Medical education faces numerous challenges and when students enter medical college, they have a huge ocean of medical science in front of them. By the time they start learning Obstetrics and Gynaecology, they tend to forget the concerned anatomy, the peritoneal reflections. When they observe the patients undergoing per vaginal examination, they do not understand what and how the facts and findings are gathered and interpreted because the examining fingers and the organs being examined are inside and invisible to them. Similar difficulty is faced while observing IUCD insertion.
Different researchers have worked on this problem with variety of models. Saleem A et al., has created three dimensional visualisations using large scale HMM, made of readily available materials like transparent plastic sheets and sleeves, cardboard boxes, plastic bottles and balloons, and often even the students themselves to depict the anatomical structures [1]. Herur A et al., has utilised dough models for students to depict sensory and motor tracts [2]. Clay-models and hand-made silicon-bandage model have also been used [3,4]. The results were in favor of the models; concluding that learning with models was much beneficial.
Many readymade models and simulators are available for teaching the students, which are very expensive. They are not readily available at all institutes in developing countries and in settings with limited resources. As far as the author’s search could go, HMM for teaching Obstetrics and Gynaecology to undergraduates could not be found, which would make the learning easy and at no cost. If some such models are developed, this gap can be narrowed down. With the same motive, this study was planned and conducted by using HMM prepared on-the-spot, from on-the-spot available objects without spending a single penny; on medical undergraduates for teaching Obstetrics and Gynaecology and to see its efficacy.
Materials and Methods
An interventional study was carried out at Department of Obstetrics and Gynaecology, Chirayu Medical College and Hospital, Bhopal Madhya Pradesh, India over a duration of four months. Permission from Head of Department of Obstetrics and Gynaecology, Dean of the Institute and Research Committee was obtained. Informed consent from the study subjects was obtained, after they understood the nature of the study. There were no ethical issues involved in the project; hence ethical approval was not obtained from the ethical committee. The study subjects were 115 Final year MBBS students. The study was initially conducted on 30 students as a pilot study. Then extended study was done on other 85 students, out of which 11 students dropped out and thus final study was done on 104 students.
Few areas from the subject were further selected for the teaching purpose: Viz., 1) Anatomy of uterus, cervix, fallopian tubes, round ligament and ovary with ovarian ligament and broad ligament.
2) Method of per vaginal examination.
3) Method of IUCD insertion.
Students were selected by convenient sampling. They were divided into two groups. Both the groups were administered the same information (1,2,3) with two different teaching methods. For e.g.,
Group A: First 52 students were given demonstration of (1,2,3) by HMM prepared on-the-spot, with on-the-spot available objects (paper, pen, pencil, sharpener, polythene sheet).
Group B: Next group of 52 students were given the same information (1,2,3) by readymade videos.
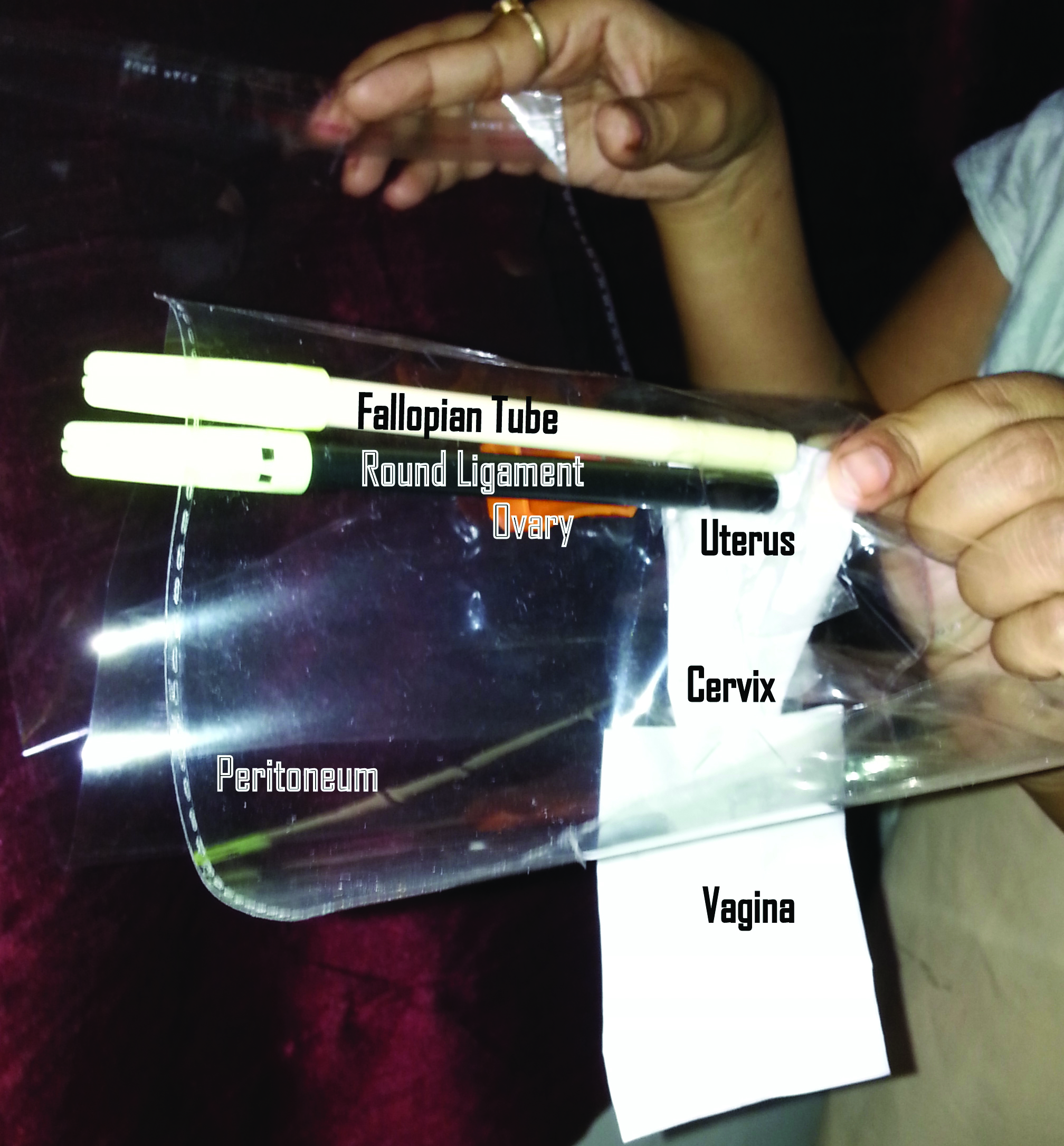
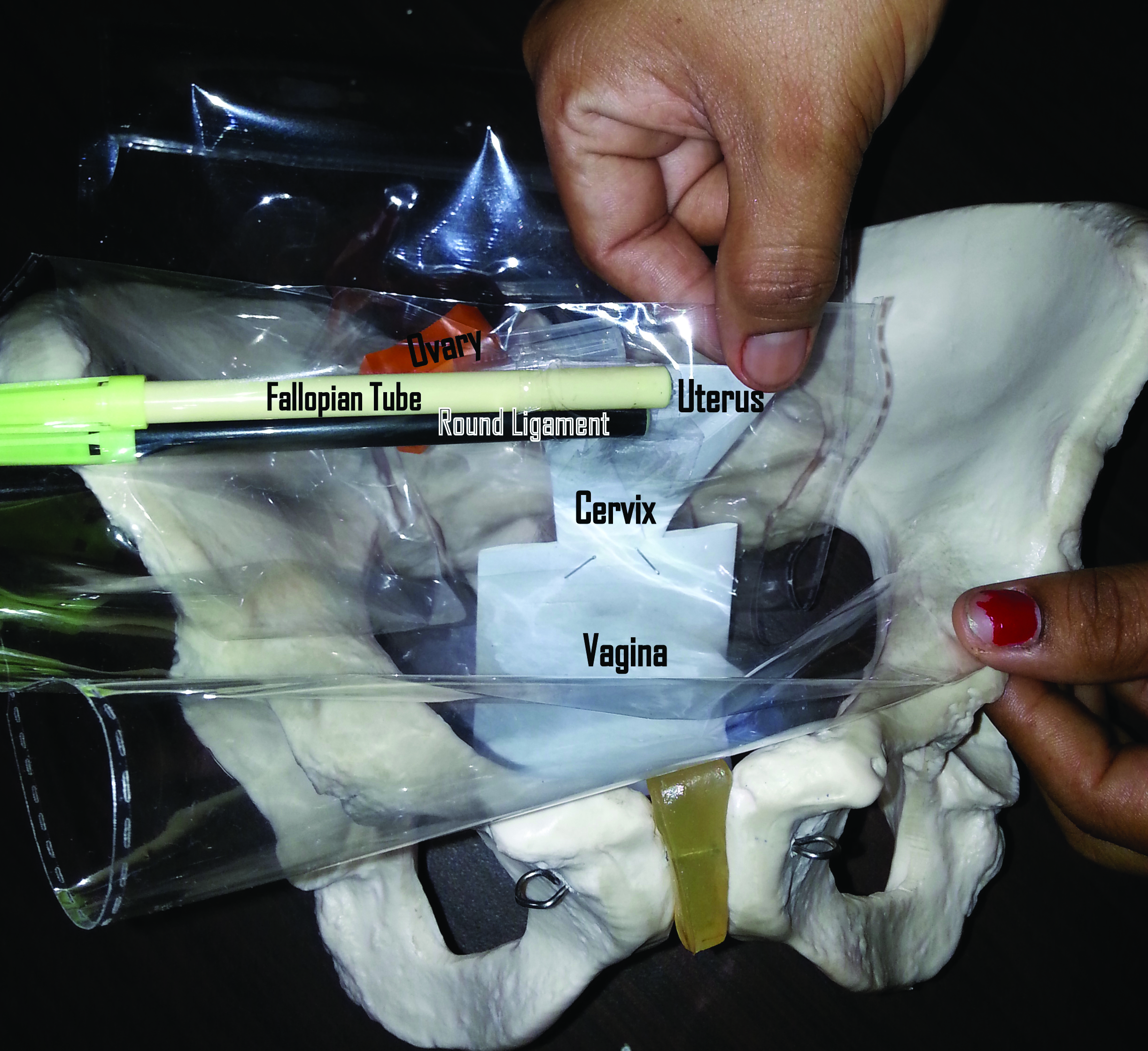
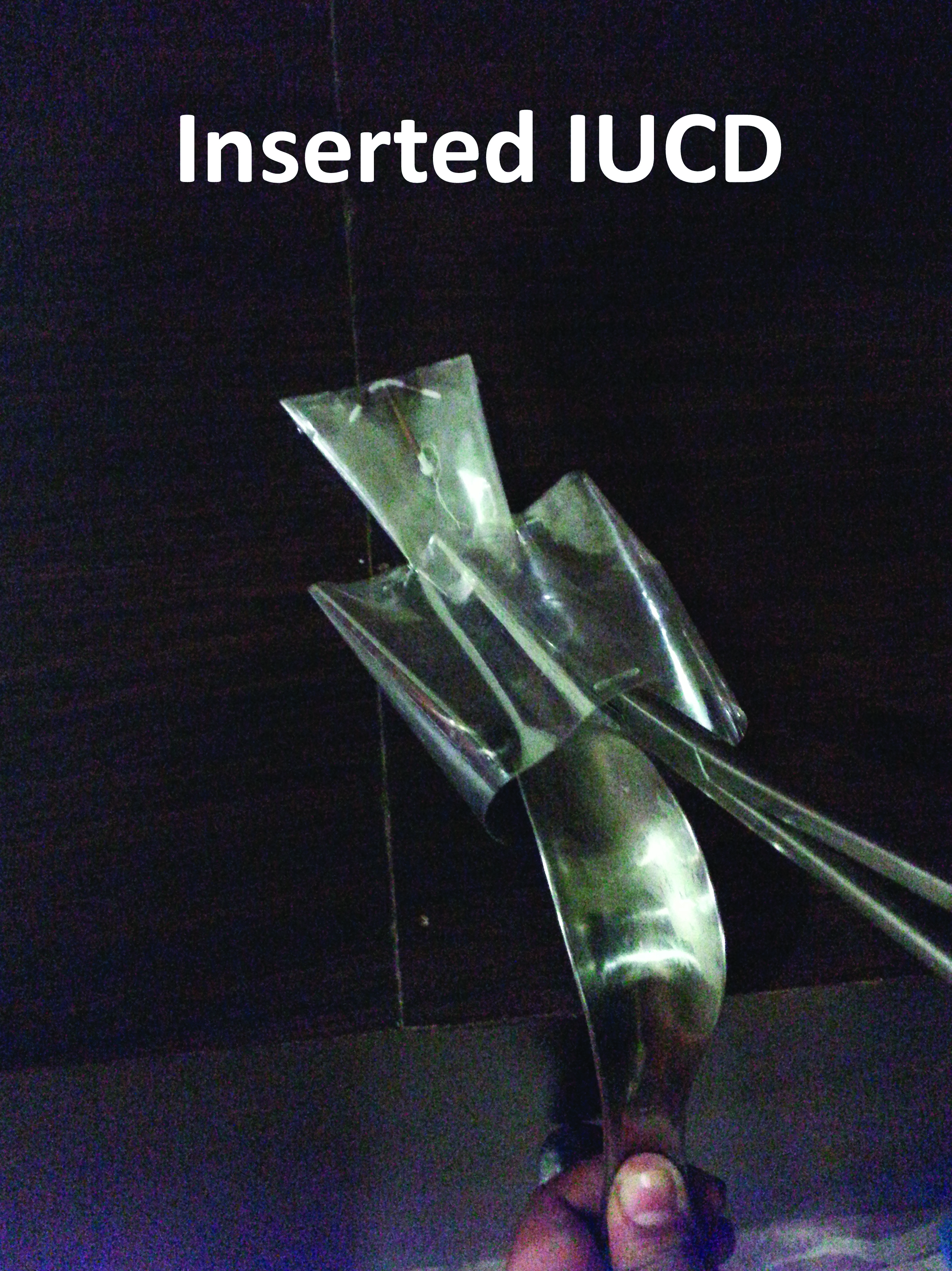
For making model of uterus, a paper was folded in the shape of uterus and cervix. This was further folded at the uterocervical junction to depict uterocervical angulation. Vagina was made with another paper [Table/Fig-1]. Pencil or pen was used to show fallopian tube and round ligament. They were held close to the cornu of uterus to show their anatomical attachment to uterus. A very small pencil was used to show ovarian ligament, at the lateral end of which a sharpener was attached to depict the ovary. Then a transparent polythene sheet was used to show the peritoneal reflection over and above these organs [Table/Fig-2]. This could also demonstrate well the mesosalpinx, meso-ovarium and mesentry of round ligament. This model was inserted into a bony pelvis [Table/Fig-3]. Students were involved in this activity to hold the uterine model in anatomical position there. After this, demonstration of per vaginal examination [Table/Fig-4] and IUCD insertion was performed on the model [Table/Fig-5]. For per vaginal examination, vagina was made with transparent sheet; for IUCD insertion, both uterus and vagina were prepared by transparent sheet so that both the procedures could be made visible.
Uterus, cervix and vagina.

Uterus, cervix, adnexa and peritoneum.
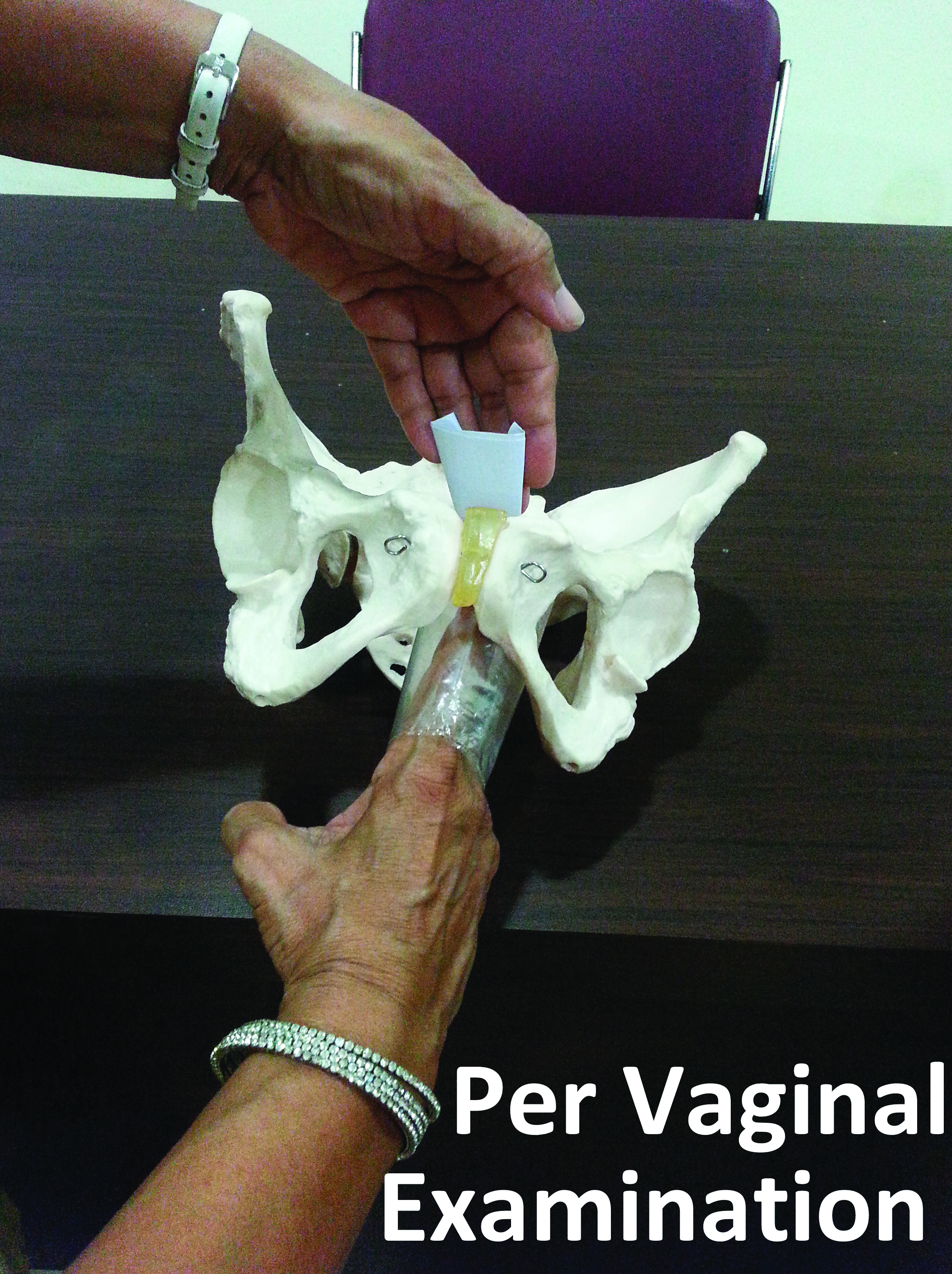
This activity could also be done if bony pelvis was not available.
The author herself conducted the teaching sessions by both the methods for the respective groups. The difference in the knowledge in each group was evaluated on the basis of OSCE. There were three OSCE stations, one for each activity. This was done with the help of a pre-structured check-list. The stations were:
Station-1: Demonstration of anatomy which carried 5 marks;
Station-2: Performing per vaginal examinations which carried 5 marks;
Station-3: Performing IUCD insertions which carried 10 marks.
Total maximum score: 20.
Time allotted for each activity: 3 minutes.
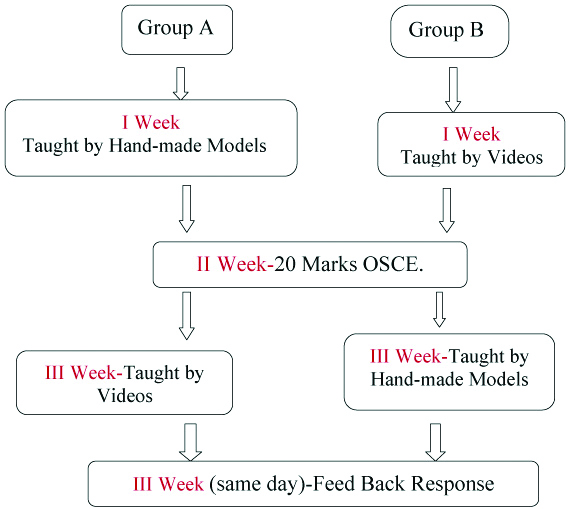
Names of the students and the group to which they belonged were blinded during OSCE. There were no practice sessions for them after they were taught. At the end of the study, the groups were crossed over for giving the same information as shown in [Table/Fig-6]. Lastly, students’ perception was noted on five-point Likert’s scale. Feedback was taken after the crossover so that they could experience both the methods and respond according to liking or disliking of the methods used.
Flowchart of methodology.
Statistical Analysis
The results such obtained were compared between both the groups. Statistical analysis was done by chi-square test, unpaired t-test of significance. The statistical software used was SPSS version 20.
Results
The mean OSCE scores for each activity are shown in [Table/Fig-7]. Combined mean scores for all three activities in group A and group B were 10.96±1.5 and 8.96±1.95 respectively. The difference being highly significant p<0.00001.
| Topics for teaching | Maximum score | Mean score obtained Group-A (HMM) | Mean score obtained Group-B (Video) | p-value, t-statistics |
|---|
| 1. Anatomy demonstration | 5 (100%) | 2.64 (52.8%) | 2.32 (46.4%) | p-value ≤0.00001Highly significant at p<0.05, t=5.04109 |
| 2. Per vaginal examination | 5 (100%) | 3.44 (68.8%) | 2.31 (46.2%) |
| 3. IUCD insertion | 10 (100%) | 4.61 (46.1%) | 4.33 (43.3%) |
| Mean of combined obtained score of activity 1,2,3 | | 10.96±1.5 | 8.96±1.95 |
| Total Maximum Score | 20 |
Discussion
Most of the teachers follow traditional, didactic and passive lecturing. This style of lecturing is usually less effective. If students are given the knowledge in such a manner which makes learning interesting and easy; they learn faster, the concept building is much easier. Concept building is the foundation of teaching-learning activity.
It is the duty of medical teachers to give them the knowledge in an interactive and interesting way. Students must not relate it to boredom. If the teaching activities are planned in this fashion, students’ attendance also improves. As per opinion of DiCarlo SE et al., teachers often focus more on the content rather than its influence. Students forget much of the content they memorise. Hence rather than worrying about covering the content, teachers should design such activities which focuses on the learning of students on how to use scientific knowledge to solve important questions and stimulate deep thinking [5].
Engaging lectures (broken or interactive) in which “breaks” with 1-min papers, problem sets, brainstorming sessions or open discussions were involved have been seen to show positive results [6]. Giuliodori MJ et al., have developed a model to demonstrate the underlying principles regarding Starling’s law of heart, lung and arterial elastic recoil. This enabled them to demonstrate the Hooke’s law [7].
Many simulators and readymade models are available for making learning easy, which are expensive. They are not readily available at all institutes in developing countries and in low resource settings. Saleem A et al., has created three dimensional visualisations using large scale HMM, made of readily available materials like transparent plastic sheets and sleeves, cardboard boxes, plastic bottles and balloons, to demonstrate the configuration of pleura, thoracic structures, peritoneum and abdominal/pelvic structures. He also made the use of students themselves to depict the anatomical structures [1]. Home-made limbs and kidneys have also been tried by him [1], to conclude that such activities promote interest, attention, learning and fun in class for both students and teachers.
Herur A et al., have studied the effect of active learning by dough models for students to depict sensory and motor tracts [2]. The results were analysed on the basis of questionnaire, concluding that the scores in the study group were greater when evaluated immediately after the class, after 15 and 30 days. In the study group, there was less deterioration in the scores.
HMM of sarcomere to illustrate the sliding filament mechanism in muscle contraction has been found to be efficacious [8]. Krontiris-Litowitz J et al., used modeling clay and beads as manipulatives and suggest that such activities can be used to enhance learning in neurophysiology curriculum [9].
HMM is an innovative method of the author, which she has used since many years as and when required during teaching. She observed that, in this method students participated with great curiosity and enthusiasm and they imbibed the concept quite easily. So, this was chosen as a subject for methodically studying the effect on their learning.
The results of study with HMM are consistent with above mentioned studies. The results suggests that this method is quite effective than the videos, difference in OSCE scores was statistically significant; p<0.00001, t=5.04109. [Table/Fig-8] also shows that HMM is a better method of teaching-learning than traditional, providing better understanding of concepts, helpful in changing learning attitude and behaviour while studying and can be introduced as a routine teaching-learning method for next batches, role of mentor is very important in teaching with HMM (94-97% response). Responses to open-ended questions [Table/Fig-9] tell that HMM is preferred method of choice, they are reproducible (87.49%) for own study. A total of 14.42% students responded that HMM is better for learning per vaginal examination and IUCD insertion while video is better for learning anatomy.
Feedback responses: Closed-ended questions.
| S. No. | Questions (Number of Participants=104) | Strongly agree (5%) | Agree (4%) | Neutral (3%) | Disagree (2%) | Strongly disagree (1%) |
|---|
| 1. | Hand-made models are helpful in better understanding of concepts. | 69 (66.34%) | 33 (31.73%) | 1 (0.96%) | 1(0.96%) | 0 |
| 2. | Teaching with hand-made models is a better method of teaching-learning than traditional lectures. | 75 (72.11%) | 26 (25%) | 3 (2.88%) | 0 | 0 |
| 3. | Teaching with hand-made models is a better method of teaching-learning than with videos. | 43 (41.34%) | 48 (46.15%) | 8 (7.69%) | 3 (2.88%) | 2 (1.92%) |
| 4. | Teaching with hand-made models is much helpful in understanding the anatomy. | 53 (50.96%) | 33 (31.73%) | 3 (2.88%) | 11 (10.57%) | 0 |
| 5. | Teaching with hand-made models is very helpful in learning clinical examination. | 62 (59.61%) | 33 (31.73%) | 3 (2.88%) | 5 (4.80%) | 1 (0.96%) |
| 6. | Teaching with hand-made models is very easy for understanding IUCD insertion. | 53 (50.96%) | 32 (30.76%) | 6 (5.76%) | 13 (12.5%) | 0 |
| 7. | Teaching with hand-made models has created interest and motivation in exploring other topics. | 61 (58.65%) | 36 (34.61%) | 6 (5.76%) | 1 (0.96%) | 0 |
| 8. | Role of mentor is very important in teaching with hand-made models. | 86 (82.69%) | 14 (13.46%) | 3 (2.88%) | 1 (0.96%) | 0 |
| 9. | Teaching with hand-made models is helpful in changing my learning attitude and behaviour while studying. | 62 (59.61%) | 40 (38.46%) | 1 (0.96%) | 1 (0.96%) | 0 |
| 10. | Teaching with hand-made models can be introduced as a routine teaching-learning method for next batches. | 67 (64.42%) | 32 (30.76%) | 5 (4.80%) | 0 | 0 |
| 11. | We can reproduce these models for our own learning at home and improve the learning process. | 50 (48.07%) | 41 (39.42%) | 6 (5.76%) | 4 (3.84%) | 3 (2.88%) |
| 12. | Teaching with hand-made models is a MUST in medical education from first MBBS. | 67 (64.42%) | 32 (30.76%) | 4 (3.84%) | 0 | 1 (0.96%) |
(Evaluated on the basis of five point Likert’s scale)
Feedback responses: open-ended questions.
| Questions | Answers-Number of students-(%) |
|---|
| Which is the preferred teaching-learning method of your choice? | Hand Made Models- 79 (75.96%) Video- 10 (9.61%) HMM+Video-15 (14.42%)
|
| Why do you say that a particular teaching-learning method is preferable? | HMM-Easy to understand-69 (66.34%) Facts are retained for long time-10 (9.61%)
Video-
Gives 3-D image, interesting-6 (5.76%) Concepts remain forever-2 (1.92%) Better understanding-2 (1.92%)
HMM+Video-15 (14.42%)
HMM is better for learning per vaginal examination and IUCD insertion Video is better for learning anatomy.
|
| Please mention the fact you liked the most in teaching by hand-made models. | Reproducible at home-91 (87.49%) Interactive-7 (6.73%) Linked with concepts hence easy to understand-6 (5.76%)
|
However, results of the study by DeHoff ME et al., are not consistent with the present study. Her results states that learning outcomes in human anatomy with clay models and cat dissection has concluded that both methods are equally effective [3].
Limitation
There were drop-outs due to the schedule spread over a long period. The OSCE and cross-over could be done at a gap of one week each. As this study was regarding demonstration, it was done on small group, hence sample size was limited.
Conclusion
Results of the study show that the scores in HMM group were higher than video group and the difference was statistically significant. The feedback also supports these results. Hence, the conclusion turns out that-teaching by HMM is an effective, simple and zero-cost method for teaching Obstetrics and Gynaecology to medical undergraduates.
(Evaluated on the basis of five point Likert’s scale)