Ipsilateral Femoral Neck and Shaft Femur Fracture in a Child: Nonoperative Management
Manoj Aggarwal1, Kunal Kishore2, Chirag Arora3, Sanjay Pandey4, Vishal Kumar5
1 Consultant, Department of Orthopaedics, Gaurav Fracture Clinic, Patna, Bihar, India.
2 Assistant Professor, Department of General Surgery, Narayan Medical College, Jamuhar, Bihar, India.
3 Senior Resident, Department of Orthopaedics, PGIMER, Chandigarh, India.
4 Associate Professor, Department of PMR, AIIMS, Patna, Bihar, India.
5 Assistant Professor, Department of Orthopaedics, PGIMER, Chandigarh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Chirag Arora, #C2/74; Ashok Vihar Phase II, Opp. Deep Market, New Delhi-110052, India.
E-mail: aro.chirag@gmail.com
Concomitant ipsilateral fractures of the neck and shaft of femur are a rare occurrence in childhood. Only 14 cases have been reported to date, the most common fracture pattern being Delbet Type III and a spiral fracture of midshaft femur. A four-year-old boy presented with closed fracture shaft femur and chest trauma (2-8th rib fractures right side with underlying haemopneumothorax), fracture neck femur was incidentally detected on pelvic radiographs. Initially, he was managed according to ATLS protocols, surgical management of lower limb was deferred till vitals stabilised. Later child was managed nonoperatively in view of persistent poor chest condition with one and half hip spica cast. Successful clinic-radiological union was noted at 24 months. We should have a high index of suspicion for proximal femur fractures especially in a child with multiple organ injuries.
Coxa vara, Neck femur, Paediatric trauma, Polytrauma
Case Report
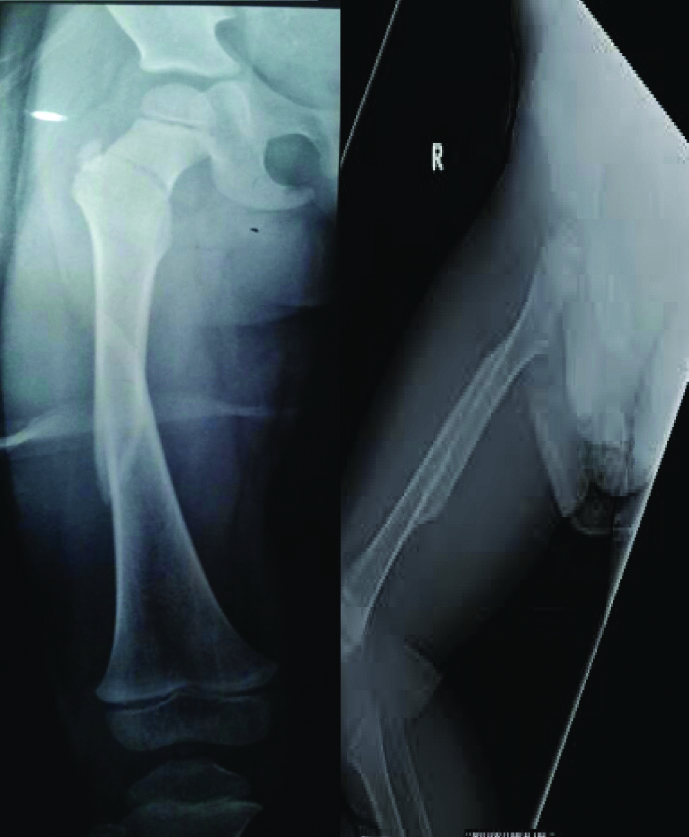
A four-year-old boy was brought to the trauma centre following a roadside accident (2 hours following trauma). At the time of examination, the child was in shock with thready pulse, difficulty in breathing and hypotension. Blood Pressure (BP) was 80/40 mmHg, Heart rate 140 per minute, Arterial Blood Gas analysis revealed lactic acidosis and base deficit. Clinical examination revealed chest compression test positive and chest tenderness was noted on right side. The child was managed according to ATLS protocol with intubation, rapid infusion of IV fluids, sodium bicarbonate, whole blood and urine output monitoring. After the primary survey, a thorough secondary survey was done and deformity of right thigh was noted. Chest and pelvic radiographs were done after stabilisation of vitals. Radiographs revealed a displaced fracture shaft of femur, multiple rib fractures right side 2-8th with underlying haemopneumothorax. Undisplaced fracture neck femur (cervicotrochanteric type) was noted as an incidental finding [Table/Fig-1]. The child was managed with insertion of Intercostal drainage tube (ICD) and skin traction. Orthopaedic surgical management was deferred until the child was stabilised for operative treatment. After 10 days, the child was still on ventilator, therefore, he was planned for closed reduction with one and half hip spica cast and tracheostomy in view of anticipated prolonged intubation. He was weaned-off the ventilator on 21st day. Confirmatory X-rays were done at that time which shows adequate reduction. The child was discharged on 23rd day. At each follow-up visit, clinical and radiological examinations were done. At 2 month follow-up, hip spica was removed, clinical examination revealed a varus deformity and 2 cm shortening of affected limb, and however, the child was able to walk comfortably with no pain. Anteroposterior (AP) and Lateral X-rays [Table/Fig-2] were showing callus formation. At the final 2 years follow-up, clinical examination reported no limb length discrepancy [Table/Fig-3,4] with pain free return of activities and no deformity or no restriction of range of motion at hip and knee joint.
Radiograph showing ipsilateral fracture neck and shaft of femur.
Showing 2 months follow-up of ipsilateral neck and shaft femur fracture. (first two images from left side);
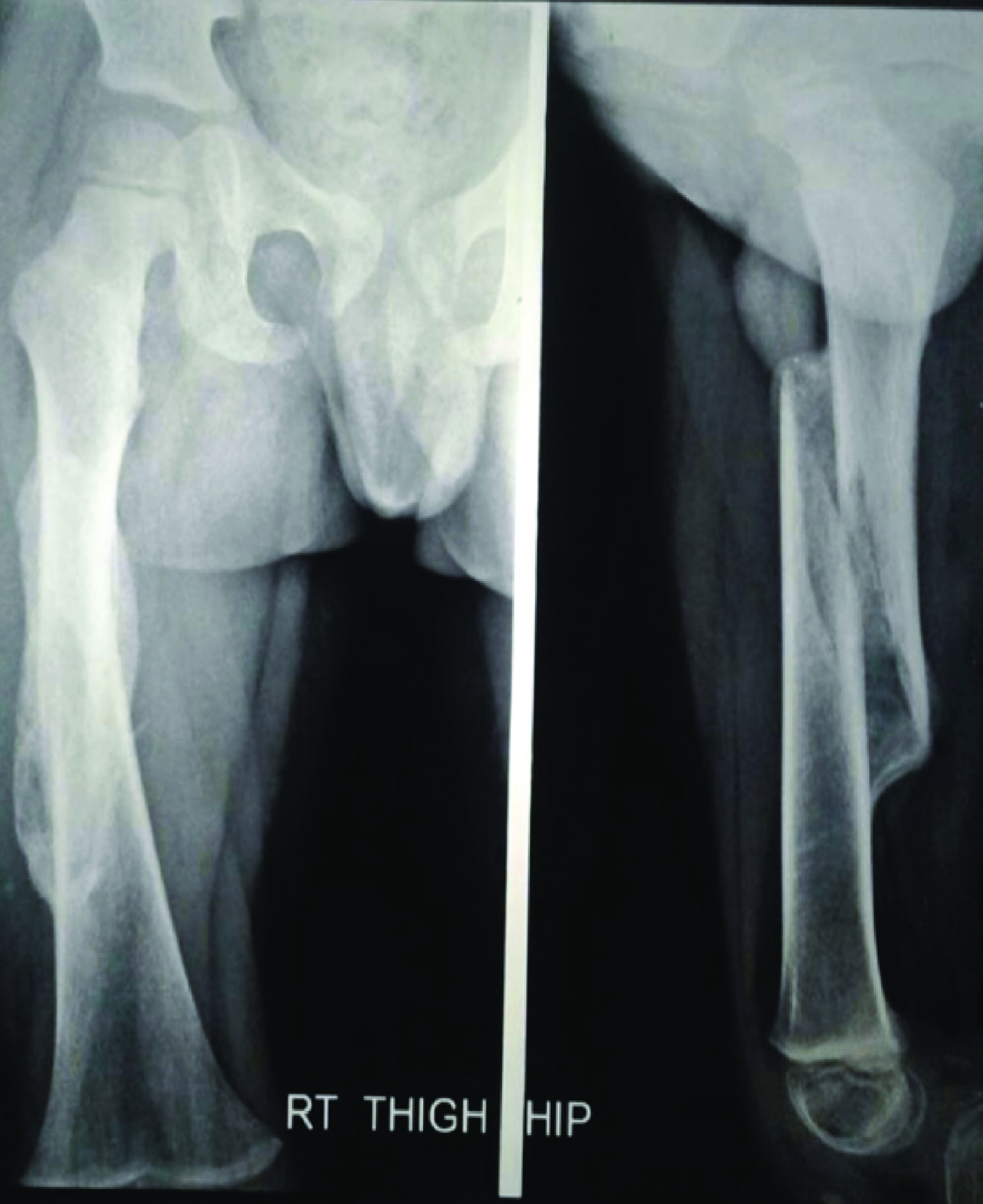
Two-year follow-up radiograph of the same patient. (first image from right side)

Clinical photograph showing no limb length discrepancy (24 months follow-up).

Discussion
Concomitant ipsilateral fractures of the neck and shaft of femur are a rare occurrence in childhood, carrying significant morbidity to the patient [1,2]. Only one or two cases are reported in each of the works mentioned in the literature [3,4]. These injuries occur in children due to high-velocity trauma typically seen in road traffic accidents, and commonly there are associated injuries to other organ systems. Early anatomical reduction and internal fixation is the treatment of choice in femoral neck fractures in children and adolescents [5-7]. Open/closed reduction internal fixation with a plate or flexible nails are recommended for shaft fracture. These injuries are associated with high incidence of AVN, shortening, limb length discrepancy and coxa vara [8,9]. The incidence of these complications are proportional to degree of initial displacement, the type of neck fracture and the timing of surgery [2-7]. Routine use of CT scan to detect neck fracture is not recommended in view of very low incidence (0.7%) of this combination of injuries and the damaging effects of radiation on physis [10].
Hoekstra HJ and Binnendijk B, estimated an approximate ratio of 1:4 for hip fracture in children/adolescents (age group 0-16 years) with those of adults [11]. The most common fracture pattern in these injuries is Delbet Type III and a spiral fracture of midshaft femur [1]. The physician should have a high index of suspicion for this combination of injury as these are associated with difficulty in management and complication [11,12]. Most common mechanism of trauma is simultaneous application of torsional and bending forces at both the fracture sites simultaneously. A medial comminution in the neck region is common in such cases leading to initial coxa vara [13] which resolves subsequently over time. Agarwal A et al., suggested a “symbiotic relationship” for this combination of ipsilateral femoral neck and shaft fracture in children, as a fracture at two sites resulted in dissipation of energy, therefore preventing extreme damage to either of the fracture sites and relatively lower complications [1].
Multiple treatment options are available for treatment of these injuries including nonoperative and operative modalities or a combination [3,4,9]. Nonoperative treatment includes reduction and hip spica immobilisation. Frequent check radiographs should be done to check for displacement of fracture sites. Operative treatment was performed using cannulated screws or paediatric hip compression screw (cervicotrochanteric fracture). Available options for shaft fracture treatment include plates or flexible nails (titanium or stainless steel). Good results have been described with either treatment, however operative stabilisation of both fracture sites is preferred as it allows early mobilisation and reduces chances of displacement and further complications [12-14]. It is recommended to fix the shaft fracture first so as to allow traction, closed reduction and manipulation for neck femur reduction [4,5]. Childhood femoral neck fractures are associated with a number of complications including AVN, coxa vara, early physeal closure, chondrolysis and limb length discrepancy [3-8]. The degree of displacement of fracture is proportional to intensity of trauma leading to higher incidence of complications. The child should be under a close and regular follow-up until skeletal maturity.
Conclusion
These uncommon injuries are associated with poor outcomes and a higher incidence of complications due to higher initial trauma, peculiar vascular anatomy of femoral neck and presence of open physis. Therefore, a close long-term follows-up till skeletal maturity should be maintained. Early detection and treatment of complications are of paramount importance.
Financial or Other Competing Interests
None.
Patient consent was obtained before publication of this work.
[1]. Agarwal A, Agarwal R, Meena DS, ipsilateral femoral neck and shaft fracture in childrenJ Trauma 2008 64(4):E47-53.10.1097/01.ta.0000196696.87716.8c18404044 [Google Scholar] [CrossRef] [PubMed]
[2]. Fardon DF, Fracture of neck and shaft of the same femur. Report of a case in a childJ Bone J Surg Am 1970 52:797-99.10.2106/00004623-197052040-00010 [Google Scholar] [CrossRef]
[3]. McDougall A, Fracture of the neck of femur in childhoodJ Bone Jt Surg Am 1967 49:16-29. [Google Scholar]
[4]. Swiontkowski MF, Hansen ST, Kellam J, Ipsilateral fracture of the femoral neck and shaft. A treatment protocolJ Bone Jt Surg Am 1984 66:260-68.10.2106/00004623-198466020-00013 [Google Scholar] [CrossRef]
[5]. Akahane T, Fujioka F, Shiozawa R, A transepiphyseal fracture of the proximal femur combined with a fracture of the mid-shaft of ipsilateral femur in a child: a case report and liter-ature reviewArch Orthop Trauma Surg 2006 126(5):330-34.10.1007/s00402-005-0028-y16612620 [Google Scholar] [CrossRef] [PubMed]
[6]. Bali K, Sudesh P, Patel S, Kumar V, Saini U, Dhillon MS, Pediatric femoral neck fractures: our 10 years of experienceClin Orthop Surg 2011 3(4):302-08.10.4055/cios.2011.3.4.30222162793 [Google Scholar] [CrossRef] [PubMed]
[7]. Boardman MJ, Herman MJ, Buck B, Pizzutillo PD, Hip fractures in childrenJ Am Acad Orthop Surg 2009 17:162-73.10.5435/00124635-200903000-00005 [Google Scholar] [CrossRef]
[8]. Ratliff AH, Fractures of the neck of the femur in childrenJ Bone Jt Surg Br 1962 44:528-42.10.1302/0301-620X.44B3.528 [Google Scholar] [CrossRef]
[9]. Canale ST, Fractures of the hip in children and adoles-centsOrthop Clin North Am 1990 21:341-52. [Google Scholar]
[10]. Morrissy RT, Hip fractures in childrenClin Orthop Relat Res 1980 152:202-10.10.1097/00003086-198010000-00023 [Google Scholar] [CrossRef]
[11]. Hoekstra HJ, Binnendijk B, Fractures of neck and shaft of same femur in children. A report of two casesArch Orthop Trauma Surg 1982 100:197-98.10.1007/BF00442734 [Google Scholar] [CrossRef]
[12]. Moon ES, Mehlman CT, Risk factors for avascular necrosis after femoral neck fractures in children: 25 Cincinnati cases and Meta-analysis of 360 casesJ Orthop Trauma 2006 20:323-29.10.1097/00005131-200605000-0000516766935 [Google Scholar] [CrossRef] [PubMed]
[13]. Huges LO, Beaty JH, Current concept review. Fractures of the head and neck of the femur in childrenJ Bone Joint Surg 1994 76A:283-92.10.2106/00004623-199402000-000198113267 [Google Scholar] [CrossRef] [PubMed]
[14]. Bennett FS, Zinar DM, Kilgus DJ, Ipsilateral hip and femoral shaft fracturesClin Orthop 1993 296:168-77.10.1097/00003086-199311000-00030 [Google Scholar] [CrossRef]