Journey from Fighters to Survivors: Quality of Life and Mental Status in Cancer Patients in a Rural Tertiary Care Hospital
Raza Shaheed1, Samarth Shukla2, Sourya Acharya3, Uplabdh Gopal4, Neema Acharya5
1 Student, Department of Medicine, Jawaharlal Nehru Medical College, Wardha, Maharshtra, India.
2 Professor, Department of Pathology, Jawaharlal Nehru Medical College, Wardha, Maharshtra, India.
3 Professor, Department of Medicine, Jawaharlal Nehru Medical College, Wardha, Maharshtra, India.
4 Student, Department of Medicine, Jawaharlal Nehru Medical College, Wardha, Maharshtra, India.
5 Professor, Department of Obstetrics and Gynaecology, Jawaharlal Nehru Medical College, Wardha, Maharshtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Mr. Raza Shaheed, T-2, Shivaji Boy’s Hostel, DMIMS (DU), Jawaharlal Nehru Medical College, Wardha, Maharashtra, India.
E-mail: razashahid27196@gmail.com
Introduction
Cancer is a major public health burden in India. Though modern medicine has made tremendous advancements in the treatment of cancers, still morbidity and mortality remain high. It affects different domains of Quality of Life (QOL). So apart from the conventional treatment protocols, cancer care seems to be the corner stone to reduce patient morbidity and ultimately prolonging survival.
Aim
To assess QOL and mental status in cancer patients undergoing treatment.
Materials and Methods
Patients diagnosed with cancer and undergoing treatment and patients attending the oncology clinics for follow-up after receiving chemo or radiotherapy during January 2019 to March 2019 were studied. The scores of WHOQOL-BREF and WEMWBS questionnaires were evaluated. Pearson’s Correlation Coefficient was applied to determine different domains of WHOQOL-BREFwith WEMWBS. Reliability analysis of WHOQOL-BREF and WEMWBS by Cronbach Alpha. Regression analysis of different Domain of WHOQOL-BREF with age, gender and WEMWBS.
Results
A total of 42 patients were enrolled in the study. The correlation between WHOQOL-BREF and WEMWBS was found to be significant. Physical health was significantly (p-value <0.05) associated with psychological, social relationship and environmental domain. Psychological domain was significantly (p-value <0.05) associated with physical health and environment domain. Social relationship was significantly (p-value <0.05) associated with physical health only. Environment was significantly (p-value <0.05) associated with physical health and psychological domain. Internal consistency of WHOQOL-BREF and WEMWBS were acceptable . Regression analysis of Physical health=8.090+0.205*WEMWBS. Regression analysis of Psychological domain=1.020+0.317*WEMWBS.
Conclusion
Awareness amongst the patients diagnosed with cancer is very important. Special emphasis should be given to improve the QOL and overall well-being of cancer patients apart from the normal treatment protocols.
Cancer care, Chemotherapy, Radiotherapy
Introduction
Cancer seems to be one of most dreaded ailments worldwide which one can manifest and despite immense advancements in cancer therapeutics, cancer related morbidity and mortality remains high [1]. It is the second leading cause of mortality, with an estimated 9.6 million deaths globally in 2018 and about 1 in 6 deaths is due to cancer [2]. Cancers are of diverse origin, involving almost all possible organ systems. An estimated 18.1 million new cases were diagnosed in 2018 [3]. The cancer burden in India is on rise. The prevalence of cancer in India is estimated to be around 2.0 to 2.5 million, with over 7-8 lac new cases detected every year and 4-5 lakh cancer deaths per year [4]. So it is imperative to improve cancer care strategies thereby helping to reduce patient morbidity and ultimately prolonging survival.
Cancer is a burden not only for the patient but also for the entire family. Cancer may have many effects on different domains of QOL in such individuals [5]. Cancer care seems to be the corner stone for fighting the dreaded pathology.
WHO Quality of Life-BREF (WHOQOL-BREF) is an assessment method which takes into consideration, the physical, environmental, psychological and social effects of patients suffering from chronic illness and its treatment [6,7]. The WHOQOL-BREF questionnaire contains two items from the Overall QOL and General Health and 24 items of satisfaction divided into four domains; Domain 1: deals with physical health and has 7 questions, Domain 2: deals with psychological health and has 6 questions, Domain 3: deals with social relationships and has 3 questions and Domain 4: deals with environmental health and has 8 questions. Cancer patients suffer from various detrimental symptoms during and after their treatment. QOL assessment gives a comprehensible paradigm of the cancer patients QOL as they go through various treatment modalities. So, it is important to evaluate QOL in cancer patients [8-10].
The psychological issues that are associated with the treatment of cancer patients are complex. Patients experience various negative emotions in form of anger, fear, pain, stress, uncertainty about life impending doom of the diagnosis that adversely affect their day-today living. Chemotherapy itself can cause various physical and psychological problems that negatively affects patients QOL [11-13]. Some of the patients attempt to relieve these stresses by developing risky behaviours like smoking or drinking alcohol and some become more sedentary with poorer QOL. Patients who effectively cope with these negative psychological aspects with relaxation and stress management techniques usually have lower levels of depression, anxiety and adverse symptoms related to cancer and its treatment [14].
Early intervention that focuses to prevent major psychological distress is necessary. New researches have shown substantial evidence indicating that psychological stress influences the incidence and progression of cancers through different mechanisms, like stimulating the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis leading to release of multiple stress related mediators that acts as immunosuppressants or mitogens in the tumour micro environment [15-18]. The ultimate effects of psychological stress on cancer cells activate the intracellular proliferative and migratory signalling pathways helping in progression of the tumour cells [15].
Warwick-Edinburg Mental Well Being Scale (WEMWBS) measures mental health in population. This scale contains 14 items which are answered on a 1-5 Likert scale. The total score ranges from 14-70. Higher scores represent higher mental well-being [19].
This study was undertaken to evaluate the QOL by WHOQOL-BREF and mental status by WEMWBS of cancer patients undergoing treatment in a rural tertiary care hospital. The different domains of WHOQOL-BREF were compared with age, gender and WEMWBS.
Materials and Methods
This observational cross-sectional study was carried out from January 2019 to March 2019 in DMIMS University, AVBR Hospital in Wardha district of central India. It included 42 patients suffering from various cancers in different stages undergoing treatment and giving written informed consent.
Institutional Ethics Committee (IEC) approval (Ref. No. DMIMS (DU)/IEC/2018-2019/7153) was taken before starting of the study.
Inclusion Criteria
Patients diagnosed with various malignancies undergoing treatment.
Exclusion Criteria
Defaulter patients of chemotherapy.
Patients with recurrence of cancer.
Patients with psychiatric illnesses.
Terminally ill cancer patients.
Patients not giving consent.
After taking due permission all patients were interviewed. The diagnosis, form of treatment received were noted. Then patients were asked to fill-up the WHOQOL-BREF and WEMWBS questionnaires which was translated and validated by a translator in the local language (Marathi and Hindi) then the questionnaire was again back-translated into English by another language expert who was not aware of the original version. Then the back-translated version was compared with the original by another language expert and also by a psychiatrist for conceptual equivalence of each item in the WHOQOL-BREF and WEMWBS (α=0.85). Then the scores were evaluated.
Statistical Analysis
Data analysis was carried by Statistical Package SPSS (version 25.0, IBM Corporation) and Microsoft Excel 2016. Descriptive statistics was described in proportions and frequencies. Quantitative data was presented as mean and standard deviation. Pearson’s correlation was done to find the correlation between two quantitative data. A p-value of <0.05 was considered statistically significant.
Results
A total of 42 cancer patients were included in the study. There were 24 males (57.14%) and 18 females (42.85%) The most commonly reported malignancy was breast cancer (35.71%). Patients were in different stage of malignancy and were undergoing chemo or radiotherapy [Table/Fig-1].
Showing baseline characteristics of the study participants.
| Variables | Categories | Breast (n=15) | Colorectal (n=9) | Prostate (n=3) | Stomach (n=5) | Oral (n=10) |
|---|
| Age (years) | Less than 55 years | 12 | 3 | 1 | 2 | 7 |
| ≥55 years | 03 | 6 | 2 | 3 | 3 |
| Gender | Male (n=24) | 0 | 8 | 3 | 4 | 9 |
| Female (n=18) | 15 | 1 | 0 | 1 | 1 |
| Stage of cancer | | Stage-II (n=9) | Stage-II (n=3) | Stage-II (n=2) | Stage-II (n=3) | Stage-I (n=4) |
| Stage-III (n=6) | Stage-III (n=6) | Stage-III (n=1) | Stage-III (n=2) | Stage-II (n=6) |
| Chemotherapy | Yes | n=15 | n=9 | n=3 | n=5 | n=6 |
| No | 0 | 0 | 0 | 0 | n=4 |
| Radiotherapy | Yes | 0 | n=2 (Ca Rectum) | n=3 | 0 | n=6 |
| No | 0 | | 0 | 0 | 0 |
| WHOQOL-BREF | Mean | 26.57 | 27.93 | 28.91 | 24.19 | 25.49 |
| SD | 3.12 | 2.59 | 3.01 | 2.49 | 2.41 |
| WEMWBS | Mean | 23.87 | 26.11 | 25.61 | 21.75 | 22.01 |
| SD | 2.51 | 2.01 | 3.05 | 2.46 | 2.37 |
Mean score of Domains of WHOQOL-BREF were computed which showed highest score for environmental domain and lowest for social domain. So social domain was affected more in comparison to other domains [Table/Fig-2]. Significant Pearson’s correlation coefficient between different domains of WHOQOL-BREF was observed, where it was observed that Physical health domain showed significant correlation with psychological, social relationship and environment domains. Psychological domain showed significant correlation with physical health and environment domains. Social relationship domain showed significant correlation with physical health only. Environment domain showed significant correlation with physical health and psychological domain [Table/Fig-3]. A significant positive correlation was observed between WHOQOL-BREF and WEMWBS [Table/Fig-4,5] i.e., with increase in QOL, mental well-being was improved. It indicates that patients with better QOL had better mental well-being. Internal consistency reliability of WHOQOL-BREF and WEMWBS was highly reliable [Table/Fig-6]. In Multiple regression analysis keeping physical domain of WHOQOL-BREF as the dependent variable, WEMWBS score was found to be positively associated with physical health (Physical Health=8.090+0.205*WEMWBS) [Table/Fig-7]. In other Multiple regression analysis keeping psychological domain of WHOQOL-BREF as the dependent variable, WEMWBS score was found to be positively associated with psychological health (Psychological=1.020+0.317*WEMWBS) [Table/Fig-8].
Descriptive statistics of domains of WHOQOL-BREF.
| Domain | Mean | Std. Deviation |
|---|
| Physical health | 19.40 | 3.80 |
| Psychological | 19.80 | 4.66 |
| Social relationship | 10.00 | 1.57 |
| Environment | 26.97 | 2.82 |
Pearson’s correlation coefficient between various domains of WHOQOL-BREF.
| Physical health | Psychological | Social relationship | Environment |
|---|
| Physical health | r-value | | 0.722** | 0.464** | 0.499** |
| p-value | | 0.0001, S | 0.002, S | 0.001, S |
| N | 42 | 42 | 42 | 42 |
| Psychological | r-value | 0.722** | | 0.222 | 0.374* |
| p-value | 0.0001, S | | 0.157, NS | 0.015, S |
| N | 42 | 42 | 42 | 42 |
| Social relationship | r-value | 0.464** | 0.222 | | 0.137 |
| p-value | 0.002, S | 0.157, NS | | 0.387, NS |
| N | 42 | 42 | 42 | 42 |
| Environment | r-value | 0.499** | 0.374* | 0.137 | |
| p-value | 0.001, S | 0.015, S | 0.387, NS | |
| N | 42 | 42 | 42 | 42 |
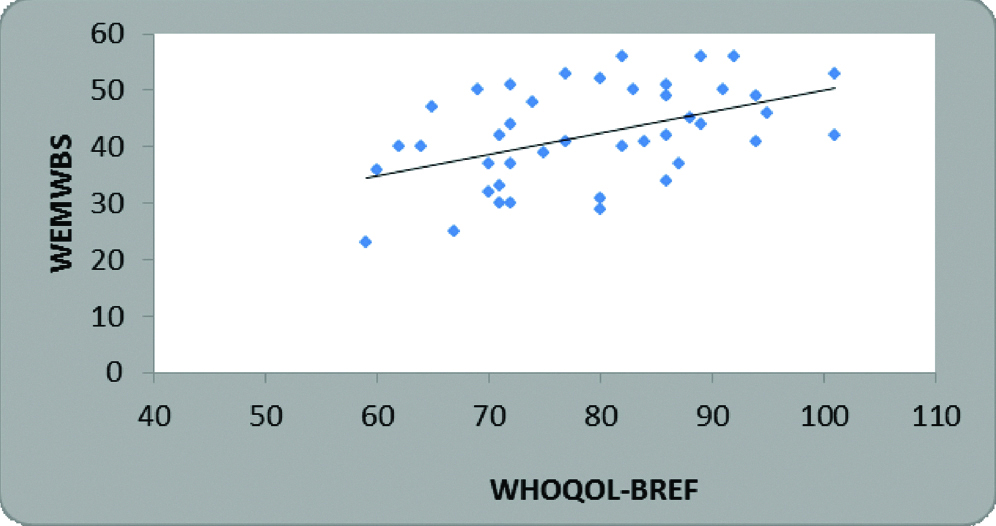
Correlation between WHOQOL-BREF and WEMWBS.
| Mean | Std. Deviation | N | Correlation ‘r’ | p-value |
|---|
| WHOQOL-BREF | 79.19 | 10.93 | 42 | 0.474 | 0.002, S |
| WEMWBS | 42.19 | 8.67 | 42 |
Pearson’s correlation coefficient
Scatter plot showing positive correlation between WHOQOL-BREF and WEMWBS.
Reliability analysis of WHOQOL-BREF and WEMWBS.
| Cronbach alpha | p-value |
|---|
| WHOQOL | 0.859 | 0.0001, S |
| WEMWBS | 0.897 | 0.0001, S |
Regression analysis of physical domain with age, gender and WEMWBS.
| Model | Unstandardized coefficients | Standardised coefficients | t | p-value |
|---|
| B | Std. Error | Beta |
|---|
| Physical health | 8.090 | 4.159 | | | |
| Age | 0.089 | 0.046 | 0.280 | 1.955 | 0.058, NS |
| Gender | -0.646 | 1.079 | -0.086 | 0.599 | 0.553, NS |
| WEMWBS | 0.205 | 0.063 | 0.467 | 3.228 | 0.003, S |
Regression analysis of psychological domain with age, gender and WEMWBS.
| Model | Unstandardized coefficients | Standardised coefficients | t | p-value |
|---|
| B | Std. Error | Beta |
|---|
| Psychological | 1.020 | 3.989 | | | |
| Age | 0.023 | 0.044 | 0.066 | 0.524 | 0.603, NS |
| Gender | 1.196 | 1.035 | 0.146 | 1.155 | 0.255, NS |
| WEMWBS | 0.317 | 0.061 | 0.665 | 5.205 | 0.0001, S |
Discussion
The present study showed significant correlation of all the domains of WHOQOL-BREF. A similar study conducted on 197 patients in Japan showed similar results, indicating self-care and self-rated health predicts QOL in cancer patients [20]. In our study the highest score of WHOQOL-BREF was of environmental domain and the lowest score was of social relationship, emphasising the importance of positive inter-personal relationship, positive emotional stability as an important parameter for positive well-being [21].
In a study by Morris J et al., 80% of the health care professionals believed in authenticity of WHOQOL assessment but, interestingly only 50% of the health care providers applied it in clinical practice [22]. Implementation of QOL along with the treatment protocols also improves the communication between treating physicians and patients [21].
In the present study multiple regression analysis showed that physical health and psychological health was positively affected by WEMWBS suggesting that mental health affects the physical and social domains of cancer patients, a similar observation was made by another study [23]. A study that included patients of colorectal cancer found that the environmental domain was most commonly affected and psychological domain was least affected [24].
The physical domain consists of the energy level, ability to perform daily activities, fatigability and lastly pain and mobility. All these factors are interrelated. In our study physical domain was positively correlated with psychological, environmental and social relationship. This signifies the importance of inculcating healthy interpersonal and environmental changes in the life of cancer patients. Various studies were done to determine QOL and Mental well-being in cancer patients with results similar to the current study [Table/Fig-9] [20,21,25-30].
Showing results of various studies as compared with the present study [20,21,25-30].
| Tazaki M et al., [20] | High correlation between the psychological and the environmental domains (r=0.7021), the physical domain and the level of independence (r=0.6031) and social relations and the environment (r=0.6856) and QOL scores. |
| Pooja RS et al., [21] | Positive correlation was observed between duration of treatment and social domain. |
| Rabin EG et al., [25] | In the psychological and social relationship domains, only depression stood out as significant (p=0.009 and p=0.006, respectively). For the other domains, no variable appeared to be statistically significant. |
| Yen JY et al., [26] | Quality of life, depression and stress were compared between the malignant and benign groups, and the factors related to QoL were also examined. It was found that the malignant group had poorer physical and psychological QoL and higher life stress. |
| de Mol M et al., [27] | All domains demonstrated good internal consistency (α>0.70), except Social Relationships (α=0.57). Nineteen of the 24 WHOQOL-BREF items had correlations of ≥0.40 with their intended domain. |
| Shakeri J et al., [28] | Cancer patients being male, single, having higher salary and education, and lower age are related to higher QOL. Furthermore, in general, QOL of cancer patients was positively correlated with avoidant coping style (p<0.05, r: 0.170) and negatively associated with emotion-focused coping styles (p<0.01, r: −0.378). |
| Lin CY et al., [29] | The mean WHOQOL-BREF domain scores were between 13.34 and 14.77. |
| Mansano-Schlosser TC et al., [30] | The psychological domain reached the highest scores, unlike the others, who evaluated the environmental domain as best. The results suggest that health self-assessment can be a reliable predictor of quality of life in these patients. |
In this study, it was observed that QOL in cancer patients should be addressed at an individual level because a negative QOL imparts negative results on the patients physical, social, psychological and environmental factors.
Limitation
This study was taken up as a short-term student research program, so the duration was limited. The sample size of study was small because of the limited duration. Only limited type of malignancies could be included because it was a prospective study and patients were recruited according to their hospital visits and treatment schedules. The mental status and QOL was studied during the treatment phase only.
Conclusion
Awareness amongst the patients diagnosed with cancer is very important. Special emphasis should be given to improve the QOL and overall well-being of cancer patients apart from the normal treatment protocols. Physicians, Oncologists and the care givers should be concerned about mental well-being of cancer patients, as they go through pain, anxiety, mood despair, depression, etc. In this study physical health and psychological health was positively affected by mental well-being. Our study showed significant correlation of all the domains of WHOQOL-BREF emphasising importance of positive inter-personal relationship, positive emotional stability as an important parameter for positive well-being.
Pearson’s correlation coefficient
[1]. Dehkordi A, Heydarnejad MS, Fatehi D, Quality of life in cancer patients undergoing chemotherapyOman Med J 2009 24:204-07.10.5001/omj.2009.4022224186 [Google Scholar] [CrossRef] [PubMed]
[2]. Cancer. Fact sheet. [Internet] World Health Organization [revised 2018 Sep 12; reviewed 2018 Sep 12; cited 2019 Jan 12]; [about 10 screens]. Available from: https://www.who.int/news-room/fact-sheets/detail/cancer [Google Scholar]
[3]. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A, Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countriesCA Cancer J Clin 2018 68(6):394-24.10.3322/caac.2149230207593 [Google Scholar] [CrossRef] [PubMed]
[4]. Project Proposal September State Health Systems Resource Centre National Rural Health Mission. Department of Health and Family Welfare, Government of Punjab. 2012. Available from: pbhealth.gov.in/Final State Proposal.pdf [Google Scholar]
[5]. Roiland RA, Heidrich SM, Symptom clusters and quality of life in older adult breast cancer survivorsOncol Nurs Forum 2011 38:672-80.10.1188/11.ONF.672-68022037330 [Google Scholar] [CrossRef] [PubMed]
[6]. Taechaboonsermsak P, Kaewkungwal J, Singhasivanon P, Fungladda W, Wilailak S, Causal relationship between health promoting behavior and quality of life in cervical cancer patients undergoing radiotherapySoutheast Asian J Trop Med Public Health 2005 36:1568-75. [Google Scholar]
[7]. Guyatt G, Feeny DH, Patrick DL, Measuring health related quality of lifeAnn Inter Med 1993 118:622-29.10.7326/0003-4819-118-8-199304150-000098452328 [Google Scholar] [CrossRef] [PubMed]
[8]. MS Heydarnejad, Dehkordi A Hassanpour, Dehkordi K Solati, Factors affecting quality of life in cancer patients undergoing chemotherapyAfr Health Sci 2011 11(2):266-70. [Google Scholar]
[9]. Wilson IB, Cleary PD, Linking clinical variables with health-related quality of life. A conceptual model of patient outcomesJ Am Med Ass 1995 273:59-65.10.1001/jama.1995.03520250075037 [Google Scholar] [CrossRef]
[10]. Spilker B, Quality of Life and Pharmacoeconomics in Clinical Trials 1996 PhiladelphiaLippincott-Raven [Google Scholar]
[11]. Wen KY, Gustafson DH, Needs assessment for cancer patients and their familiesHealth and Quality of Life Outcomes 2004 2(1):1110.1186/1477-7525-2-1114987334 [Google Scholar] [CrossRef] [PubMed]
[12]. Sharpe L, Butow P, Smith C, McConnell D, Clarke S, Changes in quality of life in patients with advanced cancer: Evidence of response shift and response restrictionJournal of Psychosomatic Research 2005 58:497-504.10.1016/j.jpsychores.2005.02.01716125516 [Google Scholar] [CrossRef] [PubMed]
[13]. Ganz PA, Quality of life measures in cancer chemotherapy: Methodology and implicationsPharmacoeconomics 1994 5:376-88.10.2165/00019053-199405050-0000410147229 [Google Scholar] [CrossRef] [PubMed]
[14]. Artherholt SB, Fann JR, Psychosocial care in cancerCurrent Psychiatry Reports 2012 14(1):23-29.10.1007/s11920-011-0246-722068509 [Google Scholar] [CrossRef] [PubMed]
[15]. Yuan A, Wang S, Li Z, Huang C, Psychological aspect of cancer: From stressor to cancer progressionExp Ther Med 2010 1(1):13-18.10.3892/etm_0000000323136586 [Google Scholar] [CrossRef] [PubMed]
[16]. Garssen B, Psychological factors and cancer development: Evidence after 30 years of researchClin Psychol Rev 2004 24:315-38.10.1016/j.cpr.2004.01.00215245834 [Google Scholar] [CrossRef] [PubMed]
[17]. Chida Y, Hamer M, Wardle J, Steptoe A, Do stress-related psychosocial factors contribute to cancer incidence and survival?Nat Clin Pract Oncol 2008 5:466-75.10.1038/ncponc113418493231 [Google Scholar] [CrossRef] [PubMed]
[18]. Sood AK, Bhatty R, Kamat AA, Landen CN, Han L, Thaker PH, Stress hormone-mediated invasion of ovarian cancer cellsClin Cancer Res 2006 12:3697510.1158/1078-0432.CCR-05-169816428474 [Google Scholar] [CrossRef] [PubMed]
[19]. Tennant R, Hiller L, Fishwick R, Platt S, Joseph S, Weich S, The Warwick-Edinburgh mental well-being scale (WEMWBS): Development and UK validationHealth and Quality of life Outcomes 2007 5(1):6310.1186/1477-7525-5-6318042300 [Google Scholar] [CrossRef] [PubMed]
[20]. Tazaki M, Nakane Y, Endo T, Kakikawa F, Kano K, Kawano H, Results of a qualitative and field study using the WHOQOL instrument for cancer patientsJapanese J Clin Oncol 1997 28(2):134-41.10.1093/jjco/28.2.1349544830 [Google Scholar] [CrossRef] [PubMed]
[21]. Pooja RS, Mahesh V, Muninarayana C, Anil NS, Quality of life assessment among cancer patients undergoing treatment in a rural tertiary care centerJournal of Preventive Medicine and Holistic Health 2016 2(2):36-40. [Google Scholar]
[22]. Morris J, Perez D, McNoe B, The use of quality of life data in clinical practiceQual Life Res 1998 7:85-91.10.1023/A:10088930070689481154 [Google Scholar] [CrossRef] [PubMed]
[23]. Jacobsen PB, Davis K, Cella D, Assessing quality of life in research and clinical practiceOncology (Williston Park) 2002 16:133-39. [Google Scholar]
[24]. Michelone APC, Santos VLCG, Quality of life of cancer patients with and without a colostomyRev Latino-am Enfermagem 2004 12(6):34-47.10.1590/S0104-1169200400060000515678213 [Google Scholar] [CrossRef] [PubMed]
[25]. Rabin EG, Heldt E, Hirakata VN, Bittelbrunn AC, Chachamovich E, Fleck MP, Depression and perceptions of quality of life of breast cancer survivors and their male partnersIn Oncol Nurs Forum 2009 36(3):153-58.10.1188/09.ONF.E153-E15819403443 [Google Scholar] [CrossRef] [PubMed]
[26]. Yen JY, Ko CH, Yen CF, Yang MJ, Wu CY, Juan CH, Quality of life, depression, and stress in breast cancer women outpatients receiving active therapy in TaiwanPsychiatry and Clinical Neurosciences 2006 60(2):147-53.10.1111/j.1440-1819.2006.01479.x16594937 [Google Scholar] [CrossRef] [PubMed]
[27]. de Mol M, Visser S, Aerts JG, Lodder P, de Vries J, den Oudsten BL, Satisfactory results of a psychometric analysis and calculation of minimal clinically important differences of the World Health Organization quality of life-BREF questionnaire in an observational cohort study with lung cancer and mesothelioma patientsBMC Cancer 2018 18(1):117310.1186/s12885-018-4793-830477456 [Google Scholar] [CrossRef] [PubMed]
[28]. Shakeri J, Kamangar M, Ebrahimi E, Aznab M, Shakeri H, Arman F, Association of coping styles with quality of life in cancer patientsIndian Journal of Palliative Care 2015 21(3):29810.4103/0973-1075.16489026600698 [Google Scholar] [CrossRef] [PubMed]
[29]. Lin CY, Hwang JS, Wang WC, Lai WW, Su WC, Wu TY, Psychometric evaluation of the WHOQOL-BREF, Taiwan version, across five kinds of Taiwanese cancer survivors: Rasch analysis and confirmatory factor analysisJournal of the Formosan Medical Association 2019 118(1):215-22.10.1016/j.jfma.2018.03.01829661488 [Google Scholar] [CrossRef] [PubMed]
[30]. Mansano-Schlosser TC, Ceolim MF, Quality of life of cancer patients during the chemotherapy periodTexto & Contexto-Enfermagem 2012 21(3):600-07.10.1590/S0104-07072012000300015 [Google Scholar] [CrossRef]