Pathologists rarely receive an ideal specimen with the necessary clinical data or sufficient tissue to supplement or support the histologic diagnosis. Inadvertent omission of pertinent clinical information deter pathologist to visualise the site and nature of the lesion. Other errors arise during the gross examination of the specimens in the pre-analytic phase due to the physical recording of macroscopic features which is mostly subjective and inadequate [1]. There is a need of a “gold standard” approach and an instrument to record the macroscopic features of specimens during the gross examination to reduce the incidence of errors in the pre-analytic phase of tissue processing [2].
The present study evaluates the utility of stereozoom microscope in gross examination of biopsy specimens and the potential application of stereozoom microscope to bridge the gap between clinical and histologic diagnosis.
Materials and Methods
The present study was an evaluation study on the utility of stereozoom microscope as a potential instrument in gross examination of biopsy specimens. A total of thirty biopsy specimens received in the Department of Oral Pathology and Oral Microbiology, Vinayaka Mission’s Sankarachariyar Dental College, Salem from the period of October 2018 to March 2019 was utilised in this study. Prior to commencing the study, ethical clearance was obtained from the Institutional Ethics Committee of the respective institution where the study was conducted (VMSDC/IEC/Approval no.068). Based on the provisional diagnosis in the biopsy requisition forms, the specimens were classified according to the type of tissue and nature of pathology [Table/Fig-1]. Convenience sampling was done for the study.
Specimens classified according to the type of tissue and nature of pathology.
| Provisional diagnosis | Specimen numbers |
|---|
| Epithelial tumours (6) |
| Oral squamous cell carcinoma | 3 |
| Verrucous carcinoma | 2 |
| Leukoplakia | 1 |
| Lymph node (2) |
| Lymph node (from the excisional biopsy of oral squamous cell carcinoma) | 1 |
| Lymph node (from the excisional biopsy of ameloblastic carcinoma) | 1 |
| Connective tissue tumours (7) |
| Neurofibroma | 1 |
| Ossifying fibroma | 2 |
| Fibroma | 3 |
| Capillary haemangioma | 1 |
| Odontogenic tumours (5) |
| Ameloblastoma | 3 |
| Ameloblastic carcinoma (incisional) | 1 |
| Ameloblastic carcinoma (excisional) | 1 |
| Odontogenic cysts (4) |
| Gingival cyst of newborn | 1 |
| Orthokeratinzed keratocyst | 1 |
| Periapical cyst | 2 |
| Inflammatory lesions (6) |
| Pyogenic granuloma | 3 |
| Peripheral giant cell granuloma | 1 |
| Osteomyelitis | 1 |
| Chronic ulcer | 1 |
| Total | 30 |
Inclusion criteria: Soft tissue specimens from the oral cavity by incisional biopsy and lymph nodes taken from an excisional biopsy specimen were included in the study.
Exclusion criteria: Hard tissue specimens, specimens obtained from outside the oral cavity were excluded from the study, specimens submitted without sufficient clinical data or provisional diagnosis.
All the specimens that matched the above criteria were gross examined by three observers without and with the stereozoom microscope and the macroscopic features were recorded and entered in separate data entry sheets, 1 and 2. One observer was an Oral Pathologist with seven years of experience following post-graduation and the two observers were postgraduate trainees specialising in the field of Oral Pathology and Oral Microbiology. The stereozoom microscope (OptoMag Stereozoom microscope, KOM 23E) of Greenough design with a magnification of 0.7x to 4.5x was utilised to gross examine the biopsy specimens. For photography, a digital camera (Kodak) with 9 MP resolution was used to take photographs of the biopsy specimens. The gross examination without the stereomicroscope was performed by placing the specimen on a green cloth with two metal scales placed perpendicular to each other with one scale from the marking zero and the other at the approximate size of the specimens. The observer was to view, record the macroscopic features in data entry sheet 1 and to take photographs of the specimen using the digital camera mentioned above. The gross examination with the stereomicroscope was performed by placing the specimen on a transparent rectangular disposable plastic sheet of 3.5×4 cm fixed by the stage clips. The observers were to view, record the macroscopic features in data entry sheet 2 and take the photograph using the digital camera mentioned above. Following the gross examination, the observers were required to answer a questionnaire provided to them. Questionnaire was prepared by the authors and validated by the speciality experts before using it for the present study. The questionnaire consisted of 33 questions [Table/Fig-2] categorised as:
| S. No. | With stereomicroscope | 1 | 2 | 3 | 4 | 5 |
|---|
| 1. | General visibility | | | | | |
| 2. | Colour apprehension | | | | | |
| 3. | Observation of macroscopic features | | | | | |
| 4. | Appreciation or border or extent | | | | | |
| 5. | Identification of normal tissue | | | | | |
| 6. | Identification of abnormal tissue | | | | | |
| 7. | Supplement in dissecting the area of suspicion | | | | | |
| 8. | Orient the histology section in the specimen | | | | | |
| 9. | Relate the histology features seen in sections with specimens | | | | | |
| 10. | Facilitate in rendering diagnosis | | | | | |
| Unaided eye | 1 | 2 | 3 | 4 | 5 |
| 11. | General visibility | | | | | |
| 12. | Colour apprehension | | | | | |
| 13. | Observation of macroscopic features | | | | | |
| 14. | Appreciation or border or extent | | | | | |
| 15. | Identification of normal tissue | | | | | |
| 16. | Identification of abnormal tissue | | | | | |
| 17. | Supplement in dissecting the area of suspicion | | | | | |
| 18. | Orient the histology section in the specimen | | | | | |
| 19. | Relate the histology features seen in sections with specimens | | | | | |
| 20. | Facilitate in rendering diagnosis | | | | | |
| Operation of stereomicroscope | 1 | 2 | 3 | 4 | 5 |
| 21. | General easy to operate | | | | | |
| 22. | Easy to take photographs | | | | | |
| 23. | Ability to photograph details observed | | | | | |
| 24. | Easy to move specimens on stage | | | | | |
| 25. | Easy to zoom/magnify the specimens | | | | | |
| Preference of stereomicroscope use | 1 | 2 | 3 | 4 | 5 |
| 26. | General visibility | | | | | |
| 27. | Colour apprehension | | | | | |
| 28. | Observation of macroscopic features | | | | | |
| 29. | Appreciation or border or extent | | | | | |
| 30. | Identification of normal tissue | | | | | |
| 31. | Identification of abnormal tissue | | | | | |
| 32. | Supplement in dissecting the area of suspicion | | | | | |
| 33. | Based on the above features, would you use stereomicroscope for gross examination | | | | | |
1: Very Good; 2: Good; 3: Average; 4: Poor; 5: Very Poor
Gross examination with Stereomicroscope (Question 1-10);
Gross examination without Stereomicroscope (Question 11-20);
Operation of Stereomicroscope (Question 21-25);
Preference of Stereomicroscope over conventional method (Question 26-33).
Statistical Analysis
The Likert scale questionnaire data by the observers were entered into an excel sheet (MS Excel 2013). The statistical analysis was performed using SPSS Version 19.0 software (IBM SPSS, US). The Chi-square test was applied to compare the responses made by three observers with respect to use of stereomicroscope, operation and its preference in gross examination and the p-value <0.001 was considered significant.
Results
The total number of biopsy specimens taken in our study was 30 which included neoplastic (66.7%) and inflammatory conditions (33.3%) affecting the oral cavity. The results of the different parameters with regard to macroscopic examination, operation and preference of use of stereozoom microscope along with the p-values have been shown in [Table/Fig-3,4,5 and 6], respectively. Significance levels were set at 5% significant and 1% highly significant level using the Chi-square test. In gross examination using a stereozoom microscope [Table/Fig-3], all three observers had favoured a very good to good for questions 1 to 10 pertaining to parameters considered in macroscopic viewing and recording. A statistical difference was found between three observers with regard to supplementing in dissecting the area of suspicion (p<0.001), relating the histological features seen in sections with specimens (p<0.001) and to facilitate in rendering a diagnosis (p<0.001). While in the gross examination without the stereozoom microscope, the overall response ranged from poor to average for questions 11 to 18 and 20 and very poor for question 19 for the same specimens and parameters. A statistical difference was found between three observers with regard to general visibility (p<0.001), observation of macroscopic features (p<0.003), appreciation of border or extent (p<0.001), relate the histology features seen in sections with specimens (p<0.001) and facilitate in rendering diagnosis (p<0.002) [Table/Fig-4]. With regard to operating the stereozoom microscope, all three observers had given an overall response of very good to good for questions 21 to 25 with a statistical difference found between the three observers in ease to move specimens on stage (p<0.001), ease to zoom/magnify the specimens (p<0.001) [Table/Fig-5]. All three observers had given a response of very good to good for questions 26 to 33 pertaining to the preference of use of the stereozoom microscope for examining biopsy specimens with statistical difference observed in appreciation or border or extent (p<0.045), identification of abnormal tissue (p<0.032) and supplementing in dissecting the area of suspicion (p<0.001) [Table/Fig-6].
Macroscopic examination utilising stereozoom microscope (Chi-Square test).
| Observer | Total | Chi-square | p-value |
|---|
| OB 1 | OB 2 | OB 3 | N | % |
|---|
| N | % | N | % | N | % |
|---|
| General visibility | Very good | 28 | 93.3 | 30 | 100.0 | 27 | 90.0 | 85 | 94.4 | 2.96 | 0.227 |
| Good | 2 | 6.7 | | | 3 | 10.0 | 5 | 5.6 |
| Colour apprehension | Very good | 27 | 90.0 | 30 | 100.0 | 26 | 86.7 | 83 | 92.2 | 4.03 | 0.133 |
| Good | 3 | 10.0 | | | 4 | 13.3 | 7 | 7.8 |
| Observation of macroscopic features | Very good | 29 | 96.7 | 30 | 100.0 | 27 | 90.0 | 86 | 95.6 | 3.66 | 0.160 |
| Good | 1 | 3.3 | | | 3 | 10.0 | 4 | 4.4 |
| Appreciation or border or extent | Very good | 21 | 70.0 | 27 | 90.0 | 24 | 80.0 | 72 | 80.0 | 5.25 | 0.263 |
| Good | 5 | 16.7 | 2 | 6.7 | 5 | 16.7 | 12 | 13.3 |
| Average | 4 | 13.3 | 1 | 3.3 | 1 | 3.3 | 6 | 6.7 |
| Identification of normal tissue | Very good | 21 | 70.0 | 23 | 76.7 | 16 | 53.3 | 60 | 66.7 | 5.11 | 0.276 |
| Good | 7 | 23.3 | 6 | 20.0 | 13 | 43.3 | 26 | 28.9 |
| Average | 2 | 6.7 | 1 | 3.3 | 1 | 3.3 | 4 | 4.4 |
| Identification of abnormal tissue | Very good | 22 | 73.3 | 26 | 86.7 | 26 | 86.7 | 74 | 82.2 | 3.63 | 0.458 |
| Good | 7 | 23.3 | 4 | 13.3 | 4 | 13.3 | 15 | 16.7 |
| Average | 1 | 3.3 | | | | | 1 | 1.1 |
| Supplement in dissecting the area of suspicion | Very good | 28 | 93.3 | 16 | 53.3 | 27 | 90.0 | 71 | 78.9 | 27.25 | 0.001** |
| Good | | | 14 | 46.7 | 2 | 6.7 | 16 | 17.8 |
| Average | 2 | 6.7 | | | 1 | 3.3 | 3 | 3.3 |
| Orient the histology section in the specimen | Very good | 27 | 90.0 | 28 | 93.3 | 24 | 80.0 | 79 | 87.8 | 5.58 | 0.233 |
| Good | 1 | 3.3 | 2 | 6.7 | 5 | 16.7 | 8 | 8.9 |
| Average | 2 | 6.7 | | | 1 | 3.3 | 3 | 3.3 |
| Relate the histology features seen in sections with specimens | Very good | 24 | 80.0 | 13 | 43.3 | 10 | 33.3 | 47 | 52.2 | 20.64 | 0.001** |
| Good | 5 | 16.7 | 17 | 56.7 | 15 | 50.0 | 37 | 41.1 |
| Average | 1 | 3.3 | | | 5 | 16.7 | 6 | 6.7 |
| Facilitate in rendering diagnosis | Very good | 21 | 70.0 | 9 | 30.0 | 11 | 36.7 | 41 | 45.6 | 22.27 | 0.001** |
| Good | 7 | 23.3 | 21 | 70.0 | 12 | 40.0 | 40 | 44.4 |
| Average | 2 | 6.7 | | | 7 | 23.3 | 9 | 10.0 |
| Total | 30 | 100.0 | 30 | 100.0 | 30 | 100.0 | 90 | 100.0 | | |
*Significant at 5%; **Significant at 1% (Highly significant)
Macroscopic examination without stereozoom microscope (Chi-Square test).
| Observer | Total | Chi-square | p-value |
|---|
| OB 1 | OB 2 | OB 3 | N | % |
|---|
| N | % | N | % | N | % |
|---|
| General visibility | Good | 3 | 10.0 | 4 | 13.3 | 4 | 13.3 | 11 | 12.2 | 22.28 | 0.001** |
| Average | 4 | 13.3 | 18 | 60.0 | 16 | 53.3 | 38 | 42.2 |
| Poor | 21 | 70.0 | 5 | 16.7 | 8 | 26.7 | 34 | 37.8 |
| Very poor | 2 | 6.7 | 3 | 10.0 | 2 | 6.7 | 7 | 7.8 |
| Colour apprehension | Good | 3 | 10.0 | 3 | 10.0 | 2 | 6.7 | 8 | 8.9 | 6.39 | 0.381 |
| Average | 9 | 30.0 | 17 | 56.7 | 17 | 56.7 | 43 | 47.8 |
| Poor | 17 | 56.7 | 9 | 30.0 | 10 | 33.3 | 36 | 40.0 |
| Very poor | 1 | 3.3 | 1 | 3.3 | 1 | 3.3 | 3 | 3.3 |
| Observation of macroscopic features | Good | 3 | 10.0 | 1 | 3.3 | | | 4 | 4.4 | 20.02 | 0.003** |
| Average | 7 | 23.3 | 22 | 73.3 | 20 | 66.7 | 49 | 54.4 |
| Poor | 13 | 43.3 | 6 | 20.0 | 7 | 23.3 | 26 | 28.9 |
| Very poor | 7 | 23.3 | 1 | 3.3 | 3 | 10.0 | 11 | 12.2 |
| Appreciation or border or extent | Good | 3 | 10.0 | | | | | 3 | 3.3 | 25.84 | 0.001** |
| Average | 1 | 3.3 | 15 | 50.0 | 16 | 53.3 | 32 | 35.6 |
| Poor | 21 | 70.0 | 10 | 33.3 | 9 | 30.0 | 40 | 44.4 |
| Very poor | 5 | 16.7 | 5 | 16.7 | 5 | 16.7 | 15 | 16.7 |
| Identification of normal tissue | Average | 6 | 20.0 | 15 | 50.0 | 15 | 50.0 | 36 | 40.0 | 8.56 | 0.073 |
| Poor | 18 | 60.0 | 10 | 33.3 | 9 | 30.0 | 37 | 41.1 |
| Very poor | 6 | 20.0 | 5 | 16.7 | 6 | 20.0 | 17 | 18.9 |
| Identification of abnormal tissue | Average | 8 | 26.7 | 15 | 50.0 | 13 | 43.3 | 36 | 40.0 | 3.87 | 0.424 |
| Poor | 15 | 50.0 | 9 | 30.0 | 11 | 36.7 | 35 | 38.9 |
| Very poor | 7 | 23.3 | 6 | 20.0 | 6 | 20.0 | 19 | 21.1 |
| Supplement in dissecting the area of suspicion | Average | 9 | 30.0 | 15 | 50.0 | 11 | 36.7 | 35 | 38.9 | 2.83 | 0.586 |
| Poor | 17 | 56.7 | 13 | 43.3 | 16 | 53.3 | 46 | 51.1 |
| Very Poor | 4 | 13.3 | 2 | 6.7 | 3 | 10.0 | 9 | 10.0 |
| Orient the histology section in the specimen | Good | 3 | 10.0 | | | | | 3 | 3.3 | 12.51 | 0.052 |
| Average | 6 | 20.0 | 2 | 6.7 | 9 | 30.0 | 17 | 18.9 |
| Poor | 17 | 56.7 | 24 | 80.0 | 16 | 53.3 | 57 | 63.3 |
| Very Poor | 4 | 13.3 | 4 | 13.3 | 5 | 16.7 | 13 | 14.4 |
| Relate the histology features seen in sections with specimens | Good | 3 | 10.0 | | | | | 3 | 3.3 | 22.59 | 0.001** |
| Average | 6 | 20.0 | 2 | 6.7 | 1 | 3.3 | 9 | 10.0 |
| Poor | 8 | 26.7 | 18 | 60.0 | 7 | 23.3 | 33 | 36.7 |
| Very Poor | 13 | 43.3 | 10 | 33.3 | 22 | 73.3 | 45 | 50.0 |
| Facilitate in rendering diagnosis | Very Good | | | | | 3 | 10.0 | 3 | 3.3 | 23.96 | 0.002** |
| Good | 3 | 10.0 | | | | | 3 | 3.3 |
| Average | 7 | 23.3 | 3 | 10.0 | 1 | 3.3 | 11 | 12.2 |
| Poor | 15 | 50.0 | 21 | 70.0 | 13 | 43.3 | 49 | 54.4 |
| Very Poor | 5 | 16.7 | 6 | 20.0 | 13 | 43.3 | 24 | 26.7 |
| Total | 30 | 100.0 | 30 | 100.0 | 30 | 100.0 | 90 | 100.0 | | |
*Significant at 5%; **Significant at 1% (Highly significant)
Operation of stereozoom microscope (Chi-square test).
| Observer | Total | Chi-square | p-value |
|---|
| OB 1 | OB 2 | OB 3 | N | % |
|---|
| N | % | N | % | N | % |
|---|
| General easy to operate | Very good | 28 | 93.3 | 30 | 100.0 | 30 | 100.0 | 88 | 97.8 | 4.09 | 0.129 |
| Good | 2 | 6.7 | | | | | 2 | 2.2 |
| Easy to take photographs | Very good | 28 | 93.3 | 30 | 100.0 | 30 | 100.0 | 88 | 97.8 | 4.09 | 0.129 |
| Good | 2 | 6.7 | | | | | 2 | 2.2 |
| Ability to photograph details observed | Very good | 26 | 86.7 | 30 | 100.0 | 28 | 93.3 | 84 | 93.3 | 4.29 | 0.117 |
| Good | 4 | 13.3 | | | 2 | 6.7 | 6 | 6.7 |
| Easy to move specimens on stage | Very good | 7 | 23.3 | 2 | 6.7 | 18 | 60.0 | 27 | 30.0 | 37.85 | 0.001** |
| Good | 11 | 36.7 | 4 | 13.3 | 4 | 13.3 | 19 | 21.1 |
| Average | 6 | 20.0 | 3 | 10.0 | 3 | 10.0 | 12 | 13.3 |
| Poor | 5 | 16.7 | 16 | 53.3 | 5 | 16.7 | 26 | 28.9 |
| Very poor | 1 | 3.3 | 5 | 16.7 | | | 6 | 6.7 |
| Easy to zoom/magnify the specimens | Very good | 30 | 100.0 | 17 | 56.7 | 27 | 90.0 | 74 | 82.2 | 21.61 | 0.001** |
| Good | | | 11 | 36.7 | 3 | 10.0 | 14 | 15.6 |
| Very poor | | | 2 | 6.7 | | | 2 | 2.2 |
| Total | 30 | 100.0 | 30 | 100.0 | 30 | 100.0 | 90 | 100.0 | | |
*Significant at 5%; **Significant at 1% (Highly significant)
Preference of stereozoom microscope in gross examination (Chi-Square test).
| Observer | Total | Chi-square | p-value |
|---|
| OB 1 | OB 2 | OB 3 | N | % |
|---|
| N | % | N | % | N | % |
|---|
| General visibility | Very good | 30 | 100.0 | 29 | 96.7 | 30 | 100.0 | 89 | 98.9 | 2.02 | 0.364 |
| Good | | | 1 | 3.3 | | | 1 | 1.1 |
| Colour apprehension | Very good | 30 | 100.0 | 30 | 100.0 | 28 | 93.3 | 88 | 97.8 | 4.09 | 0.129 |
| Good | | | | | 2 | 6.7 | 2 | 2.2 |
| Observation of macroscopic features | Very good | 28 | 93.3 | 30 | 100.0 | 30 | 100.0 | 88 | 97.8 | 4.09 | 0.129 |
| Good | 2 | 6.7 | | | | | 2 | 2.2 |
| Appreciation or border or extent | Very good | 27 | 90.0 | 30 | 100.0 | 30 | 100.0 | 87 | 96.7 | 6.21 | 0.045* |
| Good | 3 | 10.0 | | | | | 3 | 3.3 |
| Identification of normal tissue | Very good | 26 | 86.7 | 29 | 96.7 | 28 | 93.3 | 83 | 92.2 | 2.17 | 0.338 |
| Good | 4 | 13.3 | 1 | 3.3 | 2 | 6.7 | 7 | 7.8 |
| Identification of abnormal tissue | Very good | 25 | 83.3 | 30 | 100.0 | 30 | 100.0 | 85 | 94.4 | 10.59 | 0.032* |
| Good | 3 | 10.0 | | | | | 3 | 3.3 |
| Average | 2 | 6.7 | | | | | 2 | 2.2 |
| Supplement in dissecting the area of suspicion | Very good | 28 | 93.3 | 18 | 60.0 | 30 | 100.0 | 76 | 84.4 | 31.26 | 0.001** |
| Good | | | 12 | 40.0 | | | 12 | 13.3 |
| Average | 2 | 6.7 | | | | | 2 | 2.2 |
| Based on the above features, would you use stereomicroscope for gross examination | Very good | 28 | 93.3 | 30 | 100.0 | 30 | 100.0 | 88 | 97.8 | 4.09 | 0.129 |
| Good | 2 | 6.7 | | | | | 2 | 2.2 |
| Total | 30 | 100.0 | 30 | 100.0 | 30 | 100.0 | 90 | 100.0 | | |
*Significant at 5%; **Significant at 1% (Highly significant)
Discussion
Gross examination of specimens provides diagnostically valuable information that facilitate the process of histologic diagnosis in pathology. This is routinely performed by recording the macroscopic features and photographing the specimen prior to tissue processing. This step is currently performed by postgraduate trainees or resident pathologists with the documentation done as an academic activity. The present study evaluates the stereozoom as an instrument to study as well to record the macroscopic features of biopsy specimens. The history and evolution of this microscope can enable pathologist to better understand the scope of this microscope and a detailed description of which is given in a recent review article published in 2019 by Simon-Stickley A [3].
A literature search conducted in the PubMed database showed 1300 articles published in the English language for studies done using stereomicroscope in the materials and methodology to analyse human tissue samples. This number was increased by 728 to a total of 2028 published articles for studies done also on other species and samples which include human teeth and dental instruments such as handpiece burs and endodontic instruments. Studies in Pathology showed stereomicroscope assisted dissection of tissue blocks, in the research of tissue culture samples, and studies on cornea and bone samples. In dental specialities, such as Endodontics and Prosthodontics, the microscope was used to analyse the surfaces of instruments, morphologies of roots and apices of single and multi-rooted teeth. This instrument has also been used in forensic dentistry as a tool in the identification process by macroscopic examination of teeth. Except for 21 studies, these studies have not mentioned whether a stereozoom or stereomicroscope was utilised in their study. The primary purpose cited in these articles showed that this microscope had been employed to obtain a magnified view of surfaces and to study the spatial anatomy of samples either for the objective of identification or comparison. There is a single article describing the utilisation of stereomicroscope in gross examination of five specimens and reaching a final diagnosis. However, there exist no studies reviewing this microscope in the gross examination or macroscopic study of biopsy specimens in comparison with the unaided eye.
This is the first study reporting an evaluation on the application of stereozoom microscope in gross examination of biopsy specimens. The study investigated the utility of the microscope in observing and recording the macroscopic features such as colour, appreciation of border and identification of normal and abnormal tissues features which are usually recorded by pathology trainees or residents prior to tissue processing for future reference and legal purposes. The present study showed that all observers were able to view the specimen (94.4%) and better differentiate the colour of the specimens (92.2%) and appreciate not only the macroscopic feature (95.6%) but also the border or extent (80%) of the specimen by utilising the stereozoom microscope and also scored a response of very good for all parameters such general visibility (98.9%), observation of macroscopic features (95.6%), appreciation or border or extent (96.7), identification of normal tissue (92.2%) and abnormal tissue (94.4%) to its preference of use in gross examination over the unaided eye (97.8%). The advantage provided by the microscope was the ability to magnify the surfaces of specimens which can prove difficult in case of the unaided eye wherein close observation can irritate the mucosal linings of the nasal cavity and the eye due to the vapours of the formalin fixatives in spite of taking protective measures.
The better recognition of macroscopic features enable proper dissections of specimens particularly incisional biopsy specimens of small dimensions which can prove difficult with the unaided eye [4,5]. Cysts and tumours of the oral cavity arise within the jaws and rarely manifests extraorally. The commonality between these lesions is that they arise from the odontogenic cells residing within the connective tissue component. Cysts and tumours are often difficult to diagnose with clinical examination alone and rely on radiographic and histologic features. Even specimen linings of cystic lesions require macroscopic examination to rule nodular growths which are suspicious areas suggestive of neoplastic proliferation. Also, the specimens of cystic linings frequently confirm a folded architecture due to lack of osmolality of the cystic fluid and the effect of tissue processing. In the present study, the observers were able to appreciate the architecture of the odontogenic cyst lining foldings, to explore the complete lining submitted and dissect the area of suspicion with the stereozoom microscope. Also, the observers were able to differentiate between the normal and abnormal tissue when compared with the conventional method and correlate the macroscopic with the microscopic features in the slide particularly in thin linings of odontogenic cysts.
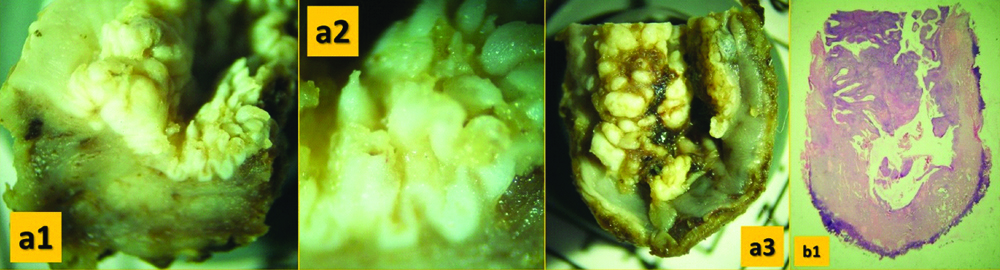
All three observers did find that the option of continuous zoom mechanism in stereozoom microscope for magnification to be better than the step up configuration of compound microscope. It was also found that all three observers favoured the use of the stereomicroscope in inspecting, taking photographs and recording the macroscopic features of the biopsy specimens. The observers were able to clearly visualise, observe, orient and record the macroscopic features of the specimens which are all the basic requirements of gross examination [6,7]. Efforts to view magnified images of biopsy specimens taken with the digital cameras can suffice but the clarity is lost when the magnified digital image is further zoomed in. Another alternative would be to zoom in or using option of optical zoom while taking the photograph of the specimen, but frequently the resultant image appears pixelated. While, the magnified images can be taken with ease without any loss of image clarity by attaching a digital camera by means of a mechanical adaptor to the stereomicroscope eyepiece or by using microscope eyepiece camera. Another advantage is that a video or multiple images can be preserved particularly for small specimens as the whole specimen would be embedded for tissue processing [8,9]. All three observers found the stereozoom microscope easy to operate as well to capture photographs of the specimen with a digital camera. With the option of transmitted light, the translucency of the specimen particularly in mucosal linings, the shadow of blood vessels could be appreciated showing the vascularity of tissues. Another use of transmitted light was that microscopic slides can be placed on the stage to appreciate the architecture or pattern of tissues such as the exophytic and endophytic growth, keratin plugging seen in histology slides of Verrucous Carcinoma [Table/Fig-7].
Biopsy specimen of Verrucous Carcinoma specimen under stereomicroscope in different aspects showing the exophytic and endophytic growth (a1, a2, a3). Histology section b1 of biopsy specimen shown in a3.
The study had also examined the operability of the microscope such as ability to zoom or magnify the specimens to enable dissection of the area of suspicion or interest, orientation of the specimens on the stage and the extent of transmitted and reflected illumination to capture photographs. All three observers found that the instrument was ease to operate with 97.8% scoring very good to good response. This is basically due to the simple design and mechanism for lens movement without the need of additional lens combination such as condensers seen in light microscopes. The strain on the eye is minimal and the stereo setup of the eyepiece or dual light pathway enable a three dimensional rendering of biopsy specimens providing the perception of depth and focus of different surface planes of irregular specimens.
Moreover, histological examination of specimens at times can be misleading, as the presence of the cells does not necessarily always substantiate the diagnosis. Proper evaluation of surrounding tissues can provide the reason for the source or origin of the cells in question. Macroscopic examination enable pathologist to orient the histology section to the specimen. The microscope that can record macroscopic features can help identify and recover specimen details which can serve as “clues” in case of specimen misidentification in the pre-analytic phase of specimen accession [10,11].
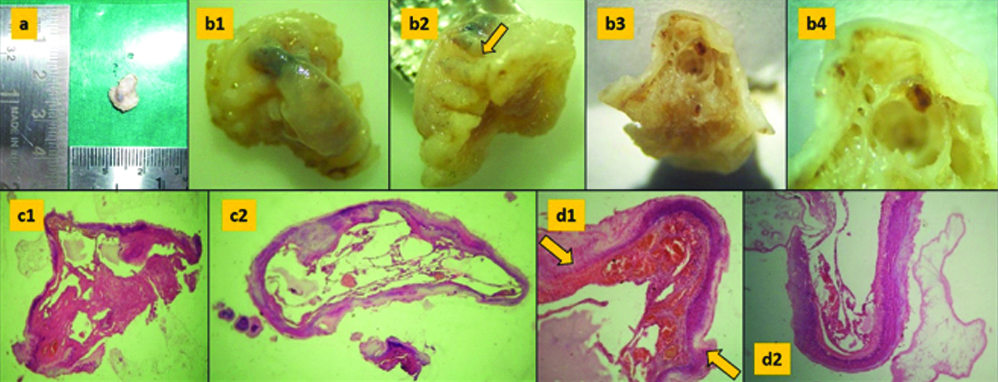
Artefacts due to the biopsy procedure or improper fixation are frequently encountered in microscopic sections and have always to be accounted. These can usually be neglected in the biopsy requisition forms or missed out at times which in turn may lead to delay in diagnosis [12]. Even specimen dimensional changes that distort the specimen caused as result of tissue processing can be better appreciated under the stereomicroscope. There is always a simple explanation to appearance of the tissue in microscopy which can be identified in the specimens. In biopsy specimen shown in [Table/Fig-8] illustrates the instrument markings on the specimen imprinted due to pressure exerted by the surgeon while performing the incisional biopsy in order to attain the a clean border. This creates an artefact or “squeeze artefact” which can be observed in the histological sections of d1 and d2 in [Table/Fig-8].
Biopsy specimen without the stereomicroscope (a); same specimen under stereomicroscope in different aspects (b1, b2, b3, b4). Imprints of tissue forceps (yellow arrow) visible in b2; Histology section c1, c2 of b3; Higher magnification d1, d2 of the same specimen showing the crush effect (yellow arrow).
The present study utilised the stereozoom microscope to examine soft tissue biopsy specimens from neoplastic to inflammatory lesions that presented in the oral cavity. To cite a few, the observers were able to differentiate certain tissues such as keratin in Verrucous Carcinoma, the loss of epithelium in linings of the fibroma, the adipose tissue surrounding the lymph nodes, and account for other tissues such the fibrous components in connective tissue tumours. These features were identified and well appreciated owing to the low power magnification provided by the microscope.
The clinical translation of Stereozoom microscope in gross examination is to disseminate information necessary for surgical pathologists and surgeons on the considerations to be taken when performing biopsies such as artefacts (mentioned above) and factors that oral pathologists require to interpret histologically particularly in small incisional biopsies where the specimens are either too small or misrepresented that the specimens carry little or no histologic features to render a diagnosis.
Limitation
The limitation of the present study was small sample size and not comparing the time taken for examination of specimens with and without the stereozoom microscope. For further study, a larger sample with excisional biopsy specimens can be considered to assess the utility of stereomicroscope in gross examination.
Conclusion
The primary purpose of this study was to evaluate the scope of stereozoom microscope as an aid in screening biopsy specimens in gross examination prior to tissue processing which is the preliminary step in the pre-analytic phase of tissue processing. The results of this study have shown that the stereozoom microscope can enable pathologists to not only examine specimens macroscopically but also orient and dissect areas of suspicion and prevent untoward loss of specimen tissue. Another aspect is that archiving is possible by recording the macroscopic features of specimens without the loss of clarity due to magnification. Also, this microscope enhances the knowledge of diagnostic pathology by correlating the macroscopic features with the histological features in a slide to better appreciate and understand the disease pathogenesis and bridge the gap of clinical and histological diagnosis. This evaluation study has shown that the stereozoom microscope does improve the existing practice of gross examination and macroscopic examination of biopsy specimens.
1: Very Good; 2: Good; 3: Average; 4: Poor; 5: Very Poor
*Significant at 5%; **Significant at 1% (Highly significant)
*Significant at 5%; **Significant at 1% (Highly significant)
*Significant at 5%; **Significant at 1% (Highly significant)
*Significant at 5%; **Significant at 1% (Highly significant)