An Unusual Presentation of Ochronosis with Palmar Pigmentation
Mohan Rao Nandam1, Shanthi Vissa2, Syam Sundara Rao Byna3, Bhavana Grandhi4, Sujitha Raguraman5
1 Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
2 Professor and Head, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
3 Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
4 Associate Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
5 Assistant Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Mohan Rao Nandam, Professor, Department of Pathology, Narayana Medical College, Nellore, Andhra Pradesh, India.
E-mail: nmr2020kmc@gmail.com
Ochronosis is the deposition of homogentisic acid in connective tissues resulting in bluish black discolouration. Hereby a case of ochronosis over the palmar surface of hand in 41-year-old male patient has been reported. Histopathological examination revealed yellowish brown colouration of collagen bundles in reticular dermis over palm of hand.
Alkaptonuria, Homogentisic acid, Methylene blue stain
Case Report
A 41-year-old male presented to dermatology outpatient department with stiffness of knee joints for 2 months, back pain since 6 months, bluish discolouration over palm for 1 year and passage of brown to black discolouration of urine for the last two years. No similar complaints noted in his family. Patient gave family history of consanguineous marriage. Patient’s haematological findings, liver function tests and kidney function tests were within normal limits. Urine turned to dark on exposure to air. Dermatological examination revealed bilaterally symmetrical palmar pigmentation.
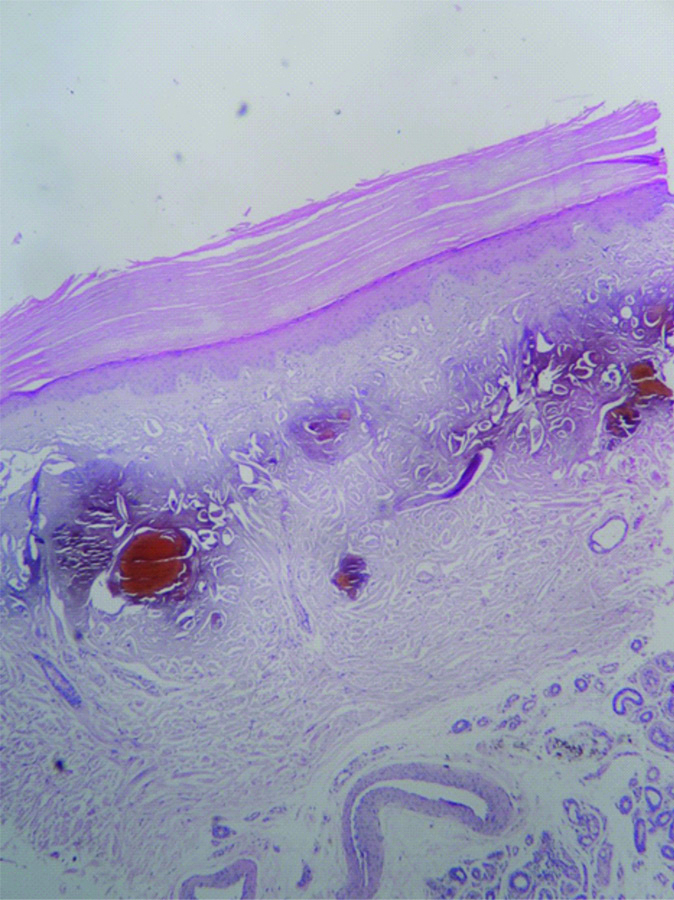
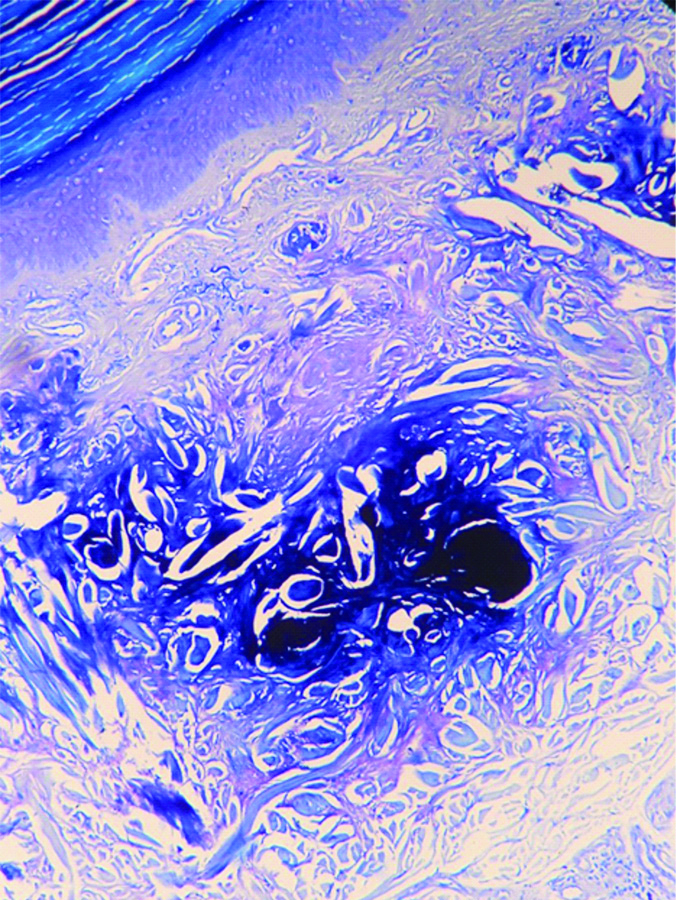
Clinically diagnosed as an acquired dermal melanocytosis of hands; plaque type of blue naevus. Skin punch biopsy sent to the Department of Pathology, tertiary care hospital for histopathological examination. Histopathological examination of skin biopsy reveal keratinized epidermal stratified squamous epithelium with underlying dermis showing skin adnexae and reticular dermis showing yellowish brown colouration of collagen bundles [Table/Fig-1]. Methylene blue staining of tissue sections showed from yellow brown colour to black colouration [Table/Fig-2]. Finally, it was diagnosed as ochronosis over the palm of the hand. The patient was treated symptomatically with Nonsteroidal Anti-Inflammatory Drugs (NSAIDs) and vitamin C. Patient is doing well after treatment.
Yellow brown ochronotic pigment deposition in collagen bundles of dermis (H&E, X100).
Blue black colouration of ochronotic pigment in collagen bundle of dermis (Methylene blue, X400).
Discussion
Ochronosis is a syndrome caused by deposition of homogentisic acid in connective tissues. In 1865, Rudolf Virchow first used the term ochronosis. It is one of the manifestations of alkaptonuria. Alkaptonuria is a rare inherited disorder characterised by deficiency of homogentisic acid oxidase enzyme [1]. Alkaptonuria consist of triad of manifestations, homogentisic aciduria, ochronosis and precocious degenerative arthropathy. Incidence of alkaptonuria is 1 in 250,000 live births to 1,000,000 liver births [2]. In present case, bilaterally symmetrical bluish palmar pigmentation was noted.
In 1584, Scribonius first used the term ochronosis in a boy with urine “as black as ink”. Bordekar in 1891 first coined the term alkaptonuria and was quoted by Fischer AA and Davis MW [3]. The term ochronosis was first coined by Virchow due to deposition of yellow pigment in connective tissue in reticular dermis [3]. Dark coloured urine is earliest manifestations of alkaptonuria. On voiding urine colour is normal and standing for several hours may turn into dark colour. In this case, the patient observed the passing of dark urine and bluish discolouration of palmar surface of both hands.
Degenerative arthropathy develops after the 3rd decade. In few studies, low backache was seen in 94% of patients before 40 years of age. The hip joint, knee joint and shoulder joints were frequently affected [1]. In this case, stiffness of knee joint is noted in 4th decade. Skin discolouration is noted after the 3rd decade [3]. In current case, discolouration of skin was noted in fourth decade of life.
Ochronosis is the one of the component of alkaptonuria. Alkaptonuria is a very rare metabolic disorder of phenylalanine catabolism. Alkaptonuria is an autosomal recessive inherited disorder. Alkaptonuria is caused by deficiency in homogentisic acid oxidase. This enzyme converts homogentisic acid to maleylacetoacetate in the tyrosine or phenylalanine catabolic pathway in the various organs like liver, small intestine, colon, kidney and prostate. Characteristic symptoms in the body are produced due to the accumulation of homogentisic acid and benzoquinone, which is the oxidised product of homogentisic acid. In 1958, La Du first identified homogentisic acid oxidase deficiency in ochronosis [4].
Ochronosis is mainly of two types. 1. Endogenous ochronosis (Alkaptonuria). 2. Exogenous ochronosis. Endogenous ochronosis is an autosomal recessive disorder in which homogentisic acid oxidase deficiency may leads to accumulation of homogentisic acid in palms and soles of the skin [5]. Exogenous ochronosis occur due to hydroquinone cream application on exposed parts of skin leading to blue-black pigmentation [6].
Most common differential diagnosis of ochronosis is Gout and pseudo-ochronosis. Histopathological examination of Gout reveals brown colour urate crystals deposition surrounded by granulomas with multinucleated giant cells. On Polarising light microscopic examination, urate crystals appear as refractile crystals. On staining tissue sections with 20% silver nitrate solution, urate crystals appears as black colour with surrounding yellow tissue [7]. Pseudo-ochronosis is defined as a deposition of silver into the collagen bundles due to trauma in jewelry workers. Histopathological examination of pseudo-ochronosis reveals yellow brown colouration of collagen bundles within the dermis [8]. In present case tissue sections show methylene blue positive material and urine also turned to dark colour on standing. Hence our case was reported as an endogenous ochronosis or alkaptonuria.
Nowadays there is no effective treatment for alkaptonuria and only symptomatic management is given. NSAID’s are commonly used in arthropathy.
Conclusion
Endogenous ochronosis is an uncommon condition which produces cosmetic disfigurement due to pigmentation that requires early diagnosis. Histopathological examination is gold standard for the diagnosis. Treatment is by symptomatic management.
Financial or Other Competing Interests
None.
Patient consent was obtained before publication of this work.
[1]. Phornphutkul C, Introne WJ, Perry MB, Hernardini I, Murphey MD, Firzpatrick DL, Natural history of alkaptonuriaN Engl J Med 2002 347(26):2111-21.10.1056/NEJMoa02173612501223 [Google Scholar] [CrossRef] [PubMed]
[2]. Tharini G, Ravindran V, Hema N, Prabhavathy D, Parveen B, AlkaptonuriaIndian J Dermatol 2011 56(2):194-96.10.4103/0019-5154.8041521716546 [Google Scholar] [CrossRef] [PubMed]
[3]. Fisher AA, Davis MW, Alkaptonuric ochronosis with aortic valve and joint replacements and femoral fractureClin Med Res 2004 2(4):209-15.10.3121/cmr.2.4.209 [Google Scholar] [CrossRef]
[4]. La Du BN, Zannoni VG, Laster L, Secgmiller JE, The nature of the defect in thyrosine metabolism in alkaptonuriaJ Biol Chem 1958 230(1):251-60. [Google Scholar]
[5]. Vijaykumar M, Thappa DM, Srilanth S, Alkaptonuria ochronosis presenting as Palmoplantar pigmentationClin Exp Dermatol 2000 25(4):305-07.10.1046/j.1365-2230.2000.00649.x10971492 [Google Scholar] [CrossRef] [PubMed]
[6]. Snider RL, Thiers BT, Exogenous ochronosisJ Am Acad Dermatol 1993 28(4):662-64.10.1016/S0190-9622(08)81794-X [Google Scholar] [CrossRef]
[7]. Cohen RR, Schmidt WA, Rapini RP, Chronic tophaceous gout with severely deforming arthritis; a case report with emphasis on histopathologic considerationCutis 1991 48(6):445-51. [Google Scholar]
[8]. Robinson-bostom L, Pomerantz D, Wilkel C, Localized argyria with pseudo-ochronosisJ Am Acad Dermatol 2002 46(2):222-27.10.1067/mjd.2002.11622711807434 [Google Scholar] [CrossRef] [PubMed]