Strangulated Small Intestinal Obstruction due to Giant Meckle’s Diverticulum: A Case Report
N Thulasivasudevaiah1, S Sudhir2, Deepak Naik3, DK Dilip4, Aparna Mallya5
1 Associate Professor, Department of Surgery, JSS Medical College and Hospital, JSSAHE and R, Mysuru, Karnataka, India.
2 Professor, Department of Surgery, JSS Medical College and Hospital, JSSAHE and R, Mysuru, Karnataka, India.
3 Assistant Professor, Department of Surgery, JSS Medical College and Hospital, JSSAHE and R, Mysuru, Karnataka, India.
4 Senior Resident, Department of Surgery, JSS Medical College and Hospital, JSSAHE and R, Mysuru, Karnataka, India.
5 Junior Resident, Department of Surgery, JSS Medical College and Hospital, JSSAHE and R, Mysuru, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. N Thulasivasudevaiah, JSS Medical College and Hospital, JSSAHE and R, Mysuru, Karnataka, India.
E-mail: thulasivasu2001@yahoo.com
Meckle’s Diverticulum (MD) is the most common congenital Gastro-Intestinal Tract (GIT) anomaly. Intestinal obstruction is the common presenting symptom in the adult population, due to complications like intussusception, incarceration, adhesion, stricture and torsion around a fibrous band. MD can present with similar symptoms of acute appendicitis or can present with painless lower GIT bleeding. Axial torsion of gangrenous MD can cause acute small bowel obstruction. The correct diagnosis of complicated MD before surgery is often difficult. This article is about a young boy who had signs and symptoms of acute small bowel obstruction for 15 days duration. He had MD which was adherent to umbilical region causing gangrenous small bowel obstruction. Initially, the patient was treated conservatively for suspected appendicitis in a peripheral Hospital at his native place and later he was referred for further management. He underwent surgery successfully and discharged after a week.
As the acute small bowel obstruction in paediatric patients can also have associated MD with initial presentation as acute appendicitis we should have a high index of suspicion while treating such cases. Early diagnosis and surgical intervention can avoid major bowel resection and overall morbidity.
Ectopic mucosa, Gastrointestinal bleeding, Intestinal strangulation, Meckle’s diverticulitis
Case Report
A young boy 17-year-old was brought to casualty with history of abdominal pain and vomiting since 20 days. He complained of abdominal distension since one day. He had a history of intermittent colicky abdominal pain around the umbilicus. He was treated for a week at primary health centre about 15 days ago, with a suspicion of acute appendicitis, with IV fluids and IV antibiotics. Due to persistent abdominal pain, an abdominal CT scan was done at his native place which showed multiple dilated small bowel loops with interloop fluid, and patient was referred to higher centre for further management.
On examination he was not anaemic, well hydrated with pulse-90/min, BP-100/70 mmHg. On abdominal examination- umbilicus was normal, generalised abdominal distension with more localised distension in the supra-pubic area which was not relieved even after catheterization. There was diffuse tenderness with guarding and tympanitic note on percussion over the distended area. Bowel sounds were absent. Hernial orifices were normal.
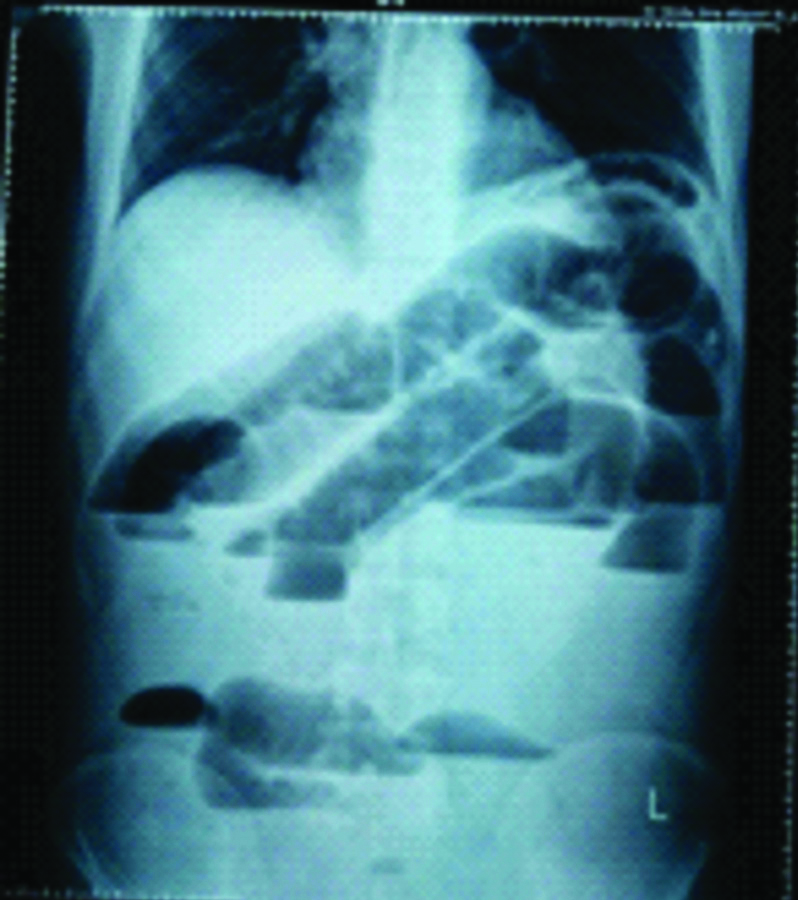
Blood investigations showed TC-11920 cells/cumm, N-90.2%, L-7.4%, E-0.3%, M-1.9%, B-0.2%, Blood urea-29 mg/dL, Creatinine-1.0 mg/dL. His abdominal plain X-ray showed multiple dilated small bowel loops across the abdomen [Table/Fig-1].
Plain abdominal radiograph- showing features of small bowel obstruction.
A provisional diagnosis of acute small intestinal obstruction due to volvulus was made and he was posted for emergency laparotomy. On opening the abdomen there was purulent fluid, partly haemorrhagic, which was aspirated. There was ischemic distended loop of terminal ileum in the pelvic region with thinned out wall and serosal tear. The Meckle’ diverticulum was big (about 10 cm long) with diameter more than 4 cm (distended) and the tip of which is attached to the umbilicus [Table/Fig-2]. A small segment of terminal ileum close to Ileo-caecal junction was viable. The loop of distended gangrenous ileum, nearly 70 cm including the ischemic MD, was resected [Table/Fig-3,4], and the distal viable end of ileum near the ileo-caecal junction was closed. The proximal cut end of the ileum was also closed in two layers and side to side ileo-transeverse anastomosis was performed. The caecum was healthy with normal retrocaecal appendix. Appendicectomy was also performed, followed by thorough peritoneal toilet. Abdominal wound was closed in layers with two flank drains.
Tip of the meckle’s diverticulum adherent to umbilicus.

Showing gangrenous ileum loop.

Resected specimen with long meckle’s diverticulum and appendix.

Postoperatively patient was managed with IV antibiotics, analgesics for one week. He was treated with TPN for 2 days. Patient was started on oral feeds on 5th day and he was discharged on 8th day. On follow-up visit, all the sutures were removed on 15th day and scar was healthy.
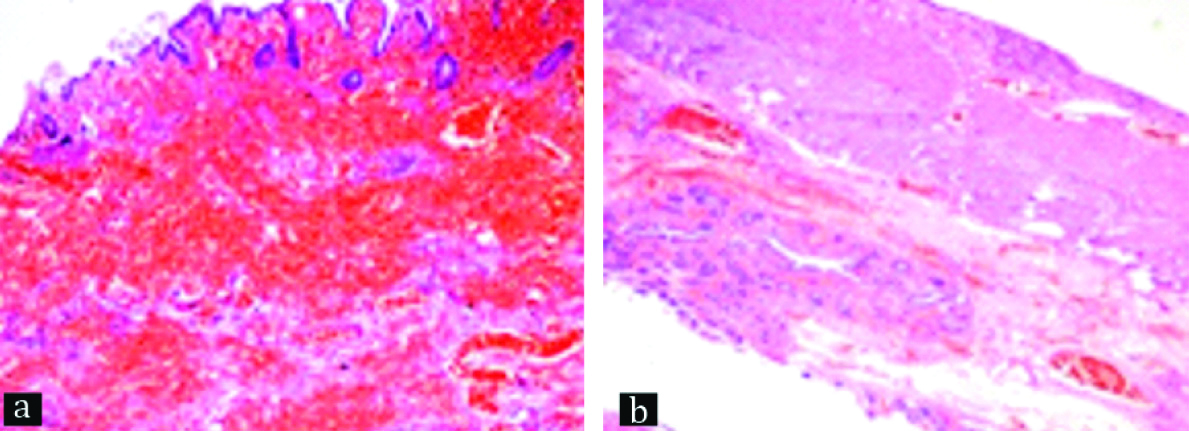
The histopathology of the specimen [Table/Fig-5a,b] showed Meckle’s diverticulitis with haemorrhagic infarction of the terminal ileum. Specimen of appendix showed reactive follicular hyperplasia.
Terminal ileum Meckel’s diverticulum; a) H&E stain, 40X; b) H&E stain, 10X.
Discussion
MD occurs in 2% of population. It is a true diverticulum possessing all the coats of the intestinal wall and has its own blood supply. It represents the embryological remnant of the proximal part of the vitello-intestinal duct which joined the faetal midgut and the yolksac. The length of this diverticulum ranges from 0.5 to 85 cm, but mean length is reported as 5 cm [1] and found 60 cm from the ileo-caecal junction.
The diverticulum is usually lined by normal small intestinal mucosa. The lumen of the diverticulum usually has a calibre similar to that of the ileum. The tip is normally free but occasionally it may be connected to the anterior abdominal wall near the umbilicus by a fibrous band. We have previously reported a case of asymptomatic MD which was bifid in nature [2]. The tip of the giant MD was adherent to the umbilicus [Table/Fig-1].
Patients with MD are usually asymptomatic. The rare complications of MD are severe haemorrhage, intussusception, diverticulitis, chronic peptic ulceration, intestinal obstruction, calculi and tumours. Meckel’s diverticulitis is uncommon in children older than 10 years. Adults with MD commonly present with small bowel obstruction caused by a fibrous band, torsion, intussusceptions and adhesions. MD can encircle the terminal ileum and cause acute small bowel obstruction [3,4]. Axial rotation and gangrene of MD is the rarest of the complication [5]. The correct diagnosis of complicated MD before surgery is often difficult due to similar clinical presentations in other acute abdominal surgical emergencies. Delay in diagnosis and surgery can lead to significant morbidity and mortality.
MD can present with acute small bowel obstruction in young adults due to fibrous band, adhesion or due to volvulus around fixed tip of MD [6]. Strangulated small bowel along with torsion of MD is described in another case report [7].
This kind of pathology is reported only 11 times, till 2014 [8]. Trapping of a bowel loop under the meso-diverticular band was the cause of small bowel obstruction in many cases [9]. Delay in the diagnosis and surgical treatment can result in significant morbidity and mortality as the patient can develop sepsis due to perforation of strangulated bowel. The index patient recovered well following resection of gangrenous bowel and ileo-transeverse anastomosis. The excised MD was nearly 10 cm with width of 4 cm near the base.
Conclusion
MD can cause acute small bowel obstruction by a band or volvulus. In a patient who presents with clinical features of acute appendicitis and if he develops distension of abdomen one should rule out possibility of complicated MD by a contrast CT abdomen or by laparotomy. As there was delay in referring the index case to higher centre, patient developed strangulated obstruction. The MD was adherent to umbilicus which was causing torsion of a loop of small bowel.
Financial or Other Competing Interests
None.
Patient permission was obtained for publication of this work.
[1]. Sengul I, Sengul D, Avcu S, Parlak O, Gangrenous meckle’s diverticulum in a strangulated umbilical herniaCases J 2010 10.1186/1757-1626-3-1020148138 [Google Scholar] [CrossRef] [PubMed]
[2]. Ravishankar N, Thulasi V, Uncomplicated bifid meckle’s diverticulum mimicking recurrent appendicitis. A case reportAnatomy Journal of Africa 2018 7(1):1094-96. [Google Scholar]
[3]. Wettasinghe M, Pussepitiya K, Samarasinghe B, Wickramasinghe N, Congenital vitilline band causing intestinal obstructionCase Rep Radiol 2016 2016:401540810.1155/2016/401540827843667 [Google Scholar] [CrossRef] [PubMed]
[4]. Thakor AS, Liau SS, O’Riodon DC, Acute small bowel obstruction as a result of a meckel’s diverticulum encircling the terminal ileum: A case reportJ Med Case Rep 2007 1:810.1186/1752-1947-1-817411459 [Google Scholar] [CrossRef] [PubMed]
[5]. Tenreiro N, Moreira H, Silva S, Madureira L, Gaspar J, Oliveira A, Unusual presentation of a meckle’s diverticulum: A case reportInternational J Surg Case Rep 2015 16:48-51.10.1016/j.ijscr.2015.09.01326413922 [Google Scholar] [CrossRef] [PubMed]
[6]. Sasilkumar K, Noonavath RN, Sreenath GS, Maroju NK, Axial torsion of gangrenous meckle’s diverticulum causing SBOJ Surg Tech Case Rep 2013 5(2):103-05.10.4103/2006-8808.12875224741431 [Google Scholar] [CrossRef] [PubMed]
[7]. Cartanese C, Petitti T, Marinelli E, Pignatelli A, Martignetti D, Zuccarino M, Intestinal obstruction caused by torsed gangrenous meckle’s diverticulum encircling terminal ileumWorld Journal of Gastrointestinal Surgery 2011 3(7):106-09.10.4240/wjgs.v3.i7.10621860699 [Google Scholar] [CrossRef] [PubMed]
[8]. Murruste M, Rajaste G, Torsion of meckle’s diverticulum as a cause of small bowel obstruction- A case reportWorld J of Gastrintsurg 2014 6(10):204-07.10.4240/wjgs.v6.i10.20425346803 [Google Scholar] [CrossRef] [PubMed]
[9]. Aljabri KA, El Shernin A, Small bowel obstruction due to meckle’s diverticulum- A case reportOman Medical Journal 2012 27(1):e029 [Google Scholar]