The diagnosis and accuracy in determining the exact location, extent and configuration of bony defects and classification of furcation defects are important aspects of periodontal examination, both for treatment planning and prognosis of teeth [1].
Currently the main diagnostic tools for periodontal diseases are clinical probing and intraoral radiography. However, both techniques have its own limitation in assessment of periodontal bone loss. The major limitation is that the three dimensional information of periodontal bone defects, especially intra bony defects and furcation involvements cannot be obtained [1]. Projection errors associated with 2 dimensional radiographs may over-estimate or under-estimate bone loss and also is hindered by the overlapping of anatomical structures [2,3]. Probing force is proportional with the values obtained during clinical probing [2].
Lack of three dimensional information of the dentition was overcome by the introduction of CT scan, however the increased radiation exposure and high cost was its main disadvantage [4]. Therefore, in order to understand the bone dimensions and to evaluate the bone gain after treatment, direct surgical or open bone measurements was considered to be the gold standard [5]. However, it gives only little time for the surgeon to evaluate the type and depth of the defect during surgery and plan for periodontal regeneration procedures. To overcome this Cone beam CT (CBCT) has been introduced and have wide range of applications in the field of dentistry [6].
Cone beam computed tomography provides three-dimensional information of the dentition as well as its supporting structures. Other benefit includes reduced radiation exposure to the patient compared to conventional CT, panoramic radiography and full mouth IOPA. Scan time is rapid in CBCT compared to panoramic radiograph, accurate image with resolution ranging from 0.4 mm to 0.076 mm can be obtained in CBCT, and also CBCT allows multiplanar reformation of the image [5].
CBCT is being widely used in dentistry since a decade. However most of its use is limited to assist or helps in implant placement, in the field of orthodontics, oral surgery and evaluate soft tissue lesions [7]. In the field of periodontology, although quite a few studies are done on dry skulls, cadavers and patients, CBCT studies evaluating horizontal and vertical bone loss, furcation involvement further need to be justified by the fact that most of the clinicians in India still rely on two dimensional radiography for periodontal and implant assessment [8]. Long term studies are scarce, this become important especially when proper research protocols are followed and provide an opportunity to regularly follow-up the study participants to understand the effectiveness of the treatment [9].
Therefore, the aim of this study was to compare linear measurements of periodontal defects using CBCT to traditional methods and direct surgical measurements with the following objectives- to determine the association between clinical probing measurements and direct bone measurements of periodontal defects during surgical procedure, to determine the association between cone beam computed tomography measurements and direct bone measurements of periodontal defects during surgical procedure, to determine the association between intraoral periapical radiographic measurements and direct bone measurements of periodontal defects during surgical procedure, to assess the reliability of clinical probing measurements, CBCT measurements, IOPA measurements with direct bone measurements of periodontal defects obtained during surgery.
Materials and Methods
This study was conducted from July 2014 to July 2017 (3 years) in the Department of Periodontology in association with the Department of Oral Medicine and Radiology, Yenepoya Dental College, Yenepoya University, Mangaluru. A cross-sectional study was conducted on 63 sites in both male and female subjects who attended the OPD of Yenepoya Dental College, Yenepoya University, Mangaluru such that the power of the study was set-up at 95 percentage confidence interval. Since the prevalence of periodontal diseases are more in population ranging from 15-64 years of age, subjects from these age groups were included in the study. The Institutional Ethical Clearance was obtained before the study (YUEC241/6/12/2014).
Participation was voluntary, and all the participants were asked to sign written consent after informing the objective of the study. The study sample included 63 sites in the dentate patients with periodontitis. Random selection of patients was done by the coin-toss method. A brief case history was recorded initially. The selected patients (inclusion criteria) were those having presence of periodontal pockets of >5 mm, molars with furcation involvement and advanced periodontal disease requiring surgical intervention. Patients with uncontrolled systemic diseases, smokers, pregnant or lactating women and mandibular or maxillary third molars were excluded from the study.
The patients were clinically examined and screened for periodontal defects. All the patients were observed under adequate natural light, mouth mirror, and University of North Carolina 15 periodontal probe in dental chair. All the measurements were done by single examiner. The examiner underwent training for performing the measurements. The examiner was unaware of the name of the patient or the clinical measurements made during surgery.
Clinical Probing Measurements
Clinical probing measurements were obtained from six areas around the tooth with a UNC-15 probe. Mid-buccal, Mid-lingual (Mid-palatal), Mesio-buccal, Disto-buccal, Mesio-lingual (Mesio-palatal), Disto-lingual (Disto-palatal).
For furcation involvement, clinical measurements were taken with Nabers probe to assess the grade of furcation involvement.
On the scheduled day of periodontal flap surgery prior to anesthesia a high definition CBCT and IOPA of the quadrant to be operated was taken.
Cone Beam Computed Tomography
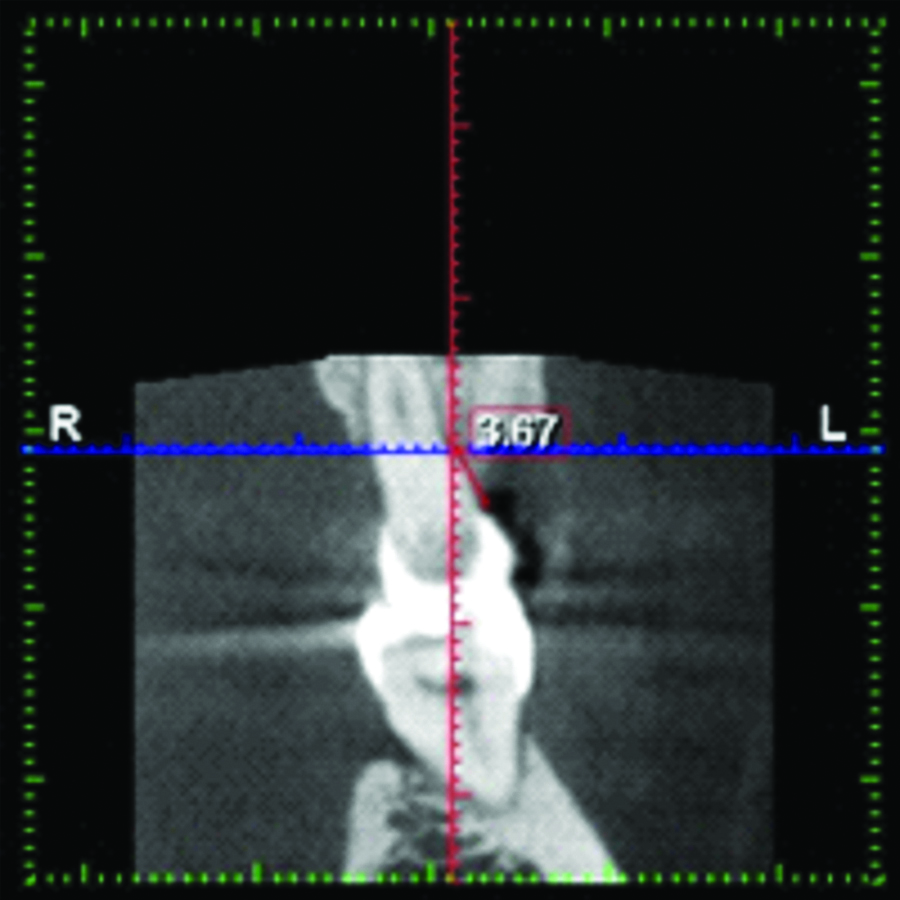
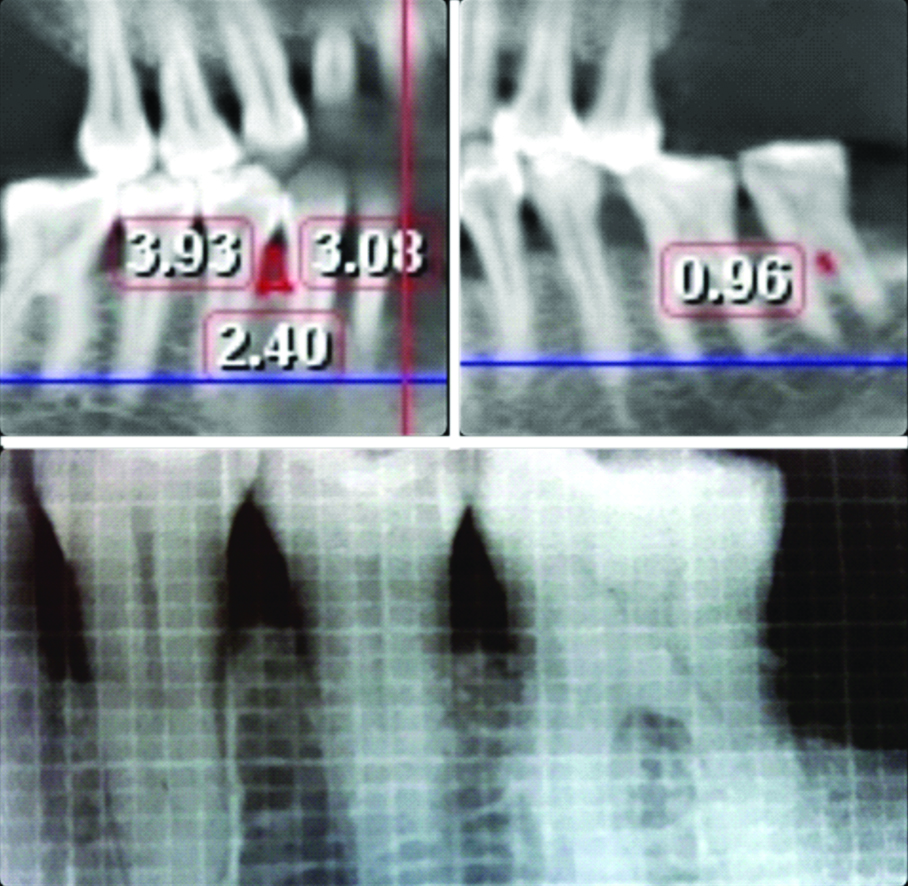
For CBCT scanning, a promax 3D CBCT device (PLANMECA, HELSINKI, FINLAND) was used. The occlusal plane of the jaws was positioned horizontally to the scan plane and mid-sagittal plane centered. The Field of view (FOV) WAS of 80 mm width and 80 mm height. Slice thickness of 0.2 mm and slice interval of 0.2 mm were obtained. 80Kv and 12 mAs using pulsed scanning time of 12 seconds were followed. The image obtained was measured using Romexis viewer 3.5.I.R software (PLANMECA, HELSINKI, FINLAND). The coronal, sagittal and axial planes are adjusted to intersect each other. The sagittal plane is adjusted until a clear image is visible in the sagittal view. The measurements for horizontal bone defects were made using saggital sections of the CBCT image, angular and furcation defect measurements were made in the panoramic mode of the CBCT. The panoramic view of the CBCT image has less magnification compared to the images obtained by OPG machines [Table/Fig-1,2].
Horizontal bone loss measured in the sagittal view of the CBCT, as the distance from the base of the bone defect to the CEJ.
Angular bone loss and furcation defects were made from the panoramic mode of CBCT; IOPA measurements were obtained by measuring the grid size of 1*1 mm from the base of the defect to the CEJ.
Intraoral Periapical Radiography
For IOPA, standardised long cone paralleling technique with grid was used (X-mind dc, ACETON GROUP, ITALY). The exposure setting was 70 Kvp with 8 mA, Focal spot 0.7 mm, and exposure time 0.02 to 3.2 seconds. A rectangular collimator and film holding system with standardised bite blocks were used. The films used were E speed Kodak Film [Table/Fig-2].
Direct Surgical Measurements
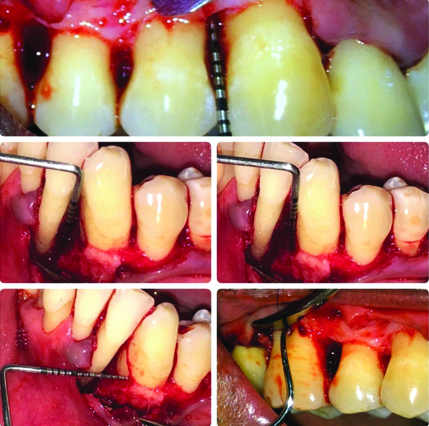
Following aseptic technique, after securing local anesthesia, a full thickness muco-periosteal flap was raised. After degranulation, scaling and root planing were performed and haemostasis was achieved. Clinical measurements were made. The surgical site was then irrigated with normal saline and flaps were sutured back and Periodontal pack applied. Post-operative instructions were provided to the patient along with antibiotic and analgesics. Suture removal was done on the 7th post-operative day. Once haemostasis was achieved, the type of defect was first identified [Table/Fig-3].
Direct surgical measurements in determining horizontal, angular bone loss and furcation involvement.
For horizontal bone loss: the distance between the CEJ and alveolar crest were measured using a UNC 15 probe placed in parallel to the long axis of the tooth. For the purpose of standardisation for horizontal defects, 6 sites around the tooth with defect were assessed- Mid-buccal, Mid-lingual (Mid-palatal), Mesio-buccal, Disto-buccal, Mesio-lingual (Mesio-palatal), Disto-lingual (Disto-palatal).
For angular bone loss: the measurements taken from each defect were: length from CEJ to the base of bony defect, length from CEJ to the crest of bone adjacent to the defect, width of the defect.
For furcation involvement: The horizontal furcation measurements were taken with a NABERS PROBE (Hu-Friedy) starting at the furcation entrance to the greatest horizontal depth. The vertical measurement was taken with a Hu-Friedy UNC probe starting at the furcation entrance and running the probe along the root surface until deepest vertical component is measured.
Furcation involvements were classified by looking at the horizontal component proposed by Hamp SE et al., (class I, class II and class III) and the vertical component proposed by Tarnow D et al., (subclass A, B and C) [10,11]. As there is discrepancy of the assigned ordinal data to this scale, only the main classes were used for the statistical analysis. A new classification system has been proposed by Vandenberghe B et al., where the horizontal component of furcation by Hamp SE et al., and vertical component of furcation by Tarnow D et al., are taken together [1,10,11]. For ease of statistical analysis, the subclasses of furcation classification proposed by Vandenberghe B et al., were assigned with numerical values starting from 0-9 such that: 0= No defect, 1=Degree I sub-class A, 2=Degree I sub-class B, 3=Degree I sub class C, 4=Degree II sub-class A, 5=Degree-II sub class B, 6=Degree II sub class C, 7=Degree III sub-class A, 8=Degree III sub-class B, 9=Degree III sub-class C.
The measurements taken during surgery were then compared to the measurements done with CBCT, IOPA and clinical probing for horizontal, angular bone defects and furcation involvement.
Statistical Analysis
The data collected were subjected to statistical analysis. The statistical constants like arithmetic mean, standard deviation and p-value were computed using SPSS 10.0 version software program. The p-value was significant at p<0.05. Pearson’s Intra-class correlation coefficient was used to determine the variability among the measurements by CBCT, IOPA and clinical probing compared with the direct bone measurements. Comparisons among the groups (CBCT, IOPA, clinical probing, direct surgical measurements were performed by means of Paired t-test. For furcation defects, only Intra-class correlation measurements were made. Direct surgical measurements were considered to be the gold standard as measurements were taken directly with a periodontal probe after opening the flap.
The interpretation of Intra class correlation coefficient is categorised as: <0.40=Poor agreement, 0.4-0.75=Fair agreement, 0.75-0.85=Good agreement, >0.85=Excellent agreement [12,13].
Results
Horizontal Bone Defects
Mesio-buccal
The standard deviation for measurements obtained from the Mesio-buccal area for direct surgical, CBCT, IOPA and clinical probing are given in [Table/Fig-4]. Highest Intra-class correlation of 0.992 is observed between the direct surgical and CBCT measurements compared to IOPA and clinical probing [Table/Fig-5]. Paired t-test revealed no statistically significant difference between direct surgical measurements and CBCT, whereas IOPA and clinical probing showed highly significant results [Table/Fig-6].
Errors (means and SDs) from direct surgical measurements using UNC-15 Probe, IOPA, CBCT and clinical probing in determining horizontal bone loss, angular bone loss and furcation involvement; measurements in mm. NA; values not available.
| Disto buccal | Disto lingual | Mesio-buccal | Mesio-lingual | Mid-buccal | Mid-lingual | CEJ/BASE | CEJ/CREST | Width | Furcation |
|---|
| Surgical measurement | 4.95±1.28 | 5.29±1.52 | 4.86±1.59 | 5±1.225 | 4.33±1.39 | 4.90±0.99 | 8.10±1.72 | 3.57±1.07 | 3.10±0.76 | 6.05±1.71 |
| CBCT | 4.99±1.28 | 5.52±1.50 | 4.95±1.53 | 5.12±1.17 | 4.48±1.37 | 5.05±0.99 | 8.29±1.74 | 3.93±1.57 | 3.25±0.80 | 5.81±1.88 |
| IOPA | 5.72±1.23 | 6.19±1.39 | 5.53±1.70 | 5.75±1.33 | NA | NA | 8.84±1.71 | 4.35±1.03 | 3.88±0.83 | 3.85±2.12 |
| Clinical probing | 6.33±1.27 | 6.81±1.32 | 6.33±1.52 | 6.52±1.12 | 5.81±1.12 | 6.48±0.81 | 9.62±1.68 | NA | NA | 2±1.64 |
Intra class correlation between the parameters involved in determining horizontal bone loss.
| Intra-class correlation | 95% Confidence interval | p-value | Significance |
|---|
| Lower | Upper |
|---|
| Distobuccal | Surgical/CBCT | 0.992 | 0.981 | 0.997 | p<0.05 | HS |
| Surgical/IOPA | 0.899 | -0.979 | 0.979 | p<0.05 | HS |
| Surgical/Probing | 0.708 | -0.191 | 0.926 | p<0.05 | HS |
| CBCT/IOPA | 0.907 | -0.101 | 0.981 | p<0.05 | HS |
| CBCT/Probing | 0.728 | -0.179 | 0.933 | p<0.05 | HS |
| IOPA/Probing | 0.885 | 0.296 | 0.966 | p<0.05 | HS |
| Distolingual | Surgical/CBCT | 0.991 | 0.693 | 0.998 | p<0.05 | HS |
| Surgical/IOPA | 0.886 | -0.135 | 0.974 | p<0.05 | HS |
| Surgical/Probing | 0.698 | -0.222 | 0.921 | p<0.05 | HS |
| CBCT/IOPA | 0.921 | 0.141 | 0.980 | p<0.05 | HS |
| CBCT/Probing | 0.745 | -0.249 | 0.932 | p<0.05 | HS |
| IOPA/Probing | 0.855 | 0.441 | 0.950 | P<0.05 | HS |
| Mesiobuccal | Surgical/CBCT | 0.992 | 0.981 | 0.997 | p<0.05 | HS |
| Surgical/IOPA | 0.934 | 0.255 | 0.983 | p<0.05 | HS |
| Surgical/Probing | 0.791 | -0.101 | 0.954 | p<0.05 | HS |
| CBCT/IOPA | 0.933 | 0.562 | 0.980 | p<0.05 | HS |
| CBCT/Probing | 0.791 | -0.157 | 0.951 | p<0.05 | HS |
| IOPA/Probing | 0.906 | 0.094 | 0.976 | p<0.05 | HS |
| Mesiolingual | Surgical/CBCT | 0.975 | 0.938 | 0.990 | p<0.05 | HS |
| Surgical/IOPA | 0.867 | -0.025 | 0.965 | p<0.05 | HS |
| Surgical/Probing | 0.643 | -0.139 | 0.907 | p<0.05 | HS |
| CBCT/IOPA | 0.865 | 0.313 | 0.958 | p<0.05 | HS |
| CBCT/Probing | 0.613 | -0.253 | 0.888 | p<0.05 | HS |
| IOPA/Probing | 0.769 | 0.097 | 0.923 | p<0.05 | HS |
| Midbuccal | Surgical/CBCT | 0.992 | 0.964 | 0.997 | p<0.05 | HS |
| Surgical/Probing | 0.660 | -0.212 | 0.909 | p<0.05 | HS |
| CBCT/Probing | 0.680 | -0.258 | 0.912 | p<0.05 | HS |
| Midlingual | Surgical/CBCT | 0.981 | 0.928 | 0.993 | p<0.05 | HS |
| Surgical/Probing | 0.507 | -0.098 | 0.853 | p<0.05 | HS |
| CBCT/Probing | 0.541 | -0.134 | 0.867 | p<0.05 | HS |
Paired t-test comparing CBCT, IOPA and clinical probing measurements to direct surgical measurements in determining horizontal bone loss.
| 95% Confidence interval | t value | p-value | |
|---|
| Lower | Upper |
|---|
| Disto-buccal | Surgical/CBCT | -0.1462 | 0.0605 | -0.865 | p>0.05 | NS |
| Surgical/IOPA | -0.915 | -0.636 | -11.607 | p<0.05 | HS |
| Surgical/Probing | -1.685 | -1.076 | -9.459 | p<0.05 | HS |
| CBCT/IOPA | -0.876 | -0.5906 | -10.717 | p<0.05 | HS |
| CBCT/Probing | -1.623 | -1.052 | -9.775 | p<0.05 | HS |
| IOPA/Probing | -0.882 | -0.327 | -4.541 | p<0.05 | HS |
| Disto-lingual | Surgical/CBCT | -0.314 | -0.1715 | -7.100 | p<0.05 | HS |
| Surgical/IOPA | -1.124 | -0.6853 | -8.599 | p<0.05 | HS |
| Surgical/Probing | -1.894 | -1.153 | -8.583 | p<0.05 | HS |
| CBCT/IOPA | -0.8915 | -0.432 | -6.013 | p<0.05 | HS |
| CBCT/Probing | -1.657 | -0.904 | -7.100 | p<0.05 | HS |
| IOPA/Probing | -0.994 | -0.243 | -3.441 | p<0.05 | HS |
| Mesio-buccal | Surgical/CBCT | -0.213 | 0.023 | -1.680 | p>0.05 | NS |
| Surgical/IOPA | -0.920 | -0.4319 | -5.775 | p<0.05 | HS |
| Surgical/Probing | -1.709 | -1.243 | -13.218 | p<0.05 | HS |
| CBCT/IOPA | -0.862 | -0.2998 | -4.310 | p<0.05 | HS |
| CBCT/Probing | -1.663 | -1.098 | -10.204 | p<0.05 | HS |
| IOPA/Probing | -1.082 | -0.517 | -5.901 | p<0.05 | HS |
| Disto-buccal | Surgical/CBCT | -0.1462 | 0.0605 | -0.865 | p>0.05 | NS |
| Surgical/IOPA | -0.915 | -0.636 | -11.607 | p<0.05 | HS |
| Surgical/Probing | -1.685 | -1.076 | -9.459 | p<0.05 | HS |
| CBCT/IOPA | -0.876 | -0.5906 | -10.717 | p<0.05 | HS |
| CBCT/Probing | -1.623 | -1.052 | -9.775 | p<0.05 | HS |
| IOPA/Probing | -0.882 | -0.327 | -4.541 | p<0.05 | HS |
| Disto-lingual | Surgical/CBCT | -0.314 | -0.1715 | -7.100 | p<0.05 | HS |
| Surgical/IOPA | -1.124 | -0.6853 | -8.599 | p<0.05 | HS |
| Surgical/Probing | -1.894 | -1.153 | -8.583 | p<0.05 | HS |
| CBCT/IOPA | -0.8915 | -0.432 | -6.013 | p<0.05 | HS |
| CBCT/Probing | -1.657 | -0.904 | -7.100 | p<0.05 | HS |
| IOPA/Probing | -0.994 | -0.243 | -3.441 | p<0.05 | HS |
| Mesiobuccal | Surgical/CBCT | -0.213 | 0.023 | -1.680 | p>0.05 | NS |
| Surgical/IOPA | -0.920 | -0.4319 | -5.775 | p<0.05 | HS |
| Surgical/Probing | -1.709 | -1.243 | -13.218 | p<0.05 | HS |
| CBCT/IOPA | -0.862 | -0.2998 | -4.310 | p<0.05 | HS |
| CBCT/Probing | -1.663 | -1.098 | -10.204 | p<0.05 | HS |
| IOPA/Probing | -1.082 | -0.517 | -5.901 | p<0.05 | HS |
| Mesio-lingual | Surgical/CBCT | -0.292 | 0.0350 | -1.640 | p>0.05 | NS |
| Surgical/IOPA | -1.021 | -0.4832 | -5.831 | p<0.05 | HS |
| Surgical/Probing | -1.798 | -1.250 | -11.608 | p<0.05 | HS |
| CBCT/IOPA | -0.936 | -0.311 | -4.161 | p<0.05 | HS |
| CBCT/Probing | -1.754 | -1.036 | -8.104 | p<0.05 | HS |
| IOPA/Probing | -1.178 | -0.364 | -3.955 | p<0.05 | HS |
| Mid-buccal | Surgical/CBCT | -0.2438 | -0.0515 | -3.203 | p<0.05 | HS |
| Surgical/Probing | -1.817 | -1.135 | -9.024 | p<0.05 | HS |
| CBCT/Probing | -1.6911 | -0.9661 | -7.645 | p<0.05 | HS |
| Mid-lingual | Surgical/CBCT | -0.2578 | -0.047 | -3.016 | p<0.05 | HS |
| Surgical/Probing | -1.802 | -1.341 | -14.201 | p<0.05 | HS |
| CBCT/Probing | -1.665 | -1.172 | -12.001 | p<0.05 | HS |
NS: No significant difference; HS: Highly significant
Mesio-lingual/Mesio-palatal
The standard deviation for measurements obtained from the Mesio-lingual/Mesio-palatal area for direct surgical, CBCT, IOPA and clinical probing are given in [Table/Fig-4]. Intra-class correlation of 0.975 is observed between the direct surgical and CBCT measurements which is greater than that of IOPA and clinical probing [Table/Fig-5]. Paired t-test revealed no statistically significant difference between direct surgical measurements and CBCT, whereas IOPA and clinical probing showed highly significant results [Table/Fig-6].
The CBCT and IOPA measurements were found to be in excellent agreement with the direct surgical measurements in both Mesio-buccal and Mesio-lingual/Mesio-palatal areas, where as clinical probing measurements were in moderate agreement with the direct surgical measurements. These results indicate that measurements obtained by CBCT were found to be superior over IOPA and clinical probing measurements in the Mesio-buccal and Mesio-lingual/ Mesio-palatal areas.
Mid-Buccal
The standard deviation for measurements obtained from the Midbuccal aspect for direct surgical, CBCT, IOPA and clinical probing are given in [Table/Fig-4]. Intra-class correlation of 0.992 is observed between the direct surgical and CBCT measurements which is greater than that of IOPA and clinical probing [Table/Fig-5]. Paired t-test revealed highly significant difference between direct surgical measurements and CBCT, IOPA and clinical probing [Table/Fig-6].
Mid-lingual/(Mid-palatal)
The standard deviation for measurements obtained from the Midlingual/Midpalatal region for direct surgical, CBCT, IOPA and clinical probing are given in [Table/Fig-4]. Highest Intra-class correlation of 0.981 is observed between the direct surgical and CBCT measurements [Table/Fig-5]. Paired t-test revealed highly significant difference between direct surgical measurements and CBCT, IOPA and clinical probing [Table/Fig-6].
The measurements from both the Mid-buccal and Mid-lingual/ (Mid-palatal) areas, indicate that CBCT was found to produce more accurate results compared to clinical probing. IOPA cannot measure the distance from the CEJ to the base of the defect in the Midbuccal and Midlingual/Midpalatal areas as it cannot determine the buccal and lingual cortical plates.
Disto-buccal
The standard deviation for measurements obtained from the Distobuccal region for direct surgical measurements, CBCT, IOPA and clinical probing are given in [Table/Fig-4]. Highest Intra-class correlation of 0.992 is observed between the direct surgical and CBCT measurements compared to IOPA and clinical probing [Table/Fig-5].
Paired t-test revealed no statistically significant difference between direct surgical measurements and CBCT, whereas IOPA and clinical probing showed highly significant results [Table/Fig-6].
Disto-lingual (disto-palatal)
The standard deviation for measurements obtained from the Disto Disto-lingual/Disto-palatal region for direct surgical, CBCT, IOPA and clinical probing are given in [Table/Fig-4]. Intra-class correlation of 0.991 is observed between the direct surgical and CBCT measurements which is greater than that of IOPA and clinical probing. [Table/Fig-5]. Paired t-test revealed highly significant difference between direct surgical measurements and CBCT, IOPA and clinical probing. [Table/Fig-6]. Also, in the Disto-buccal and Disto-lingual/Disto-palatal areas, both CBCT and IOPA measurements was found to be in excellent agreement with direct surgical measurements, whereas clinical probing measurements only showed a moderate agreement with the direct measurements.
Overall CBCT showed more accurate results than IOPA and clinical probing in determining horizontal bone defects around the tooth. There was no statistically significant difference between the CBCT and direct surgical measurements in the Mesio-buccal, Mesio-lingual/Mesio-palatal, Disto-buccal areas.
IOPA cannot be used as a reliable tool for measuring bone loss in the Midbuccal, Midlingual/Midpalatal areas, since it gives a two dimensional image of a three dimensional object.
Angular Bone Loss
Distance from CEJ to the base of bony defect
The standard deviation values for direct surgical measurements, CBCT, IOPA and clinical probing which measured the distance from CEJ to base of the bony defect are given in [Table/Fig-4]. Highest Intra-class correlation of 0.993 is observed between the direct surgical and CBCT measurements. Both CBCT and IOPA measurements showed excellent agreement with the direct surgical measurements whereas in clinical probing the agreement was moderate. CBCT produced slightly more accurate measurements than IOPA [Table/Fig-7]. Paired t-test revealed highly significant difference between direct surgical measurements and CBCT, IOPA and clinical probing [Table/Fig-8].
Intra class correlation among different parameters in determining angular bone loss.
| 95% Confidence interval | Intra-class correlation | p-value | Significance |
|---|
| Lower | Upper |
|---|
| CEJ/Base | Surgical/CBCT | 0.954 | 0.998 | 0.993 | p<0.05 | HS |
| Surgical/IOPA | -0.037 | 0.990 | 0.949 | p<0.05 | HS |
| Surgical/Probing | -0.093 | 0.959 | 0.813 | p<0.05 | HS |
| CBCT/IOPA | 0.102 | 0.993 | 0.968 | p<0.05 | HS |
| CBCT/Probing | -0.148 | 0.964 | 0.839 | p<0.05 | HS |
| IOPA/Probing | 0.096 | 0.982 | 0.926 | p<0.05 | HS |
| CEJ/Crest | Surgical/CBCT | 0.699 | 0.954 | 0.883 | p<0.05 | HS |
| Surgical/IOPA | -0.131 | 0.968 | 0.854 | p<0.05 | HS |
| CBCT/IOPA | 0.645 | 0.950 | 0.870 | p<0.05 | HS |
| Width | Surgical/CBCT | 0.858 | 0.992 | 0.974 | p<0.05 | HS |
| Surgical/IOPA | -0.089 | 0.952 | 0.783 | p<0.05 | HS |
| CBCT/IOPA | -0.174 | 0.962 | 0.835 | p<0.05 | HS |
Paired t-test comparing CBCT, IOPA and clinical probing measurements to direct surgical measurements in determining angular bone loss.
| Furcation involvement | Intra-class correlation | 95% Confidence interval | p-value | Significance |
|---|
| Upper | Lower |
|---|
| Surgical/CBCT | 0.950 | 0.878 | 0.980 | p<0.05 | HS |
| Surgical/IOPA | 0.616 | -0.296 | 0.885 | p<0.05 | HS |
| Surgical/Clinical probing | 0.152 | -0.189 | 0.542 | p>0.05 | NS |
| CBCT/IOPA | 0.663 | -0.296 | 0.898 | p<0.05 | SIG |
| CBCT/Clinical probing | 0.201 | -0.220 | 0.610 | p<0.05 | SIG |
| IOPA/Clinical probing | 0.434 | -0.337 | 0.772 | p<0.05 | SIG |
Distance from CEJ to the Crest of Bone Adjacent to the Defect
The standard deviation values for direct surgical measurements, CBCT, IOPA and clinical probing which measured the distance from CEJ to the crest of bone adjacent to the defect are given in [Table/Fig-4]. Highest Intra-class correlation of 0.883 is observed between the direct surgical and CBCT measurements compared to IOPA and clinical probing. Both CBCT and IOPA measurements showed excellent agreement with the direct surgical measurements, with superior result favoring CBCT [Table/Fig-7]. Paired t-test revealed no statistically significant difference between direct surgical measurements and CBCT, IOPA showed highly significant results, whereas clinical probing showed significant difference [Table/Fig-8].
Width of the Defect
The standard deviation values for direct surgical measurements, CBCT, IOPA and clinical probing in measuring the width of the defect are given in [Table/Fig-4]. Highest Intra-class correlation of 0.974 is observed between the direct surgical and CBCT measurements compared to other modalities. CBCT measurements showed excellent agreement with the direct surgical measurements compared to IOPA measurements in determining the width of the defect [Table/Fig-7,8].
Furcation Defects
The standard deviation values for direct surgical measurements, CBCT, IOPA and clinical probing are given in [Table/Fig-4]. Highest intra-class correlation of 0.95 is observed between the direct surgical and CBCT measurements compared to all other parameters [Table/Fig-9].
Intra class correlation between Direct surgical, CBCT, IOPA and Clinical probing measurements involved in determining furcation involvement.
| Furcation involvement | Intra-class correlation | 95% Confidence interval | p-value | Significance |
|---|
| Upper | Lower |
|---|
| Surgical/CBCT | 0.950 | 0.878 | 0.980 | p<0.05 | HS |
| Surgical/IOPA | 0.616 | -0.296 | 0.885 | p<0.05 | HS |
| Surgical/Clinical probing | 0.152 | -0.189 | 0.542 | p>0.05 | NS |
| CBCT/IOPA | 0.663 | -0.296 | 0.898 | p<0.05 | SIG |
| CBCT/Clinical probing | 0.201 | -0.220 | 0.610 | p<0.05 | SIG |
| IOPA/Clinical probing | 0.434 | -0.337 | 0.772 | p<0.05 | SIG |
CBCT measurements were almost equal to direct surgical measurements which showed an excellent agreement. The agreement between IOPA and direct surgical measurements was moderate. However, determination of horizontal component of the furcation by means of clinical probing showed poor agreement with the direct surgical measurements. Overall, CBCT is capable of producing excellent results in determining both the horizontal and vertical component of furcation compared to IOPA and clinical probing.
Discussion
A total of 63 defects were evaluated in this study. The results from the study indicated that CBCT is highly accurate for diagnosing both horizontal and vertical bone defect and assessing horizontal and vertical component of the furcation involvement. Furthermore, there is a high degree of correlation between measurements obtained after opening the flap (direct surgical measurements) which was considered to be gold standard and CBCT measurements of bone defects.
According to the results obtained, overall CBCT showed more accurate results than IOPA and clinical probing in determining horizontal bone defects around the tooth. There was no statistically significant difference between the CBCT and direct surgical measurements especially in the mesio-buccal, mesio-lingual/mesio-palatal and disto-buccal areas. In the mid-buccal/mid-lingual areas, CBCT produced more accurate measurements than clinical probing. Since IOPA couldn’t identify the buccal and lingual cortical plates, it cannot be used as a reliable tool for measuring bone loss in the midbuccal, midlingual/midpalatal areas.
These results are consistent with the results of other in-vivo studies by Misch KA et al., Grimard BA et al., de FariaVasconcelos K et al., [14-16]. However, this study was not in accordance with the study by Leung CC et al., where they found low accuracy of CBCT images in determining bone defects due to the limitations in the spatial resolution of the CBCT device used [17]. This study is one of the few studies that have evaluated and compared CBCT measurements of periodontal defects with actual surgical measurements in vivo.
The study by Vandenberghe B et al., showed that although CBCT image measurements of periodontal bone levels were comparable to those by digital intraoral radiography, both techniques under- and overestimated actual linear measurements [18]. Conversely, in this study, CBCT measurements overestimated actual surgical measurements by 0.4 mm in measuring horizontal bone defects. Since a 0.5-1 mm discrepancy between actual bone level and radiographically estimated bone levels is considered clinically acceptable [4,19], CBCT and direct surgical measurements were assumed to be similar in this study.
For angular bone loss, CBCT produced measurements almost similar to direct surgical measurements in measuring distance from CEJ to base of the bony defect, distance from CEJ to the crest of the bone adjacent to the defect and width of the defect. The results obtained by IOPA and clinical probing only showed moderate agreement with the direct surgical measurements. These results are consistent with the results of all the previous studies by Banodkar AB et al., and Deng Y et al., [5,20].
Furcation involvements were classified by looking at the horizontal component proposed by Hamp SE et al., (class I, class II and class III) and the vertical component proposed by Tarnow D et al., (subclass A, B and C). A new classification system has been proposed by Vandenberghe B et al., where the horizontal component of furcation by Hamp SE et al., and vertical component of furcation by Tarnow D et al., is taken together.
Of the furcation involvements, 62% were detectable with IOPA technique in this study. In contrast CBCT allowed 95% detection of furcation involvements. The clinical probing appears to be the least reliable technique in determining furcation involvement. Studies by Qiao J et al., Umetsubo OS et al., also found CBCT to be highly accurate in determining furcation involvement [21,22]. This study is also in accordance with the findings by Walter C et al., where they stated that CBCT could improve diagnosis validity and periodontal treatment planning optimisation, especially in cases of furcation involvement in molars [23].
A variety of similar studies which assessed the accuracy of CBCT in determining horizontal bone loss, angular bone loss and furcation involvement with their observation are given in [Table/Fig-10] [1,5,14-16,20-24].
A variety of studies with observations similar to the present study are discussed in detail [1,5,14-16,20-24].
| Study characteristics (Author, Year, Country) | Samples Involved | Methodology | Results/Conclusion |
|---|
| Banodkar AB et al., [5] 2015, India | 100 periodontal defects from 15 patients | CBCT vs. Surgical measurements. | Found CBCT to be highly accurate in measurement of both horizontal and vertical bone defects.High degree of correlation of 0.988 exists between surgical and CBCT measurements of bone defects. |
| Deng Y et al., [20] 2015, China | 75 patients, 8964 sites, horizontal and vertical defects | CBCT vs. Periapical film, Panoramic radiograph and Clinical examination | Only CBCT detected buccal and palatal alveolar bone destruction. Compared with other parameters CBCT showed significant differences (p<0.01) in alveolar bone defect measurements in mesial and distal side. There was no significant difference between clinical probing {mesial: (5.5±0.6), distal: (5.5±0.6) mm} and CBCT. {mesial: (5.5±0.4), distal: (5.6±0.8) mm}. |
| Qiao J et al., [21] 2014, China | 15 chronic generalised periodontitis patients, 20 maxillary molars | CBCT vs. Surgical measurements | Intra-surgical findings confirmed 82.4% of the CBCT data, with a weighted kappa of 0.917.CBCT demonstrated high accuracy in assessing the loss of periodontal tissue in furcation area of maxillary molars. |
| Mohan R et al., [24] 2014, India | Patient with aggressive periodontitis | Initially clinical examination and direct digital radiography showed advanced periodontal destruction.CBCT was then taken to identify the morphology of osseous lesions around all teeth. Measurements were then taken after opening the flap and compared with CBCT measurements. | CBCT measurements are as accurate as measurement obtained during surgery with a periodontal probe.Buccal and lingual defects could be identified compared to direct digital radiography. |
| de Faria Vasconcelos K et al., [16] 2012, Brazil | 51 sites, horizontal and vertical bone loss. | CBCT vs. IOPA | Both methods were identical in detecting depth and width of the defect (p-values >0.05)However differs in identifying the height of the alveolar bone. (Average 3.8 mm for IOPA, 4.1 for CBCT).CBCT helped in identifying buccal and lingual surfaces, also improved visualisation of the morphology of the defect. |
| Walter C et al., [23] 2012, Switzerland | 12 patients with chronic periodontitis, 22 maxillary molars | Financial benefit of CBCT with periodontal surgery for the treatment options of maxillary molars vs. Extraction followed by implant placement. | Average cost reduction from CBCT amounted to 915±1470 and saved 136±217 min.CBCT facilitated a reduction in treatment costs and time for periodontally involved maxillary molars. |
| Umetsubo OS et al., [22] 2012, Brazil | 15 macerated pig mandibles. | CBCT vs. Direct measurements obtained from simulated furcation lesions and area without simulated lesions. | CBCT showed high levels of accuracy, ranging from 78% to 88%.CBCT can be considered a reliable and accurate method for detecting incipient furcation involvement. |
| Grimard BA et al., [15] 2009, USA | 35 Intrabony defects | CBCT, Digital Intra Oral Radiography (IR) vs. Direct Surgical measurements. | CBCT correlated strongly with surgical measurements (r=0.89 to 0.95), whereas IRs correlated less favorably (r=0.53 to 0.67).CBCT was significantly more precise and accurate than IRs |
| Vandenberghe B et al., [1] 2007, Belgium | 41 periodontal defects of human skulls | 2D digital radiography, 3 dimensional CBCT vs. direct skull observation. | Compared to direct skull measurements, CBCT significantly detected craters and furcation (p=0.374, p=1.00 respectively for CBCT vs. IOPA.CBCT found to be more accurate in assessment of periodontal craters and furcation involvement. |
| Misch KA et al., [14] 2006, USA | Dry skulls, artificial osseous defects created on mandible | IOPA, CBCT and clinical probing measurements vs. Electronic caliper measurements. | A significant difference exists when comparing isolated interproximal measurements using a probe versus the caliper (p<0.001) but no significant difference for CBCT or IOPA.CBCT had an added advantage that the defect can be quantified. Buccal and lingual defects could not be measured with IOPA. |
Limitation
Although CBCT was found to be highly accurate in measuring periodontal defects, this study only assessed 21 sites each in determining horizontal bone loss, angular bone loss and furcation involvement. Further studies with larger sample size are to be conducted to validate the findings of this study.
The measurements were carried out by using CEJ as a reference point. The use of surgical stent may provide more accurate measurements, in case if CEJ is not adequately demarcated, which in turn can be used as a standard reference point. The factors like angulation of the probe, probing force may also influence the results.
Conclusion
CBCT allowed more accurate assessment of horizontal, angular bony defects and furcation involvements than IOPA and clinical probing. CBCT produced measurements almost similar to direct surgical measurements in disto-buccal, mesio-buccal and mesio-lingual areas for horizontal bone loss and also measuring distance from CEJ to base of the bony defect, distance from CEJ to the crest of the bone adjacent to the defect and width of the defect. 95% of the furcation defects were detected with CBCT whereas only 62% of the furcation defects were detected with IOPA in this study.
This study might help in establishing selection criteria for different imaging modalities in assessment of periodontal bone loss and further assist in periodontal diagnosis and treatment planning.