Case Report
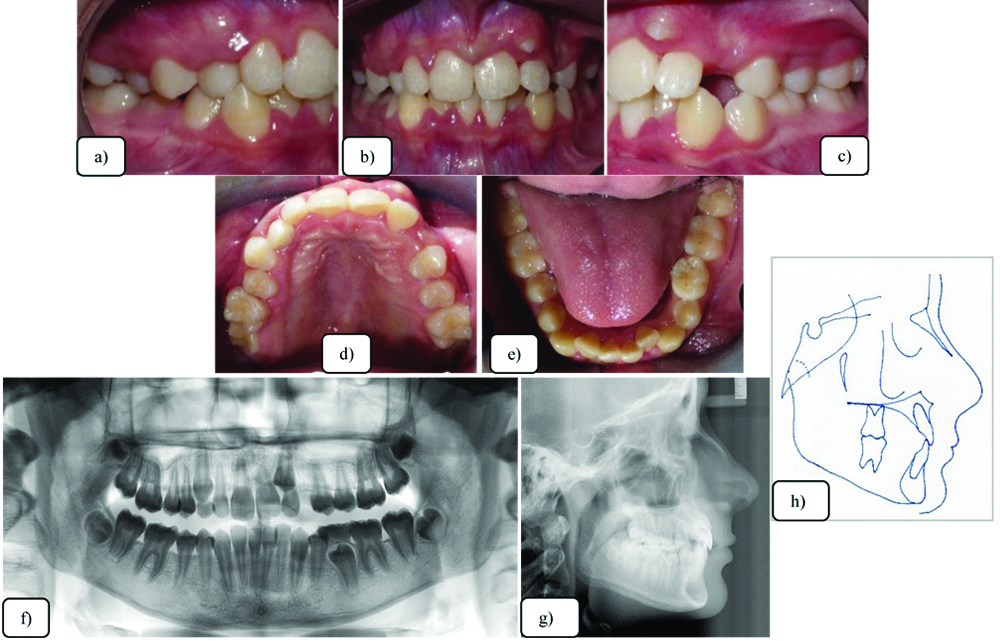
A 11 years 9-months-old female patient sought orthodontic consultation as indicated by her general practitioner with the chief complaint of “Mal-aligned teeth in the front tooth region”. She was in good general health with no relevant medical and dental history. On extraoral examination, the profile was slightly convex. Intraoral examination revealed a Class I mixed dentition, with delayed exfoliation of posterior deciduous teeth, including the maxillary canines. There was 3.0 mm overjet and exaggerated overbite. The maxillary midline was deviated 1,0 mm to the left and the lower midline coincided with the facial midline, and severe crowding in the upper and moderate in lower arch, with the crown of the upper left central incisor overlapping the lateral incisor crown [Table/Fig-1].
Phase I intraoral photographs- a) right lateral intraoral image; b) frontal image c) left lateral intraoral image d) maxillary occlusal view e) Mandibular occlusal view f) transposition of the upper left canine between the lateral and central incisor g) panoramic radiograph, h) cephalometric radiograph, and i) cephalometric tracing.
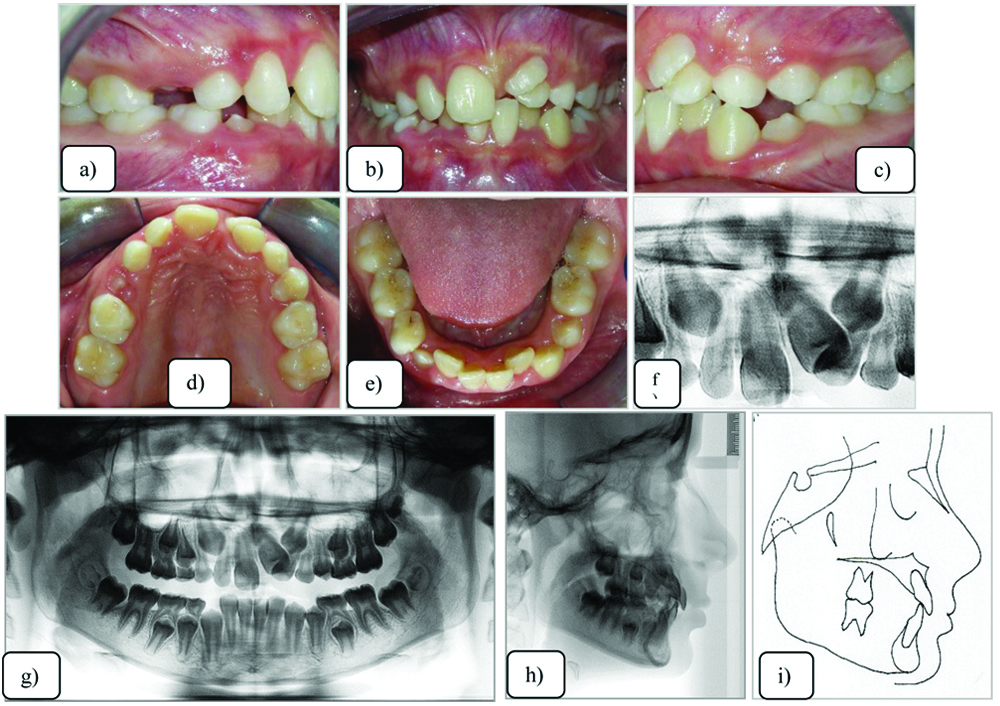
The panoramic radiograph confirmed the delayed eruption of the permanent dentition. The upper left canine was unfavourably positioned, with the crown positioned distally to the left central incisor and mesially to the lateral incisor, apparently with complete transposition characteristics of the upper left canine, between the lateral and central incisor [Table/Fig-1].
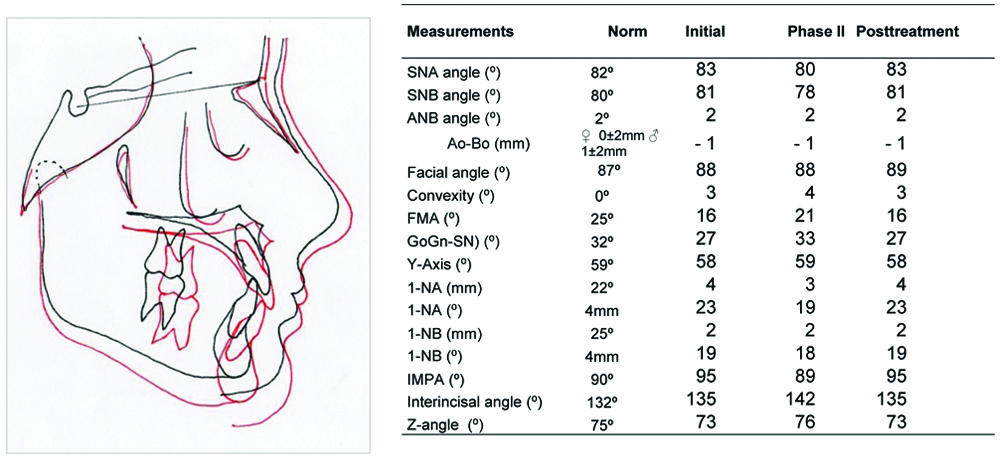
Cephalometric analysis presented a skeletal Class I malocclusion (ANB=2°), brachyfacial pattern (FMA=16°), maxillary and mandibular incisors were slightly uprighted (1NB=19°), and a good profile (Z-angle=73°).
Treatment Objectives
The patient was treated in 2 phases. The objective of phase I was to expand the maxilla and align the left and right upper incisors.
In phase II, the comprehensive treatment objectives were to: (1) establish functional Class I molar and canine relationships; (2) level and align the arches; (3) correct the transposition and restore natural tooth order; (4) create ideal overbite and overjet; and (5) correct incisor inclinations and root angulations. The overall objective was to provide the patient with improved aesthetics and a functioning occlusion.
Treatment Alternatives
A) Maxillary expansion with HYRAX type palatal expander to increase the arch perimeter;
B) attempt the distal movement of the upper left canine and position it in its place in the dental arch;
C) extraction of the upper left canine in transposition;
D) extraction of the left upper lateral incisor and position the canine in its place; and
E) possibility to perform stripping to minimise the projection of the lower incisors.
Transposed canine, the alignment of the malposed teeth and non-extraction was the most conservative treatment plan. A mini-implant was used in the left molar region to retract the transposed canine and correct the Class I malocclusion in phase II. The transposed canine was maintained in a high position as it was retracted to minimise possible root resorption.
Treatment Progress
Before orthodontic treatment, the patient was referred to the general dental practitioner for routine clinical procedures. All treatment alternatives were explained to the patient and her mother, and alternatives A and B were selected. They signed a consent form. The patient was informed of the associated risks, need for cooperation in hygiene maintenance, use of intermaxillary elastics, and the possibility of prolonged treatment time, more than 36 months.
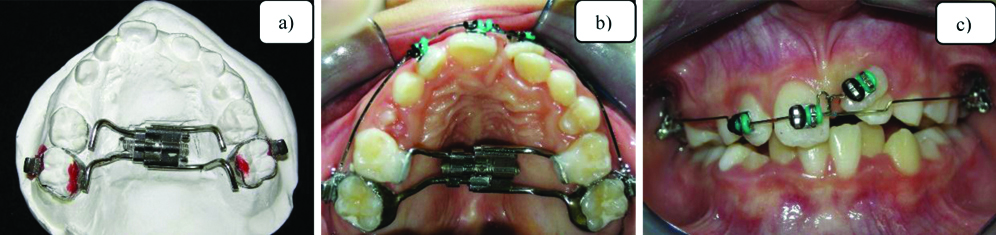
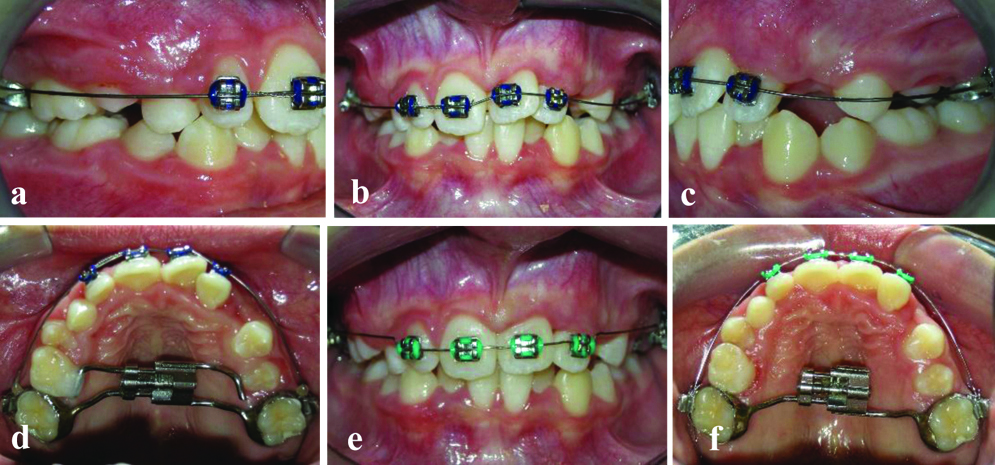
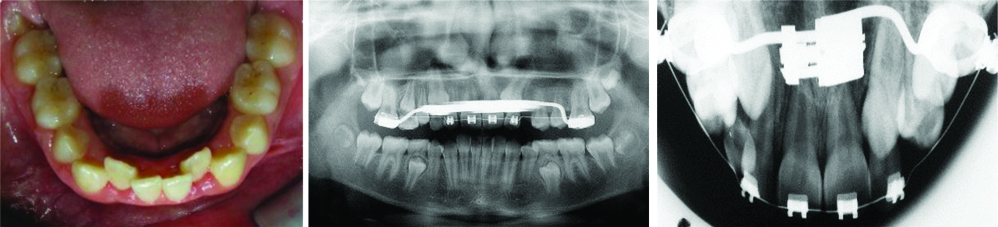
In the first stage, the HYRAX palatal expander was cemented on the permanent maxillary first molars [Table/Fig-2] and remained for 26 months initially, as stabilisation of the expansion was obtained and during the alignment, levelling of the central incisors and left upper lateral incisor as anchorage was done. A .022×.028-in standard edgewise brackets were placed on the incisors. The first .016-in SS archwire was made with mesial loop to the right upper central incisor to level the left central [Table/Fig-2]. The second archwire was the .016 “NiTi Thermal for alignment of the upper incisors [Table/Fig-3]. In this phase, as the second lower deciduous molars exfoliation was delayed the extractions were advised [Table/Fig-4].
a) HYRAX palatal expander; b) HYRAX palatal expander cemented on maxillary first molars; c) beginning of the movement of the upper left central incisor.
Progress. Alignment of upper incisors {(a) right lateral image; (b) frontal image; (c) left lateral image}. (d) Stabilisation of HYRAX; (e) Incisors aligned; and (f) removal of mesial bar of the HYRAX.
Progress. HYRAX stabilised for 26 months.
In the second comprehensive stage [Table/Fig-5], Class I irregularity was observed in the lower anterior teeth segment. There was initiation of eruption of the upper left canine between the crowns of the central and lateral incisors. A complete transposition was observed on the panoramic radiograph [Table/Fig-5]. The patient had a good lower facial profile.
Initial phase II, comprehensive treatment: a) right lateral view; b) Frontal intraoral image; c) intraoral left lateral image showing Upper left canine erupting between the central and lateral incisors; d) phase II treatment- maxillary occlusal view; e) mandibular occlusal view; f) Panoramic radiograph; g) cephalometric radiograph; and h) cephalometric tracing.
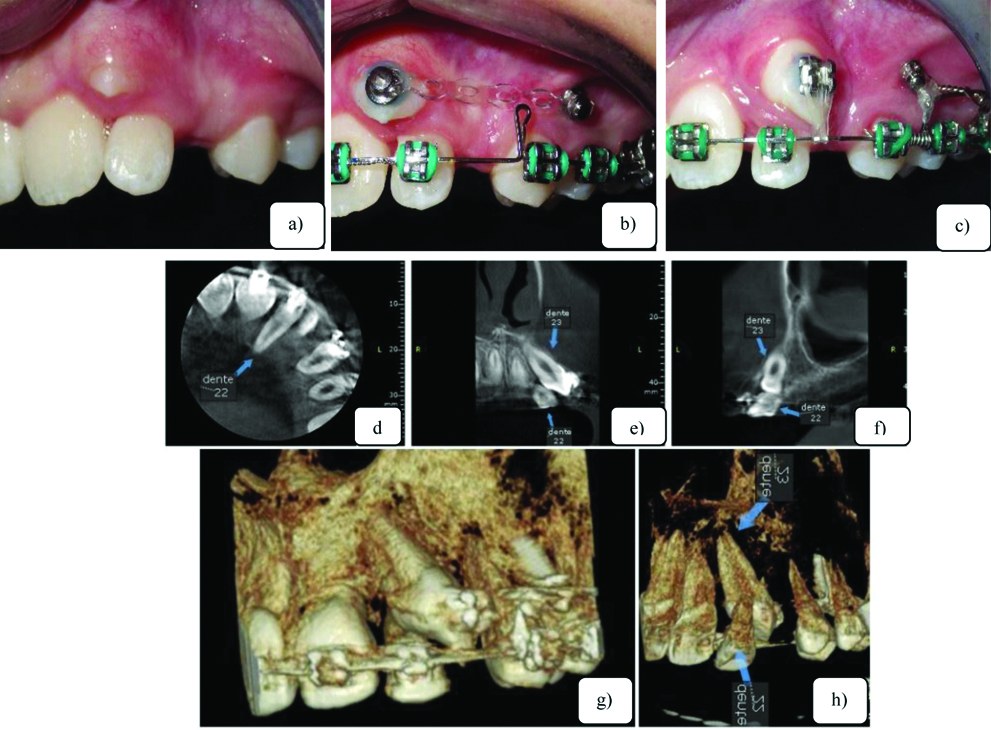
Correction of the transposition was initiated by bonding brackets with inclusion of the premolars and a 0.018×0.025-in archwire for three-dimensional biomechanical control. The root of the left lateral incisor was moved palatally to allow the movement of the crown to distal the canine [Table/Fig-6]. In this phase, due to the magnitude of the positioning of the root of the lateral incisor to the palatal side, the possibility of extracting and replacing the canine was discussed, followed by the closure of the space moving the posterior teeth mesially ([Table/Fig-6], CBCT). Toward the end of treatment, increased labial-palatal torque was placed on the lateral incisor. The diastema between central and lateral incisor was closed with an artistic bend placed into the lateral incisor. The position of the mini-implant, which was placed between the first and second premolars, favoured distal movement without loss of anchorage of the left hemi-arch teeth [Table/Fig-7].
a-c) Progress. Left upper canine movement supported on mini-implant; (d-f) Root of the left lateral incisor significantly positioned in palatal side; (g,h) movement of the canine.
a-c) Progress. Finishing stage with the upper left canine positioned in Class I; (d) The diastema between central and lateral incisor was closed with an artistic bend placed into the lateral incisor; (e,f) Standard torque in the left central incisor; (g-i) Buccal root torque in the lateral incisor.
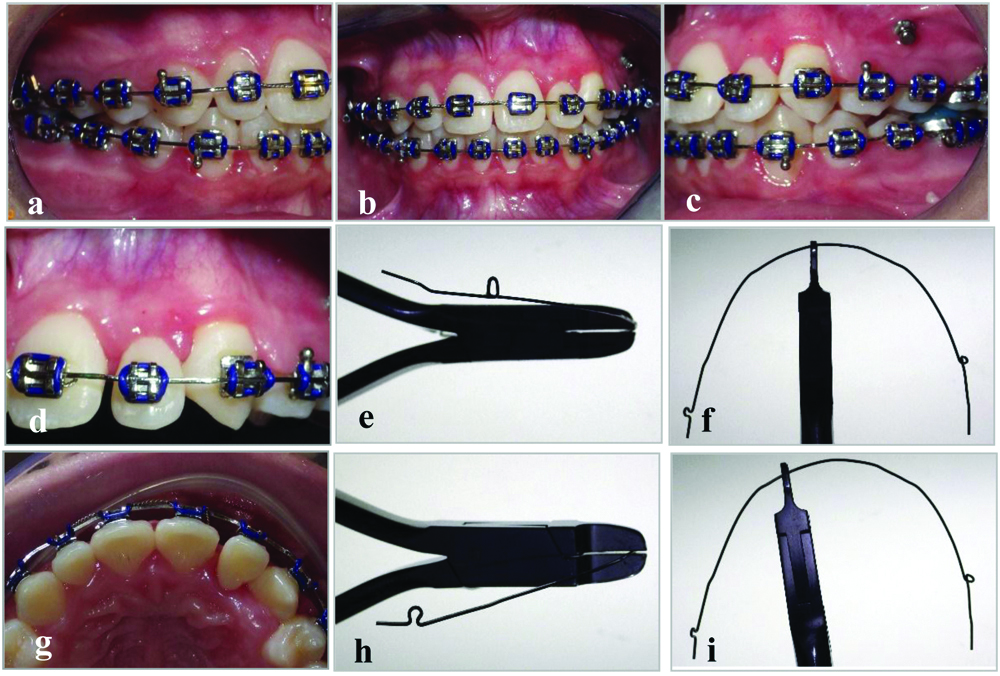
The lateral incisor was pulled palatally away from the canine roots. When the canine crown was no longer at risk, a labial root torque of the lateral incisor was included in the archwire [Table/Fig-7]. The first premolar was moved distally with a push coil spring until the premolars and molars achieved Class I relationship.
Treatment Results
The canine was positioned in its proper location in the dental arch. Third-order (torque) bends was generated in the arch to move the lateral incisor root buccally in Class I occlusion with health, aesthetics, function and gingival and periodontal health.
After 40 months of active treatment, the patient was debonded, and was retained with maxillary removable wraparound type and a mandibular fixed canine-to-canine retainer. The treatment was complex but gave excellent aesthetic and functional results. Intraoral posttreatment records show that the canines were aligned with the transposition corrected [Table/Fig-8]. The final positioning of the canines and lateral incisor were clinically balanced. Class I molar and canine relationships were established with ideal overjet and overbite. The radiographs showed correction of the transpositions with parallelism of the roots. The lateral incisors’ root lengths were maintained during the treatment [Table/Fig-8].
a-c) Post-treatment intraoral photographs; d-f) maxillary removable wraparound type and a mandibular fixed canine-to-canine retainer; g) panoramic radiograph; h) cephalometric radiograph; and i) cephalometric tracing.
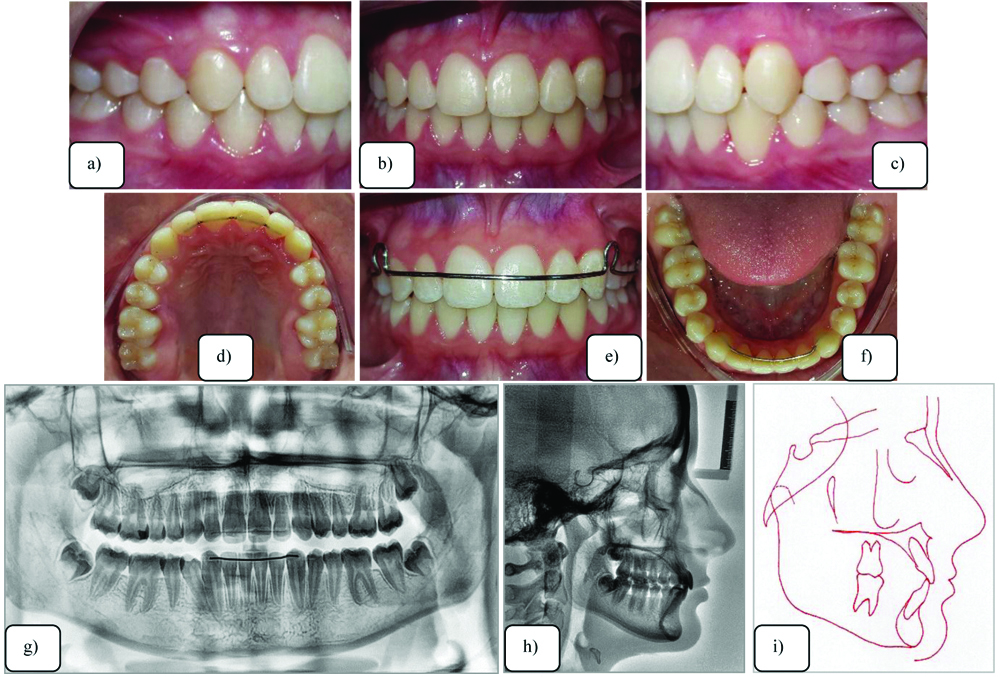
After the transposition correction, the gingival levels of both canines were anatomically correct with no recession, buccally or palatally. The periodontal tissues were healthy with no periodontal pockets or recession evident on clinical examination. The total cephalometric superimposition revealed that the upper and lower incisors were uprighted, and the good lower facial profile was maintained [Table/Fig-9].
Superimposition of the initial and final cephalometric tracings. Table with initial and final cephalometric measurements.
After one year of follow-up, the gingival levels of both canines were anatomically maintained with no recession, buccally or palatally. Overjet and overbite, as well as the molar and canine relationships, remained unchanged [Table/Fig-10].
One year follow-up intraoral photographs.

Discussion
A complete maxillary canine and lateral incisor transposition is a complex anomaly that presents a significant orthodontic challenge. The treatment of the present clinical case was complex and aimed to solve the transposition with the least tissue or root damage possible. The treatment plan was personalised to the patient’s specific needs, giving her excellent aesthetic and function by moving the canine to its correct position, resulting in a good long-term prognosis.
Although the main goal of the treatment of all transposition abnormalities is to correct the position of transposed teeth. Patient’s age, occlusion, aesthetics and treatment length, should be taken into consideration [1]. Thus, the orthodontist must come up with a meticulous and comprehensive treatment plan.
The treatment option chosen for this patient was orthodontic correction. To prevent resorption of the lateral incisors, the root was moved. The position of the lateral incisor root is critical when electing the correct treatment and biomechanics for each patient [2]. A successful orthodontic result is often predicted on the design of the force system [3]. The infrazygomatic crest is a convenient placement site in the maxilla for orthodontic mini-screws or mini-plates [4], but in this clinical case, the mini-screw was placed little bit downward, with the same success.
If the transposition is complete, correcting the transposed order is complex and may damage the teeth or supporting structures [5]. In this case, the possibility of extracting the lateral incisor and replacing the canine in transposition was discussed, considering the complexity of the case and the risk of reabsorption of the lateral incisor root. However, the application of the technique and biomechanics provided the final satisfactory result, with the left central and lateral incisors with minimal resorption compared to the panoramic radiograph at the beginning of the treatment and the canine in Class I.
It appeared that there was resorption before and after treatment on the maxillary lateral incisors involved in these corrected transpositions. Becker A and Chaushu S, recommend to distance the canine from the lateral root to prevent any further resorption [6]. In this clinical case, the recommendation was applied, and all teeth remained vital with successful aesthetic and functional results outweighing the minimal resorption that was evident.
Orthodontic correction of tooth transposition is not clinically feasible for all cases, because factors such as age, occlusion, patient’s compliance, tooth inclination, initial root positioning, and alveolar bone quality must be taken into account to move transposed teeth. Additionally, the approach demands longer treatment time as well as meticulous torque and direction of force control to move the transposed teeth while preserving buccal bone cortex [7].
The treatment took 40 months as the treatment timing for transposed teeth was considered. Expected duration of treatment, cooperation, periodontal support, age, the patient’s aesthetics, occlusion discrepancy, root apex positions, are all the factors a clinician should carefully consider.
The torque was added into the archwire, but the versatility of the bracket used by Antelo OM et al., with the bracket bonded on the lateral incisor in an inverted manner, that is, with a rotation of 180° to express a negative torque of -10° in a clinical case with the upper lateral incisor for palatine and anterior crossbite, in which biomechanics were expressed efficiently without the insertion of folds in the orthodontic arch [8].
Conservative correction of the problem entails risks that require carefully controlled appliances [3]. For this patient, a temporary anchorage device provided an independent force system for retracting the transposed canine and correcting the Class II relationship of the entire maxillary arch.
Therefore, even with the use of pre-adjusted brackets, the professional must know that the biomechanics and the system prescription have technical ability and clinical capacity to favour the individualised treatment of transposition malocclusion, as illustrated in this clinical case.
Conclusion
Correction of the transposition was performed with a fixed appliance for three-dimensional biomechanical control. The root of the left lateral incisor was moved palatally. The position of the mini-implant favoured distal movement without loss of anchorage of the teeth of this hemi-arch (left). With the canine positioned in place, third-order bends were inserted in the arch to move the lateral incisor root buccally. The canine was positioned in Class I in the line of occlusion with health, aesthetics, function and gingival and periodontal health, which remained stable after a 1-year follow-up, demonstrating that the applied biomechanics were correct.
[1]. Venkataraghavan K, Athimuthu A, Prasanna P, Jagadeesh RB, Transposition of mandibular lateral incisor-canine (mn.i2.C) associated with hypodontia: a review and rare clinical caseJ Clin Diagn Res 2014 8:ZE04-06.10.7860/JCDR/2014/7961.427824959525 [Google Scholar] [CrossRef] [PubMed]
[2]. Lorente T, Lorente C, Murray PG, Lorente P, Surgical and orthodontic management of maxillary canine-lateral incisor transpositionsAm J Orthod Dentofacial Orthop 2016 150:876-85.10.1016/j.ajodo.2016.04.02627871714 [Google Scholar] [CrossRef] [PubMed]
[3]. Hsu YL, Chang CH, Roberts WE, Canine-lateral incisor transposition: Controlling root resorption with a bone-anchored T-loop retractionAm J Orthod Dentofacial Orthop 2016 150:1039-50.10.1016/j.ajodo.2015.10.03627894525 [Google Scholar] [CrossRef] [PubMed]
[4]. Liou EJ, Chen PH, Wang YC, Lin JC, A computed tomographic image study on the thickness of the infrazygomatic crest of the maxilla and its clinical implications for miniscrew insertionAm J Orthod Dentofacial Orthop 2007 131:352-56.10.1016/j.ajodo.2005.04.04417346590 [Google Scholar] [CrossRef] [PubMed]
[5]. Shapira Y, Kuftinec MM, Tooth transpositions-a review of the literature and treatment considerationsAngle Orthod 1989 59:271-76. [Google Scholar]
[6]. Becker A, Chaushu S, Long-term follow-up of severely resorbed maxillary incisors after resolution of an etiologically associated impacted canineAm J Orthod Dentofacial Orthop 2005 127:650-54.quiz 75410.1016/j.ajodo.2004.03.03115953888 [Google Scholar] [CrossRef] [PubMed]
[7]. Matsumoto MAN, Stuani MBS, Tooth transposition: a multidisciplinary approachDental Press J Orthod 2018 23:97-107.10.1590/2177-6709.23.1.097-107.bbo29791689 [Google Scholar] [CrossRef] [PubMed]
[8]. Antelo OM, Meira TM, Giacobbo LC, Saga AY, Tanaka OM, The versatility of the pre-adjusted bracket for the maxillary lateral incisor in case of crossbiteOrthod Sci Pract 2017 10:201-12.[Translated from Portuguese]10.24077/2017;1039-201212 [Google Scholar] [CrossRef]