Reconstruction of Scalp Avulsion in a Resource Restraint Rural Hospital
Rudra Rajesh Nair1, Shweta Shaji Mathew2, Anna Mary Jose3, Suhas Jajoo4, Samarth Shukla5
1 Third Year MBBS Student, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
2 Third Year MBBS Student, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
3 Third Year MBBS Student, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
4 Professor, Department of Surgery, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
5 Professor, Department of Pathology, Datta Meghe Institute of Medical Sciences, Wardha, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Ms. Shweta Shaji Mathew, Shardha Hostel, Datta Meghe Institute of Medical Sciences, Wardha, Mahrashtra, India.
E-mail: shwetashaji98@gmail.com
Occupational hazard is a major contributing factor to various deformities that workers who work with machines are subjected to, especially when the machines are rotating and are unprotected. Women workers with long hair not capped or tied appropriately may become a victim of moving or rotating machines, when the hair gets caught in the rotating part of the machine causing avulsion of the scalp.
Scalp avulsion may lead to loss of life, disfigurement, require hospitalisation as well as psychological harm to the person. We present a case managed practically in a rural based hospital of a young girl, who had a complete scalp avulsion, and the challenges that were faced in a setting where microvascular surgery was not an option. It was treated with debridement and a simple split skin graft to cover the wound.
Absence of microvascular surgery, Rotatory machine, Split skin graft, Traumatic disfigurement
Case Report
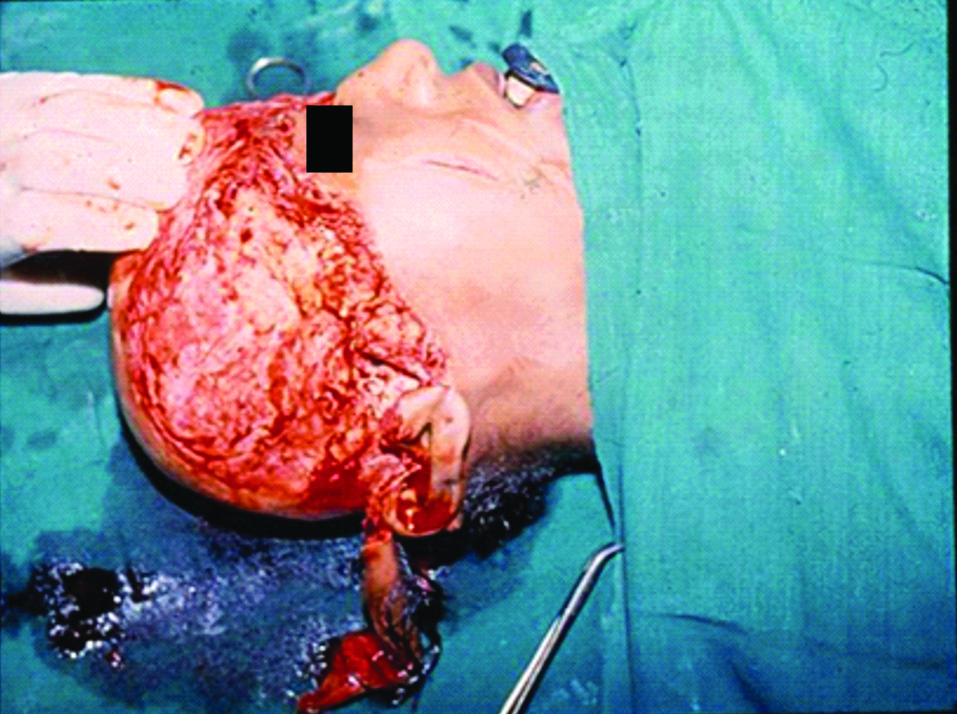
A 20-year-old young woman reported to the emergency department with an avulsed scalp. The accident occurred 30 minutes prior, wherein her hair got caught in the rotating part of the flour mill resulting in the avulsion as well as loss of eyebrows. Immediately resuscitation was started and blood loss was controlled. Assessment for intracranial injury was done. It was found that pericranium was intact, pinna were avulsed partially and eyebrows were avulsed totally [Table/Fig-1,2]. Debridement was done, pinna was placed in proper anatomical position and sutured, and scalp was split skin grafted. The split skin graft was taken out from the thigh and sutured into the defect. The donor wound was dressed, which healed within 15 days. The graft was taken up completely. The required large flaps and free flap facilities were not available. Split skin graft was a short procedure with minimum blood loss, and was thus chosen.
Anterior view of avulsed scalp including the eyebrows.

Lateral view of avulsed scalp with partial involvement of pinna.
Recovery was dramatic and satisfactory. She was advised to have eyebrow pencilled, scalp covered with a wig and to use a large dark goggle. This helped to cover the deformity to the maximum and only forehead was visible. Due to the camouflaging, the ultimate look was presentable [Table/Fig-3]. She later got married, had two children and went on to lead a normal life.
Post-op photograph. Patient was advised to wear a wig and have her eyebrows pencilled so as to regain a normal appearance.

Discussion
The scalp is a soft tissue envelope of the cranial vault. It extends from the top of the forehead in front to the superior nuchal line behind. Laterally, it projects down to the zygomatic arch and external acoustic meatus. The overlying skin, subcutaneous tissue, occipitofrontalis, act as a single unit and can move along the loose areolar tissue over the pericranium. In scalp avulsion injury, scalp usually separates at the level of loose areolar tissue, which is relatively avascular, but edges can bleed [1].
Avulsion mostly results from the entrapment of long hair or cloth in high speed rotary parts of machinery, although it has also occurred as result of animal attacks, road traffic accidents and assaults [2,3]. It is usually associated with significant co-morbidities. During avulsions, the line of tear follow the path of least resistance i.e., along the insertions of the frontalis and temporalis muscle anteriorly and occipitals muscle posteriorly [4,5]. The avulsed portion may include the eyebrows as well as all or part of the ears. The deep plane of cleavage is generally through the loose connective tissue between the galea aponeurotic and the pericranium, occasionally including part or all of the pericranium.
Large defects in the absence of microvascular facilities need drill holes in diploe for granulation tissue to grow, which can be grafted later, such as was done in a case of a 10-year-old who had her scalp completely avulsed by an agricultural machine. Multiple trephination of the calvarium was performed to expose the diploe. Granulation tissue from the holes began to cover the defect after four weeks, allowing the formation of a vascular bed suitable for skin grafting [6]. Another case, wherein a 15-year-old following a road accident presented with a 12×5 cm lacerated wound, which was managed by layer wise suturing of galea aponeurotic with 3-0 vicryl. Aesthetic closure of skin was done with 2-0 ethilon with horizontal mattress sutures the laceration which was concealed in hair and was not visible outside. Large scalp defects which are devoid of a vascular bed for a full thickness skin graft, are ideal for split thickness skin grafts [7]. Split thickness skin grafts may be taken from any area of the body, including the scalp, although the donor site is frequently scarred and discoloured [8,9]. If a free flap option is available, then it should be preferred. Free tissue transfers like latissimus dorsi with serratus anterior free flaps, free parascapular flap or free omental transfer with split skin graft over it, may also be a good choice for soft tissue coverage of the skull. If not, then skull bone is burred at multiple sites up to diploe, granulation tissue comes out over the bone from those burr holes which is then split skin grafted [6]. Such scalp reconstruction has been proven successful in a majority of the patients [10-12] with a stable soft tissue cover, low complication rate and satisfactory cosmesis as in our case.
Conclusion
In a rural hospital where the limitations are set by the financial status, time as well as limited infrastructure and expertise to deal with microsurgery, split thickness skin graft is the preferred approach. Wherein technology driven medical science is reducing the skills of general surgeons and making the treatment cost out of reach for common man, we have tried to treat all varieties of patients by those techniques which can easily be learnt by general surgeons and can be made available to common man nearby his residence at an affordable cost.
Declaration: This case was presented as a conference poster.
Author Declaration:
Financial or Other Competing Interests: No
Was informed consent obtained from the subjects involved in the study? Yes
For any images presented appropriate consent has been obtained from the subjects. Yes
Plagiarism Checking Methods: [Jain H et al.]
Plagiarism X-checker: May 04, 2019
Manual Googling: Jul 30, 2019
iThenticate Software: Sep 04, 2019 (8%)
[1]. Leedy JE, Janis JE, Rohrich RJ, Reconstruction of acquired scalp defects: An algorithmic approachPlast Reconstr Surg 2005 116:54e-72e.10.1097/01.prs.0000179188.25019.6c16163072 [Google Scholar] [CrossRef] [PubMed]
[2]. Yin JW, Matsuo JMS, Hsieh CH, Yeh MC, Liao WC, Jeng SF, Replantation of total avulsed scalp with microsurgery: Experience of eight cases and literature reviewJ Trauma 2008 64:796-802.10.1097/TA.0b013e3180341fdb18332826 [Google Scholar] [CrossRef] [PubMed]
[3]. Ozek C, Guner U, Bilkay U, Alper M, Akin Y, Cagdas A, Superficial scalp necrosis after replantationAnn Plast Burg 2001 46:197-98.10.1097/00000637-200102000-0003111216629 [Google Scholar] [CrossRef] [PubMed]
[4]. Borenstein A, Yaffe B, Seidman DS, Tsur H, Microsurgical replantation of two totally avulsed scalpsSir J Med Sci 1990 26:442-45. [Google Scholar]
[5]. Ohara-Sppert M, Mullaly SG, Nursing care of the patient with a complete scalp avulsionJ Emerg Nurs 1996 22:552-59.10.1016/S0099-1767(96)80211-X [Google Scholar] [CrossRef]
[6]. Furlanetti LL, de Oliviera RS, Santos MV, Farina JA, Jr, Machado HR, Multiple cranial burr holes as an alternative treatment for total scalp avulsionChilds Nerv Syst 2010 26:745-49.10.1007/s00381-010-1145-720390420 [Google Scholar] [CrossRef] [PubMed]
[7]. Alvi S, Ghazal Asswad R, Jenzer AC, Scalp Reconstruction. [Updated 2019 Apr 30]In: StatPearls [Internet] 2019 Jan Treasure Island (FL)StatPearls PublishingAvailable from: https://www.ncbi.nlm.nih.gov/books/NBK539788/10.1093/jscr/rjz01730788097 [Google Scholar] [CrossRef] [PubMed]
[8]. Muhlstadt M, Thomé C, Kunte C, Rapid wound healing of scalp wounds devoid of periosteum with milling of the outer table and split-thickness skin graftingBritish Journal of Dermatology 2012 167(2):343-47.10.1111/j.1365-2133.2012.10999.x22512740 [Google Scholar] [CrossRef] [PubMed]
[9]. Sokoya M, Inman J, Ducic Y, Scalp and forehead reconstructionSemin Plast Surg 2018 32(2):90-94.doi: 10.1055/s-0038-1642638. Epub 2018 May 14. PubMed PMID: 29765273; PubMed Central PMCID: PMC5951698 [Google Scholar]
[10]. Akheel M, Tomar SS, Bumb SS, Emergency esthetic closure of scalp in a rural set up: A case reportIJSS Journal of Surgery 2015 2:12-14. [Google Scholar]
[11]. Ahmad M, Hussain S, Malik SA, Long scarf: A rare cause of scalp avulsion injuriesRawal Medical Journal 2009 34:229-30. [Google Scholar]
[12]. Aldabagh B, Cook JL, Reconstruction of scalp wounds with exposed calvarium using a local flap and a split-thickness skin graft: case series of 20 patientsDermatol Surg 2014 40(3):257-65.10.1111/dsu.1241224438208 [Google Scholar] [CrossRef] [PubMed]