Introduction
Occupational health means preventive and curative medicine that deals with every aspect of health as well as safety in the workplace with primary prevention of hazards. “Occupational health should aim at the promotion and maintenance of the highest degree of physical, mental and social wellbeing of workers in all occupation” [1]. The awareness regarding occupational health help in the prevention of specific health problems related to working conditions. Further, knowledge of occupational health help in protection from risk factors, and maintenance of healthy occupational environment at the workplace. The goal of occupational health in work place is health promotion, early diagnosis, treatment, specific protection, prevention of disabilities, and rehabilitation through epidemiological approaches, health screening, statistical evaluations and health education [2].
In the past, occupational health had a focus on industrial hygienic or industrial health of factories and mine workers only. Occupational health was not properly defined until 1700 A.D. due to various political and economic reasons. Italian physician Bernardino Ramazzini published a document (De Morbis Artificum Diatriba) taking into consideration of the health of the workers. In 1920s, Alice Hamilton a United States of America’s (USA) physician and his colleague a social reformer Jane Addams addressed occupational health as a subject of public health and preventive medicine [1]. In 1960s, Rachel Carson of the USA, a biologist, and ecologist talked about the impact of industrial pollution on public health in her book “Silent Spring” [3]. In the past 50 years, extraordinary developments in science, technology, legislation, public health, and social empowerment have led to much more progress in occupational health. The Royal Commission on health promotion and health wellbeing recommended improvement of occupational health of industrial workers which ultimately lead to economic development in India. There is provision of bonus for extra working hours of the workers. Further, provision of housing, health, and safety of the working population was made mandatory for the industries. In 1929 at the time of pre-independent India, only 39 inspectors were engaged in 8129 factories from 8 provinces to report working conditions and accidents of laborers [2]. In 1940, the labour investigation report showed that incidence of the accident was low at that time, but the health infrastructures were unable to provide adequate health care to the industrial workers [3].
During independence, the concept of occupational health was included in commercial establishments, mercantile enterprises, forestry, agriculture, and services sectors. The subject also focused on industrial hygiene, industrial accidents, industrial diseases, and toxicology related to industrial hazard, occupational psychology, and rehabilitation [4]. Occupational health focus on providing preventive measure rather than curative action. Additionally, it aims for the development of healthy and safe work environments in the organisations which leads to health and wellbeing of the working population. Overall, the objective of occupational health care management is to enhance the social and economic condition of the workers [5].
The objective of this paper is to study various factors like social status, job allocation, risk, hazard distribution, and wages differentiation pertaining to occupational health among the working population. The primary aims of the review is to identify and understand various theories and models of occupational health hazard.
Literature Search
Various search engines like PubMed, Scopus, web of sciences, and jstore has been explored to understand about the phenomena of occupational health. The details of phenomenon was arranged in various themes and sub-themes according to similarity. The factors like social status, job allocation, risk, hazard distribution, and wages differentiation were discussed from various sources to infer the theoretical model of study for the understanding of factors affecting occupational health. The existing occupational health hazard models have been discussed to understand the relation of work and health among the working population in the Indian context.
Discussion
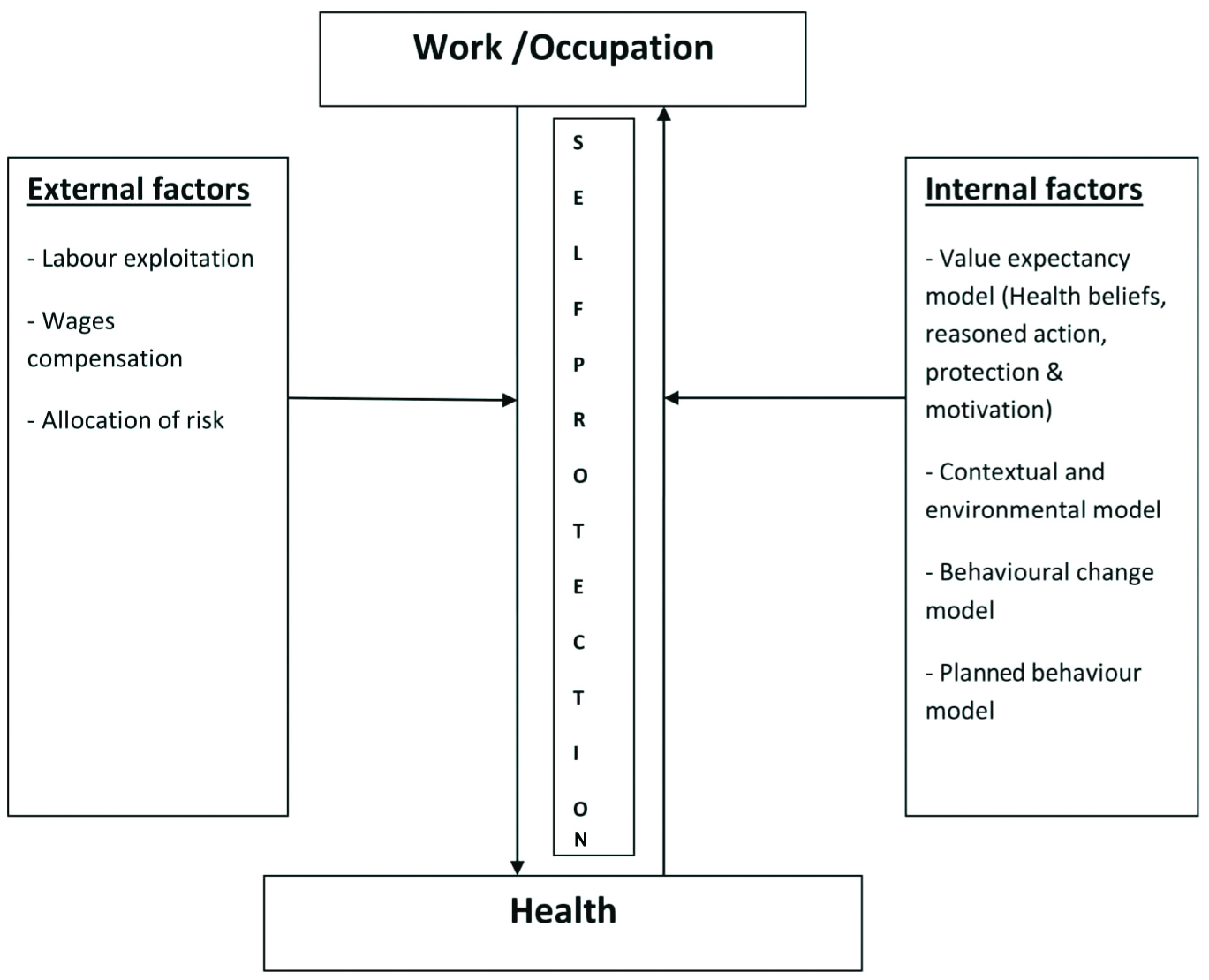
There are six models discussed in the paper on various aspects of occupational health. These models are based on the available research in the field of occupational health. The classification is done for understanding of the subject matters in an efficient way. The basis for classification is theoretical understanding of occupational health. These consists of theoretical model on occupational health behaviour, theoretical understanding on occupational health, contextual and environmental model, behaviour change model, Theory of planned behaviour (TPB) model, and Integrative framework on self-protective behaviour at workplace model. All these models and theories have a specific approach to understanding the occupational health in a different context. These models help in understanding occupational health and providing solutions specifically as per the need. The diagram in [Table/Fig-1] details the various theories and models. All these aspects discussed in elaborate manner in the following sections.
Theories and models of occupational health.
Source: Authors’ primary source
1. Theoretical Understanding of Occupational Health
There are many theories to understand occupational health in industrial set-ups. Labour exploitation theory on occupational health plays a role in understanding the concepts of how and why labor is important in solving various problems. The theory of Compensating Wage Differences (CWDs) explains the nuances of wage on the occupational health of the person in a similar set-up. Further, the theory of the allocation of risk in job markets understood by the nature of the job and factors influencing the situations at work place for occupational safety. The theories discussed with evidence in the following sections.
a. Labour exploitation theory on occupational health: According to Karl Marx, labor exploitation comes from the unfair distribution of wealth among workers. The exploitation stands on the asymmetric relationship of the power dynamic between employee and employer. The employers are unfairly and unethically taking advantage to exploit the workers. Power dynamic playing a greater role because of the inferior position of the employee and the authority provided to the exploiter. Unequal distribution of welfare in the labor force is a prominent factor of exploitation. The exploiter (employer) has the authority to command on goods and services. Employer also create revenue from the wages of the working class. Employers belong to the upper strata of society having the ownership of productive assets which dominate on the working class. So, the workers cannot enjoy their labor and redistribute wealth [6].
The theoretical perceptive shows working class used as tools of production irrespective of any health, safety and other benefits. The capitalists manipulates various aspects like workers’ desire, rights and welfare provisions. The magnitude of exploitation is high among unorganised workers in current scenario. The labour exploitation is an important factor which leads to the occupational health hazards among the working-class population.
b. Theory of Compensating Wage Differences (CWDs): In Paradigm, Adam Smith discussed CWDs and its relation to the occupational health of the working population. According to this theory, market offer the wage premiums to the working population which leads unequal wage distribution in the labor market. So, the labour forces are attracted by the highest package of wages, suppress their work preference without any workplace safety. The inferior working condition and multi-task performance raise cost of occupational health expenditure. Attention has not paid to the value of life. This theory perceives only the monetary value of the work force. Therefore, people are willing to accept jobs of a higher probability of fatal and non-fatal job accident [7].
A large number of studies found that jobs associated with harmful working conditions and a higher degree of fatal risk were among those workers getting a higher level of wage within the same occupation [8-12]. Many studies provided evidence that Chronic Wasting Diseases (CWD) has positively and statistically significant for fatal injuries [13,14]. Those who perform multi-tasks in work place were more exposed to occupational health risk, even the workers are classified within the same industry or performing the same occupation. The study also noted ignorance of non-fatal job risks for their extra compensation [12]. The concept is applicable to identify the higher risk group to occupational health hazards, and evidence found that income, as a key factor to influence the occupational health of the workers [10].
c. Distribution of risk in job markets: This approach shows the distribution of occupational risk based on the social stratification of workers. The workforce from lower social strata and less educational background are allocated to work with a harmful hazardous agent without providing any safety instruction. This approach also justifies the occupational group which gets the same risk during distribution of public provisions and compensation. Hence the incidence of occupational illness and accidents is higher among these occupations [15].
Inefficiencies of competitive market force do not provide adequate information about the relation between the employee and their workplace risk. Workers do not respond to their workplace risk rationally [16-18]. A survey found that the underestimation of the frequency of occupational risk is increasing among occupational illness [16]. Workers were unable to estimate the severity and nature of risk for their health and quality of life [19, 20]. The underestimation of risk is associated with ascertain occupation which promotes the chance of accidents and illness at work place. These kinds of miscalculation to the magnitude of risk, force the workers to work in a hazardous occupation.
2. Theoretical Model on Occupational Health Behaviour
A large number of models explained about people engaged in medical benefit and their health promotion. Details about preventive measures (exercise, vaccination, and safe sex and balanced diet), screening and detection (testing of blood pressure, genetic checking, and cholesterols check-up) and health seeking behaviour (utilisation of health services) has explained in various models. This model gives much more attention to workplace hazards and self-protective behaviour of the working population.
The perspective to health behaviour of the working population has been explained in various models. The decision making or cost-benefit model is derived from value expectancy theory [14,21]. The environmental or contextual model analyses to determine health behaviour of working population. The behaviour change model is an important approach which drives the health behaviour of the working population. Theory of planned behaviour is a paradigm which examines the path of beliefs and interpersonal behaviours. All the above models focused on the beliefs and perceptions related to the work and occupational threats, risk, and hazards [22].
a. Value expectancy model: This approach evaluates the seriousness of risk and hazards and estimates the cost and benefit of required action. The workers have right to take action which ultimately promote their expected outcome [23]. This model is motivated for self-protective behaviour to minimise the negative consequences. The motivation comes from the expected action which would reduce the magnitude of harms. The expected benefit from the particular action should be more than the expected cost. This model indicates the working population followed by protective measures within their estimated cost.
b. Health belief model: This is the most popular model used by various health research. This model perceives susceptibility and seriousness of health problem. The model also perceives the benefit and barrier of the associated action. Beliefs, self-efficacy, and response efficacy are related to the possibility of threats. The model assumes to the occurring threats of the working classes and also assumes expectations and barriers of the proposed action.
c. Theory of reasoned action: The theory focuses on behavioural intention and attitude of individual towards their risk and hazards. The theory also believes to evaluate the consequence of risk factors and intend to predict by beliefs and attitude. This model is applicable to change positive health behaviour and take preventive measures (exercise, weight loss and protective equipment) in the workplace [23-25].
d. Protection motivation theory: This theory is based on two processes such as threat appraisal and coping appraisal. Threat appraisal evaluates the pleasure principle to perceive the health vulnerability and outcome of severity. Coping appraisal evaluates the efficiency of preventive measure and assessment of successful action. The value expectancy models for workers’ health safety is a dynamic process to self-protective behaviour of the working population.
3. The Contextual and Environmental Model
This model shows that various health risk and threats influence the beliefs, attitude, and expectation of an individual. Attention is given to the environmental or social factors for betterment. The model argues that, environmental factor is the key aspect which would influence the health behaviour of the worker. Many studies argue that, the process of interaction among health and workplace safety, change the workers behaviour. This also changes work environment [26-28].
4. Behaviour Change Model
This model shows individual behaviour change towards their work-related hazards and how to take precaution. In every process of change, workers require different types of information for moving forward. The model is constructed on two processes, such as Trans-theoretical process [29] and Precaution adaptation process [14]. The details of the process is explained in [Table/Fig-2].
Behaviour Change Model.
Source: Authors’ primary source
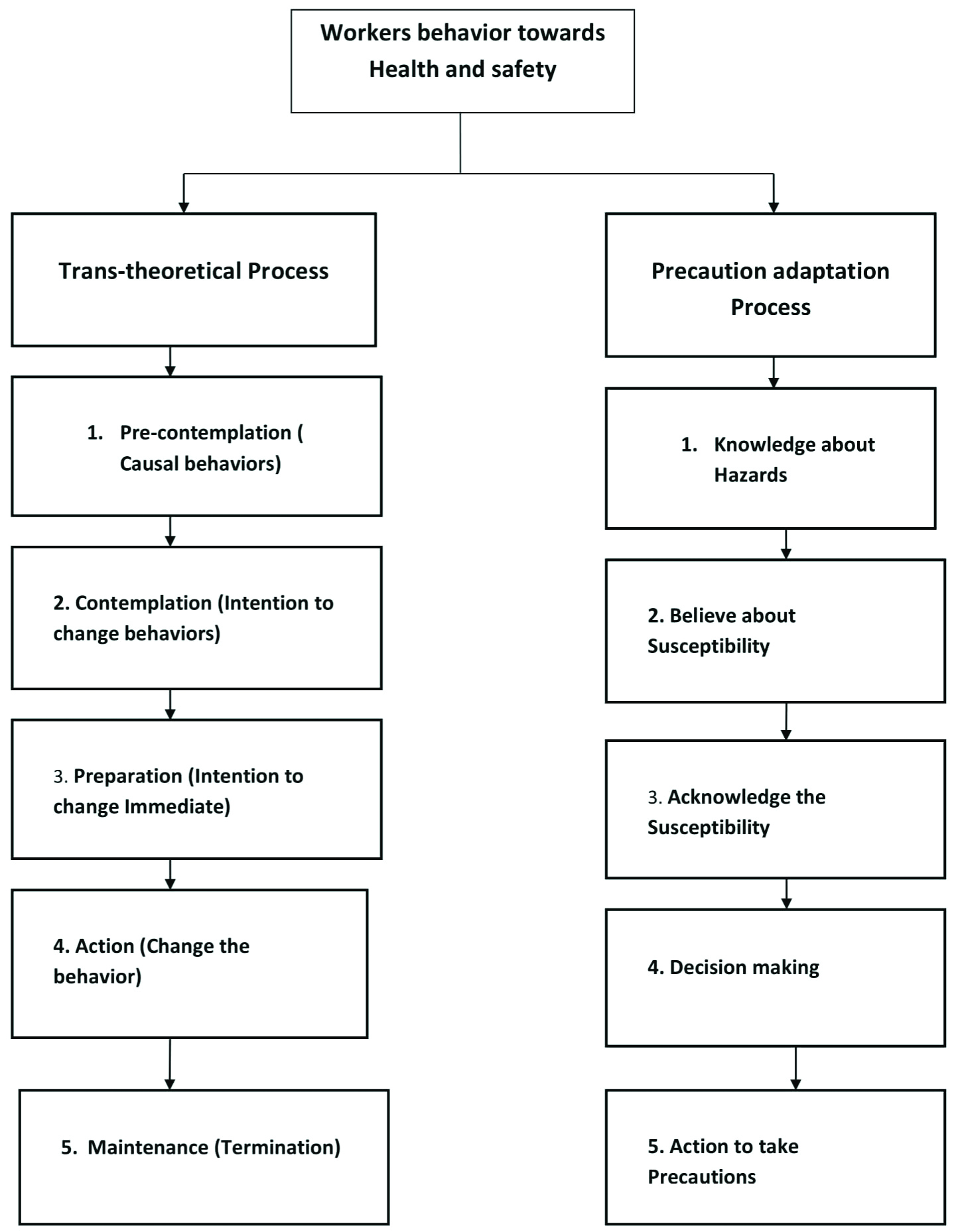
The trans-theoretical process consists of five stages such as pre-contemplation which is not thinking seriously about the change the behaviour. Second is contemplation, here the individual starts to think seriously about change their behaviour. Next is preparation where the individual intends to change as soon as possible. Lastly, this process denotes action and maintenance which followed initial behaviour change-up to termination.
The precaution adaptation process also deals with five stages. In the first stage, workers were well known about their workplace hazards, after that they believe about susceptibility with others. At the third stage, workers acknowledge their susceptibility. In the next stage, they decided to take precaution and lastly take precaution.
5. Theory of Planned Behaviour (TPB)
This model indicates that individual beliefs about their risk and hazards depend on their self behaviour. This model was constructed on the Attitude Towards Behaviour (ATB) where the cognitive and affective evaluation of the objectives was conducted. The descriptive and injective norms were evaluated by Subjective Norms (SN) in social environments. Perceived Behavioural Control (PBC) is the aspect of this model which has the autonomy to process the skills needed to required performances. All these components influence the Behavioural Intention (BI) of an individual and perform adequate intervention during occupational health hazards. Behavioural intentions are controlled by knowledge, skills, habits and some environmental factors [30]. TPB is linked to the theory of reasoned action which does not perceive the behavioural control [31]. Workplace safety is the positive predictor of safe behaviour to reducing occupational health hazards. This is predicting how the organisation, tools and equipment influence workplace safety. It also predicts the behaviour of fellow workers influencing the workplace safety [32-34]. Protective behaviour is necessary to identify adequate strategies for workplace safety [35,36]. The model describes safety climate, subjective norms, attitude and demographic predictors used for protective equipments [37].
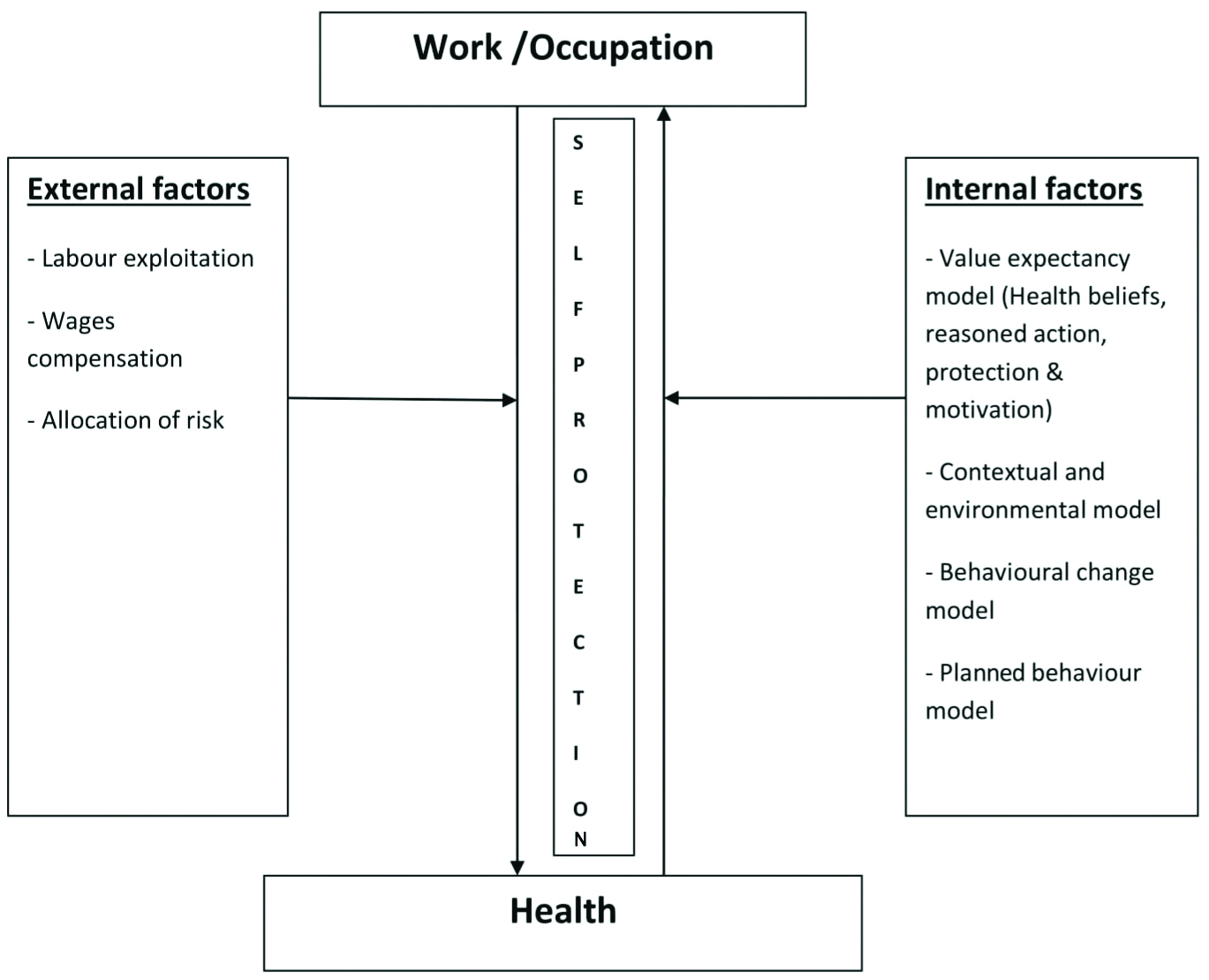
It is observed that workers are less interested in taking precaution unless they feel personally vulnerable. A study also found that individuals are optimistically biased to evaluate or judge their risk and hazards [38,39]. Information regarding work-related hazards increases awareness and personal susceptibility, which focus on skill development and promotes the self-efficacy of the workers. Further, this leads to taking action which can reduce possible barriers and positive self-protective behaviour of the working population. The details of conceptual understanding of theorising on work and health is given in [Table/Fig-3].
Conceptual understanding of theorising on work and health.
Source: Authors’ primary source
6. Integrative Framework on Self-protective Behaviour at the Workplace
According to the health belief theory and the recommended models workers behaviour on workplace safety are driven by four stages such as hazard appraisal, decision making, initiation, and adherence. Every stage carries different motivational factors to promote self-protective behaviour of workplace safety. The details of models of work place self-protective behaviour is given in [Table/Fig-4] [40].
Models of work place self-protective behaviour.
Source: David M. Dejoy, 1996 [40]
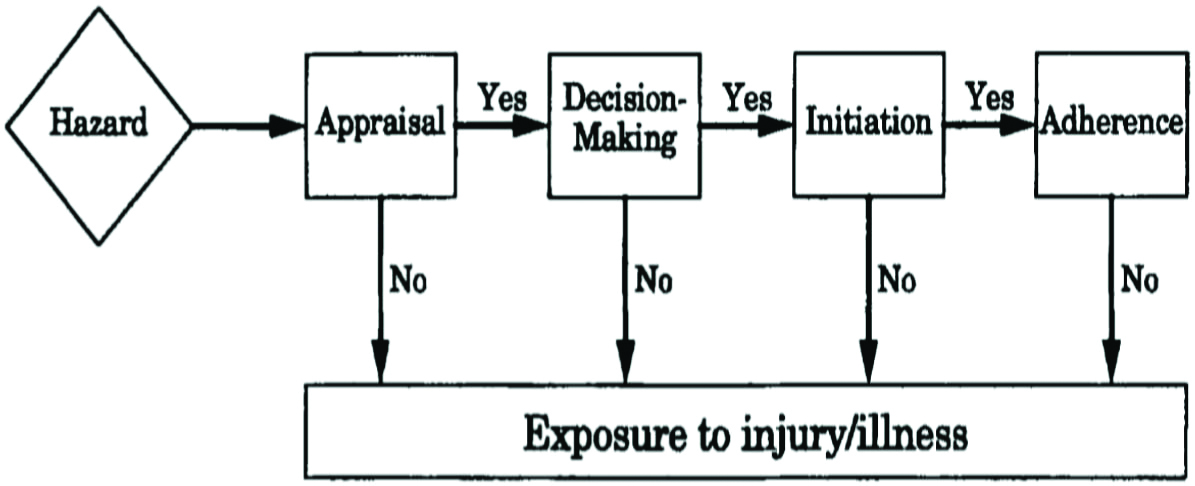
a. Hazard appraisal: Here the prime focus is given to a worker’s beliefs on workplace hazards and threats. Threats can be perceived from the interaction of susceptibility and severity of illness. Availability of preventive strategies and response of effectiveness for working population are defined here. Self-protective or defensive behaviour of worker results into release or reduction of hazards irrespective of any availability or unavailability of preventive measures [41]. Workers’ overconfidence also plays an important role in hazard appraisal [42]. Information regarding workplace hazards, mode of exposure, estimation of risk and preventive measures promote the benefits of working population.
b. Decision making: Self-efficacy and cost benefits on the course of action are associated with the decision making process of workers. It perceives the benefit of action for self-protection against the cost. The cost is considered as a reduction of productivity, skill performance, time constraints, physical discomfort and some other factors related to a reduction in the quality of life on their work. In this stage, condition of the workplace like availability of safety equipment, training for the proper utilisation of equipment and redesign of the job make more effective and self-protective for the working population. It is promoted to develop education, skill building exercise, and training programme among the working population which is considered to the safety climate [40].
c. Initiation: Condition of work and safety climate is the prime focus in this stage. Environmental and organisational factors are supported and reinforced to the self-protective actions which are very important factors to know the behavioural intention about workplace hazards. It indicates to the action and attitude for management of safety measures in work place [32,43,44].
d. Adherence: Organisational and environmental factors play a greater role in the sustainability of workplace adherence. Self-efficacy of workers should increase by successful actions. Self-efficacy and response efficacy increase more confidence among the working population.
An integrative framework of self-protective behaviour demonstrates that knowledge and awareness are important to change the behaviour about self-protective action among the working population. Hazard appraisal is focused on threats related beliefs and responses efficacy. So workers can identify both suspects and protective equipments. This influence the health and safety related decision making process. Finally, the environmental and organisational factors promote to sustain the behaviour associated with workplace safety.
The integrative frame work for self-protective behaviour would help to take the right decisions during the possibility and occurrence of occupational health hazards of the working population. Workers can measure the magnitude of risk and analyse the cost and benefit of required action. Interaction of exposure agents and occupational hazards can assume from this model. This approach brings an understanding of how the environment and organisation play a greater role to provide occupational health provision to the working population [40].
Conclusion
All the six models discussed in the paper provide a fair understanding of occupational health in the context of vulnerable industrial worker where factors like wage, work condition, position, human behaviour, environment, and provision of health care play an important role. The models provide evidence and scope for studying occupational health in different contexts in industrial settings. The theoretical understanding of occupational health helps in assessing the hazardous conditions of the workplace. All the theories help in studying and suggesting the improvement of various aspects.
[1]. WHO, 1950. What is Occupational health? Available at: http://www.agius.com/hew/resource/ohsilo.htm (accessed 20 January 2019) [Google Scholar]
[2]. Dastur HP, A doctor’s approach to industrial medicineTata Institute of Social Sciences 1960 [Google Scholar]
[3]. Mandal AK, Strategies and policies deteriorate occupational health situation in India: A review based on social determinant frameworkIndian Journal of Occupational and Environmental Medicine 2009 13(3):11310.4103/0019-5278.5891320442828 [Google Scholar] [CrossRef] [PubMed]
[4]. WHO (1970). World Health, United state department of labour, occupational safety and health administration, Available at: https://www.osha.gov/laws-regs/oshact/completeoshact (accessed 2 March 2018) [Google Scholar]
[5]. World Health Organization (2010) Regional Strategy on Occupational Health and Safety in SEAR Countries. Available at: http://www.searo.who.int (accessed 1 January 2017) [Google Scholar]
[6]. Cohen GA, The labor theory of value and the concept of exploitationPhilosophy & Public Affairs 1979 :338-60. [Google Scholar]
[7]. Smith A, An Inquiry into the Nature and Consequences of the Wealth of Nations [Google Scholar]
[8]. Smith MJ, Beringer DB, Human factors in occupational injury evaluation and control. In G. Salvendy (Ed.)Handbook of human factors 1987 Oxford, EnglandJohn Wiley & Sons:767-789. [Google Scholar]
[9]. Marin A, Psacharopoulos G, The reward for risk in the labor market: evidence from the United Kingdom and reconciliation with other studiesJournal of Political Economy 1982 90(4):827-53.10.1086/261094 [Google Scholar] [CrossRef]
[10]. McNabb R, Compensating wage differentials: Some evidence for BritainOxford Economic Papers 1989 41(1):327-38.10.1093/oxfordjournals.oep.a041898 [Google Scholar] [CrossRef]
[11]. Viscusi VK, The value of risks to life and healthJournal of Economic Literature 1999 31(4):1875-911. [Google Scholar]
[12]. Arabsheibani GR, Marin A, Stability of estimates of the compensation for dangerJournal of Risk and Uncertainty 2000 20(3):247-69.10.1023/A:1007819530588 [Google Scholar] [CrossRef]
[13]. Siebert WS, Wei X, Compensating wage differentials for workplace accidents: evidence for union and nonunion workers in the UKJournal of Risk and Uncertainty 1994 9(1):61-76.10.1007/BF01073403 [Google Scholar] [CrossRef]
[14]. Weinstein ND, Testing four competing theories of health-protective behaviorHealth Psychology 1993 12(4):32410.1037/0278-6133.12.4.324 [Google Scholar] [CrossRef]
[15]. Henderson J, What should be done about occupational accidents and diseases?International Journal of Epidemiology 1983 12(1):77-83.10.1093/ije/12.1.776840960 [Google Scholar] [CrossRef] [PubMed]
[16]. Kahneman D, Slovic SP, Slovic P, Tversky A, Judgment under uncertainty: Heuristics and biases 1982 Apr 30 Cambridge university press10.1017/CBO9780511809477 [Google Scholar] [CrossRef]
[17]. Slovic P, Monahan J, MacGregor DG, Violence risk assessment and risk communication: The effects of using actual cases, providing instruction, and employing probability versus frequency formatsLaw and Human Behavior 2000 24(3):271-96.10.1023/A:100559551994410846372 [Google Scholar] [CrossRef] [PubMed]
[18]. Kahneman D, Tversky A, Choices, values, and framesInHandbook of the Fundamentals of Financial Decision Making: Part I 2013 :269-278.10.1142/9789814417358_0016 [Google Scholar] [CrossRef]
[19]. Rogers AE, Addington-Hall JM, Abery AJ, McCoy AS, Bulpitt C, Coats AJ, Knowledge and communication difficulties for patients with chronic heart failure: qualitative studyBMJ 2000 321(7261):605-07.10.1136/bmj.321.7261.60510977838 [Google Scholar] [CrossRef] [PubMed]
[20]. Lloyd AJ, The extent of patients’ understanding of the risk of treatmentsBMJ Quality & Safety 2001 10(suppl 1):i14-18.10.1136/qhc.010001411533432 [Google Scholar] [CrossRef] [PubMed]
[21]. Glanz K, Rimer BK, Viswanath K, Health behavior and health education: theory, research, and practice 2008 Aug 28 John Wiley & Sons [Google Scholar]
[22]. Rogers RW, Cognitive and psychological processes in fear appeals and attitude change: A revised theory of protection motivationSocial Psychophysiology: A sourcebook 1983 :153-76. [Google Scholar]
[23]. Cleary P, Why people take precautions against health risks. I ND Weinstein (Ed.)Taking care: Understanding and encouraging self-protective behaviour:119-149.10.1017/CBO9780511527760.009 [Google Scholar] [CrossRef]
[24]. Kirscht JP, Preventive health behavior: A review of research and issuesHealth Psychology 1983 2(3):27710.1037/0278-6133.2.3.277 [Google Scholar] [CrossRef]
[25]. Sutton S, Social psychological Approaches to Understanding Addictive Behaviours: attitude behaviour and decision making modelsBritish Journal of Addiction 1987 82(4):355-70.10.1111/j.1360-0443.1987.tb01492.x3472583 [Google Scholar] [CrossRef] [PubMed]
[26]. DeJoy DM, Southern DJ, An integrative perspective on work-site health promotionJournal of Occupational Medicine.: Official Publication of the Industrial Medical Association 1993 35(12):1221-30. [Google Scholar]
[27]. Sheehy NP, Chapman AJ, Industrial accidents. In C. L. Cooper & I. T. Robertson (Eds.)International review of industrial and organizational psychology 1987 Oxford, EnglandJohn Wiley & Sons:201-227. [Google Scholar]
[28]. Green LW, Kreuter MW, Health promotion planning: an educational and environmental approach 1991 2nd ednMountain View, CaliforniaKreuter Mayfield Publishing [Google Scholar]
[29]. Prochaska JO, DiClemente CC, Transtheoretical therapy: Toward a more integrative model of changePsychotherapy: Theory, Research & Practice 1982 19(3):27610.1037/h0088437 [Google Scholar] [CrossRef]
[30]. Fishbein M, Ajzen I, Predicting and changing behavior: The reasoned action approachPsychology Press 2011 Feb 14 10.4324/9780203838020 [Google Scholar] [CrossRef]
[31]. Madden TJ, Ellen PS, Ajzen I, A comparison of the theory of planned behavior and the theory of reasoned actionPersonality and Social Psychology Bulletin 1992 18(1):03-09.10.1177/0146167292181001 [Google Scholar] [CrossRef]
[32]. Zohar D, Safety climate in industrial organizations: theoretical and applied implicationsJournal of Applied Psychology 1980 65(1):9610.1037/0021-9010.65.1.967364709 [Google Scholar] [CrossRef] [PubMed]
[33]. Moore D, Gamage B, Bryce E, Copes R, Yassi A, BC Interdisciplinary Respiratory Protection Study GroupProtecting health care workers from SARS and other respiratory pathogens: organizational and individual factors that affect adherence to infection control guidelinesAmerican Journal of Infection Control 2005 33(2):88-96.10.1016/j.ajic.2004.11.00315761408 [Google Scholar] [CrossRef] [PubMed]
[34]. Clarke S, The relationship between safety climate and safety performance: a meta-analytic reviewJournal of Occupational Health Psychology 2006 11(4):31510.1037/1076-8998.11.4.31517059296 [Google Scholar] [CrossRef] [PubMed]
[35]. Nilsson P, Andersson HI, Ejlertsson G, The Work Experience Measurement Scale (WEMS): A useful tool in workplace health promotionWork 2013 45(3):379-87.0.3233/WOR-12154123324702 [Google Scholar] [CrossRef] [PubMed]
[36]. Nilsson P, Development and quality analysis of the Work Experience Measurement Scale (WEMS)Work 2010 35(2):153-61.10.3233/WOR-2010-096720164610 [Google Scholar] [CrossRef] [PubMed]
[37]. Robertsen Ø, Siebler F, Eisemann M, Hegseth MN, Føreland S, Vangberg HC, Predictors of respiratory protective equipment use in the Norwegian Smelter Industry: The role of the theory of planned behavior, safety climate, and work experience in understanding protective behaviorFrontiers in Psychology 2018 910.3389/fpsyg.2018.0136630135666 [Google Scholar] [CrossRef] [PubMed]
[38]. Weinstein ND, Unrealistic optimism about susceptibility to health problemsJournal of Behavioral Medicine 1982 5(4):441-60.10.1007/BF008453727154065 [Google Scholar] [CrossRef] [PubMed]
[39]. Weinstein ND, Reducing unrealistic optimism about illness susceptibilityHealth Psychology 1983 2(1):1110.1037/0278-6133.2.1.11 [Google Scholar] [CrossRef]
[40]. DeJoy DM, Theoretical models of health behavior and workplace self-protective behaviorJournal of Safety Research 1996 27(2):61-72.10.1016/0022-4375(96)00007-2 [Google Scholar] [CrossRef]
[41]. Miller DT, Ross M, Self-serving biases in the attribution of causality: Fact or fiction?Psychological Bulletin 1975 82(2):21310.1037/h0076486 [Google Scholar] [CrossRef]
[42]. Weinstein ND, Unrealistic optimism about susceptibility to health problems: Conclusions from a community-wide sampleJournal of Behavioral Medicine 1987 10(5):481-500.10.1007/BF008461463430590 [Google Scholar] [CrossRef] [PubMed]
[43]. Brown RL, Holmes H, The use of a factor-analytic procedure for assessing the validity of an employee safety climate modelAccident Analysis & Prevention 1986 18(6):455-70.10.1016/0001-4575(86)90019-9 [Google Scholar] [CrossRef]
[44]. Dedobbeleer N, Béland F, A safety climate measure for construction sitesJournal of Safety Research 1991 22(2):97-103.10.1016/0022-4375(91)90017-P [Google Scholar] [CrossRef]