S1090-0233(03)00121-7 [Google Scholar] [CrossRef]
[22]. Kamath PG, Kamath VG, Engraved fixed restorations and denture micro-labelling to facilitate identification through forensic dentistryJ Indian Prosthodont Soc 2005 5(2):7910.4103/0972-4052.16874 [Google Scholar] [CrossRef]
[23]. Zitzmann NU, Hagmann E, Weiger R, What is the prevalence of various types of prosthetic dental restorations in Europe?Clin Oral Implants Res 2007 18:20-33.10.1111/j.1600-0501.2007.01435.x17594367 [Google Scholar] [CrossRef] [PubMed]
[24]. Garfinkel S, Holtzman H, Understanding RFID technologyRFID 2006 :15-36. [Google Scholar]
[25]. Chawla V, Ha DS, An overview of passive RFIDIEEE Communications Magazine 2007 45(9):11-17.10.1109/MCOM.2007.4342873 [Google Scholar] [CrossRef]
[26]. Jin C, Zhang J, Li X, Yang X, Li J, Liu J, Injectable 3-D fabrication of medical electronics at the target biological tissuesSci Rep 2013 3:344210.1038/srep0344224309385 [Google Scholar] [CrossRef] [PubMed]
[27]. Voulodimos AS, Patrikakis CZ, Sideridis AB, Ntafis VA, Xylouri EM, A complete farm management system based on animal identification using RFID technologyComput Electron Agric 2010 70(2):380-88.10.1016/j.compag.2009.07.009 [Google Scholar] [CrossRef]
[28]. Patidar KA, Parwani R, Wanjari S, Effects of high temperature on different restorations in forensic identification: Dental samples and mandibleJ Forensic Dent Sci 2010 2(1):3710.4103/0974-2948.7105621189989 [Google Scholar] [CrossRef] [PubMed]
[29]. EM Microelectronic, 512 bit Read/Write Multi-purpose Contactless Identification Device EM4205/4305 2018 https://www.emmicroelectronic.com/product/lf-animal-access-ics/em42054305 [Google Scholar]
[30]. Lüthy H, Filser F, Loeffel O, Schumacher M, Gauckler LJ, Hammerle CH, Strengthand reliability of four-unit all-ceramic posterior bridgesDent Mater 2005 21(10):930-37.10.1016/j.dental.2004.11.01215923031 [Google Scholar] [CrossRef] [PubMed]
[31]. Lopez-Suarez C, Tobar C, Sola-Ruiz MF, Pelaez J, Suarez MJ, Effect of thermomechanical and static loading on the load to fracture of metal-ceramic, monolithic, and veneered zirconia posterior fixed partial denturesJ Prosthodont 2019 28(2):171-78.10.1111/jopr.1300830548895 [Google Scholar] [CrossRef] [PubMed]