Correlation between Frequency of Flaps in Asterixis and Severity of the Liver Disease in Patients with Hepatic Encephalopathy
Piyush Kumar Thakur1, Vinod Kumar Dixit2, Sunit Kumar Shukla3, Ravikant Thakur4, Tuhin Mitra5, Dawesh Prakash Yadav6
1 Senior Resident, Department of Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
2 Professor, Department of Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
3 Associate Professor, Department of Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
4 Senior Resident, Department of Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
5 Senior Resident, Department of Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
6 Assistant Professor, Department of Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Dawesh Prakash Yadav, Assistant Professor, Department of Gastroenterology, Institute of Medical Sciences, Banaras Hindu University, Varanasi-221005, Uttar Pradesh, India.
E-mail: devesh.thedoc@gmail.com
Introduction
Frequency of flaps in asterixis is not uniform and varies among the patients. However, this flap frequency has not been given much importance in the literature. Neither it alters the grade of severity of Hepatic Encephalopathy (HE), nor has it been included in any of the scoring systems determining the severity of liver disease such as the Child Turcotte Pugh (CTP) and Model for End stage Liver Disease (MELD) scores.
Aim
To study the correlation between frequency of flaps in asterixis and severity of the liver disease in patients with HE.
Materials and Methods
Patients with decompensated cirrhosis and HE with asterixis had their flap frequency (per 30 seconds) counted at the time of their discharge, after clinical stabilisation. CTP and MELD scores were also calculated and the correlation between number of flaps and CTP and MELD scores was studied. A total of 63 such patients were followed up for a period of 12 months. We also studied whether patients with increasing number of flaps have a poorer clinical outcome, as suggested by re-hospitalisation.
Results
The correlation between number of flaps and CTP score was non-significant (rs=0.02, p=0.87). Correlation between number of flaps and MELD score was also non-significant (rs=0.16, p=0.20). A 13% of patients with <5 flaps/30s were subsequently re-hospitalised for both hepatic and non-hepatic causes as compared to 64% of patients with >15 flaps/30s. A total of 27 patients were re-hospitalised out of which 12 (44.4%) had worsening HE, 5 (18.5%) had Spontaneous Bacterial Peritonitis (SBP) and worsening HE, 6 (22.2%) had worsening ascites and 4 (14.8%) had acute kidney injury.
Conclusion
There was no significant correlation between number of flaps and CTP and MELD scores. However, higher number of flaps was an independent predictor for re-hospitalisation.
Child turcotte pugh, Cirrhosis, Model for end stage liver disease
Introduction
Asterixis is widely used by the clinicians to diagnose HE. Usually seen in HE, it can also be seen in other metabolic encephalopathies too. Though the frequency of flaps in asterixis is not uniform and varies among the patients, this flap frequency has not been given much importance in the literature. HE has been classified into types A, B, C depending on whether it is associated with acute liver failure, porto systemic bypass or cirrhosis [1]. Severity of HE is graded according to West Haven and ISHEN (International Society for Hepatic Encephalopathy) grading system [1]. However, the frequency of flaps neither alters the grade of severity of HE, nor has it been included in any of the scoring systems determining the severity of liver disease such as the CTP [2] and MELD [3] scores.
Asterixis was initially described in 1949 by Adams RD et al., when they observed flapping tremors in their patients with liver disease [4]. It was associated with intermittent pauses of electrical activity of 50-200 ms on EMG tracings. It has been also referred to as ‘negative myoclonus’ in further experiments [5]. However, its exact pathophysiology is still unknown.
It was in 1994 that Conn HBJ graded asterixis according to the frequency of flaps as no flaps, rare flaps, occasional flaps and frequent flaps [Table/Fig-1] [6]. However, no study has been published till date which has sought a correlation between the increasing number of flaps and severity of liver disease. The asterixis score framed by Conn HBJ too has not been validated in any study. So, this study was done to assess the correlation between frequency of flaps in asterixis and severity of the liver disease in patients with HE.
Grading of Asterixis according to frequency of flaps [6].
| Grade of Asterixis | Description | Number of flaps (per 30 s) |
|---|
| Grade 0 | No flapping tremor | 0 |
| Grade I | Rare flapping motion | 1-2 |
| Grade II | Occasional, irregular flaps | 3-4 |
| Grade III | Frequent flaps | 5-30 |
Materials and Methods
The present prospective study was done over a period of 15 months from December 2017 to February 2019 in patients admitted to Gastroenterology ward of Sir Sunderlal Hospital, Institute of Medical Sciences, Banaras Hindu University, Varanasi, India. Patients with decompensated liver cirrhosis and HE had their flaps counted (per 30 s) at the time of their clinical stabilisation, when they were planned for discharge. Informed consent from the patients was taken. An ethical clearance was taken from the ethical committee of the institute. Patients were enrolled for the initial three months and followed up over next 12 months. Study methodology has been depicted in [Table/Fig-2]. The compliance of these patients to standard medical treatment was ensured during periodic follow-ups. Patients with HE and asterixis, with no other apparent cause for asterixis were included in the study after confirmation from two independent examiners that the abnormal movements were asterixis rather than tremors.
Flow chart for study methodology.
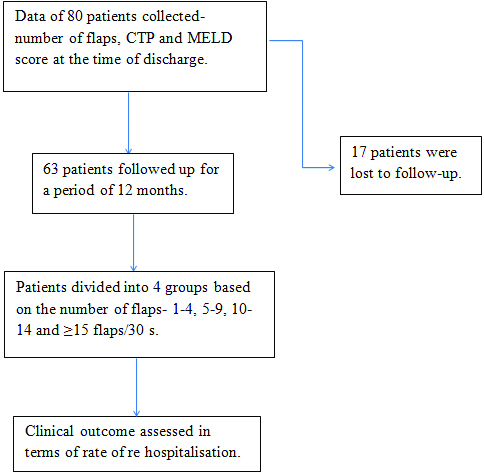
Patients who were not able to stretch their arms for 30 s and those lost to follow-up due to death or any other cause were excluded from the study.
The number of flaps were counted using a stop watch and a single examiner. Since, in some cases, the flaps were asynchronous in both the arms, so flaps were counted in both the arms separately and a mean value rounded to the nearest integral value was recorded. As with the number of flaps, CTP and MELD scores too were calculated after clinical stabilisation, when the patients were planned for discharge. CTP score was calculated using serum bilirubin, serum albumin, prothrombin time, severity of ascites and severity of HE as the parameters [1]. MELD score was calculated using online calculator with INR, serum bilirubin and serum creatinine as the parameters [2].
Statistical Analysis
MINITAB 18 software was used for statistical analysis. Continuous variables were arranged and median value was expressed. Spearman’s rank order correlation was used to study the correlation between the number of flaps and CTP and MELD scores. To assess the clinical outcome, patients were divided into four groups according to frequency of flaps- <5, 5-9, 10-14 and ≥15. Clinical outcome in terms of rate of re-hospitalisation was assessed. The p<0.05 was considered to be significant.
Results
Initially number of flaps, CTP and MELD scores of 80 patients were recorded at the time of discharge. However, 17 patients were lost to follow-up. A total of 63 patients were followed up over a period of 12 months. Patients included in the study ranged from 28-66 years of age with a median age of 45 years. All the patients had underlying decompensated liver cirrhosis as the cause of HE. We did not have any patient with type A or B HE. In 30 patients, the cause of cirrhosis was alcohol. Sixteen patients had chronic viral hepatitis whereas four patients had cirrhosis resulting from Non-alcoholic steato-hepatitis (NASH) [Table/Fig-3]. A total of 20 (31.7%) patients had HE of episodic nature whereas, 43 (68.3%) had recurrent HE [Table/Fig-3].
| Age (years)-Range (Median) | 28-66 (45) |
| Sex (n, %) | Males (n=59, 93.6%) |
| Females (n=4, 6.4%) |
| Type of HE (n, %) | Type C (63, 100%) |
| Episodic or recurrent HE (n, %) | Episodic (20, 31.7%) |
| Recurrent (43, 68.3%) |
| Cause of underlying cirrhosis (n, %) | Alcohol (30, 47.6%) |
| Viral Hepatitis (16, 25.4%) |
| NASH (4, 6.4%) |
| Wilson’s (2, 3.2%) |
| Unknown (11, 17.5%) |
(n=63)
The number of flaps ranged from 3 to 24, median value being 12. CTP score ranged from 6 to 14, median being 10; MELD score ranged from 12 to 38, median being 21. The correlation between number of flaps and CTP score was non-significant (rs=0.02, p=0.87).
Correlation between number of flaps and MELD score was also non-significant (rs=0.16, p=0.20) [Table/Fig-4]. However, only 13% of patients with <5 flaps/30 s were subsequently re-hospitalised for both hepatic and non-hepatic causes as compared to 64% of patients with >15 flaps/30 s [Table/Fig-5]. A total of 27 patients were re-hospitalised out of which 12 (44.4%) had worsening HE, 5 (18.5) had SBP and worsening HE, 6 (22.2%) had worsening ascites and 4 (14.8%) had acute kidney injury.
Association between frequency of flaps and CTP and MELD scores.
| Frequency of flaps/30s | No. of patients | CTP score-median (range) | MELD score-median (range) |
|---|
| 1-4 | 8 | 10 (8-13) | 17 (12-30) |
| 5-9 | 21 | 9 (6-12) | 20 (12-30) |
| 10-14 | 23 | 10 (6-14) | 21 (14-38) |
| ≥15 | 11 | 10 (7-13) | 21 (18-31) |
Flap frequency compared to rate of re-hospitalisation.
| No. of flaps (per 30s) | Number of patients | No. of patients re hospitalised (%) |
|---|
| 1-4 | 8 | 1 (13) |
| 5-9 | 21 | 6 (29) |
| 10-14 | 23 | 13 (57) |
| ≥15 | 11 | 7 (64) |
Discussion
To the best of our knowledge, the association between frequency of flaps in asterixis and severity of liver disease has not been studied till date. Though we did not study survival in our study, the fact that flap frequency is an independent predictor for re-hospitalisation makes it a worthy inclusion in our clinical assessment tool. However, all patients with HE do not have asterixis, and it is very important to differentiate asterixis in HE with other diseases [7]. Moreover, in all patients with asterixis, it is not possible to count the number of flaps as some are irritable whereas others are too frail to keep their arms stretched for 30 seconds. In our study, we recorded the number of flaps and calculated CTP and MELD scores after clinical stabilisation. This helped us to include some patients in our study in whom recording the number of flaps would not have been possible initially due to their altered consciousness.
Our study included patients from both the sexes and varied age groups. Since asterixis is associated with intermittent loss of muscle tone, it is possible that it can be affected by muscle mass, age or sex, though we do not have studies to confirm the same. Since we have not completely understood the pathogenesis of asterixis, we do not know about the confounding factors which might affect the frequency of flaps.
Conclusion
There was no significant correlation between number of flaps and CTP and MELD scores. However, higher number of flaps was an independent predictor for re-hospitalisation, most of them for worsening HE.
(n=63)
[1]. Hepatic Encephalopathy in Chronic Liver Disease: 2014 Practice Guidelines by the European Association for Study of the Liver DiseasesJ Hepatol 2014 [Google Scholar]
[2]. Child CG, Turcotte JG, Surgery and portal hypertensionIn: The liver and portal hypertension. Edited by CG Child 1964 PhiladelphiaSaunders:50-64. [Google Scholar]
[3]. Kamath P, Wiesner RH, Malinchoc M, Kremers W, Therneau TM, Kosberg CL, A model to predict survival in patients with end-stage liver diseaseHepatology 2001 33(2):464-70.10.1053/jhep.2001.2217211172350 [Google Scholar] [CrossRef] [PubMed]
[4]. Adams RD, Foley JM, The neurological changes in the more common types of severe liver diseaseTrans Am Neurol Assoc 1949 74:217-19. [Google Scholar]
[5]. Young RR, Shahani BT, Asterixis: One type of negative myoclonusAdv Neurol 1986 43:137-56. [Google Scholar]
[6]. Conn HBJ, Hepatic encephalopathy: Syndromes and therapies 1994 Bloomington, IllinoisMedi-Ed Press [Google Scholar]
[7]. Jones EA, Weissenborn K, Neurology and the liverJournal of Neurology, Neurosurgery & Psychiatry 1997 63:279-93.10.1136/jnnp.63.3.2799328238 [Google Scholar] [CrossRef] [PubMed]