Sublingual Foregut Cyst Lined by Respiratory Epithelium- A Rare Cause of Cystic Lesion in the Floor of the Mouth
Yasmeen Khatib1, Neha Khaitan2, Yogita M Talpade3, Manisha S Khare4, Prajakta A Gupte5
1 Associate Professor, Department of Pathology, HBT Medical College and Dr R N Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
2 Speciality Medical Officer, Department of Pathology, HBT Medical College and Dr R N Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
3 Assistant Professor, Department of Pathology, HBT Medical College and Dr R N Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
4 Professor, Department of Pathology, HBT Medical College and Dr R N Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
5 Assistant Professor, Department of Pathology, HBT Medical College and Dr R N Cooper Hospital, Juhu, Mumbai, Maharashtra, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Yogita M Talpade, Assistant Professor, Department of Pathology, HBT Medical College & Dr R N Cooper Hospital, Juhu, Mumbai-56, Maharashtra, India.
E-mail: yogita.talpade@gmail.com
Foregut cysts of the oral cavity are rare developmental anomalies which are lined by gastric, intestinal, squamous or respiratory epithelium or a mixture of these epithelia. A 10-year-old boy presented with a large cyst in the floor of the mouth and had difficulty in speech and chewing of food. On Magnetic Resonance Imaging (MRI) examination a diagnosis of ranula was given. Surgical excision was done and a diagnosis of foregut cyst lined by respiratory epithelium was given on histopathological examination. Till now only 21 cases of lingual foregut cyst with respiratory lining have been reported. We report the 22nd case for its rarity and because these lesions can pose a diagnostic dilemma and should be included in the differential diagnosis of cystic lesions in the oral cavity especially in paediatric population.
Developmental cyst, Pseudostratified ciliated epithelium, Sublingual swelling
Case Report
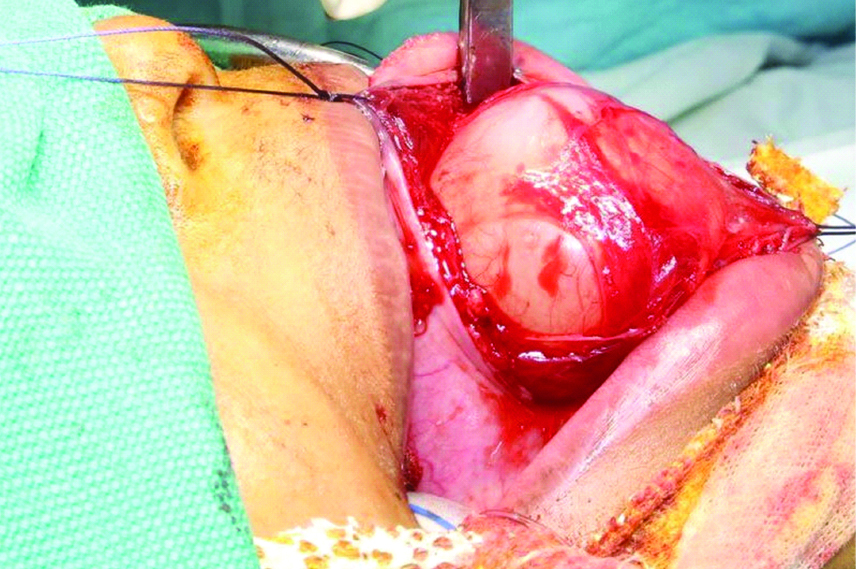
A 10-year-old boy presented with a swelling in the floor of the mouth which was present since birth. Initially, the swelling was small and it gradually increased to the present size. He had difficulty in speaking since an early age and chewing of solid food since one month. His medical history was unremarkable. On clinical examination, the swelling was non-tender, soft, cystic, translucent, and measured 5×352 cm in size. The tongue was elevated due to the swelling [Table/Fig-1]. On MRI, a well-defined cystic, non-enhancing sublingual lesion was seen in the floor of the mouth reaching up to the mylohyoid muscle, and a diagnosis suggestive of ranula was given. Under general anaesthesia, an incision was taken extending from the tip of the tongue till the posterior tongue in the sublingual region and the cyst was enucleated by blunt dissection and the cyst was separated from the intrinsic muscles of the tongue [Table/Fig-2].
Clinical picture showing a cystic swelling in the floor of the mouth.

Intraoperative dissection and excision of the cyst.
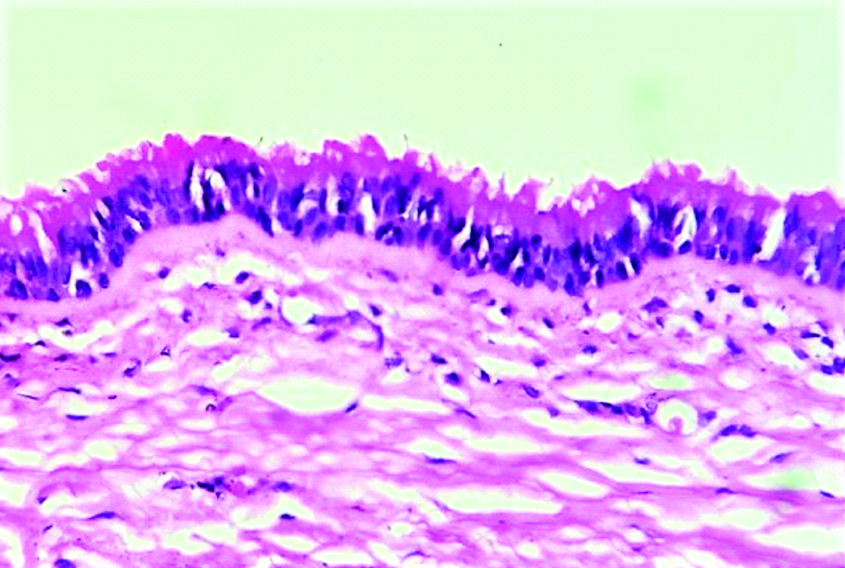
Grossly, a large single cystic mass was seen measuring 6×4×3 cm [Table/Fig-3]. On sectioning, the cyst had a smooth wall, was uniloculated, and filled with mucoid material. Microscopic examination of the cyst wall showed a cyst lined by pseudostratified ciliated epithelium which was flattened at places [Table/Fig-4]. Wall of the cyst showed fibro collagenous tissue along with underlying muscle. A diagnosis of benign foregut cyst with respiratory lining was given. The postoperative course was uneventful.
Gross specimen showing a large smooth walled cyst.

Microscopy of the cyst showing respiratory lining composed of ciliated pseudo- stratified epithelium (H&E 40X).
Discussion
Foregut cysts are a rare cause of cystic lesions involving the tongue or the floor of the mouth. They have a varied terminology and were also known as lingual choristoma, enteric duplication cysts, lingual alimentary cysts etc., [1]. The commonest location of these cysts is in the chest and abdomen but involvement of tongue and oral cavity is unusual and is seen only in 0.3% of the cases [1,2]. There are three criteria to make a diagnosis of foregut cysts- have to contain epithelium derived from foregut, should be attached to a portion of the foregut and covered by smooth muscle layer [2]. The epithelial lining seen in these cysts is gastric, intestinal, respiratory or a mixture of these cells which suggests a foregut origin [1]. Foregut cysts of oral cavity are usually present at birth and gradually increase in size. A few cases have been detected during antenatal ultrasound examination [3]. Most cases present as asymptomatic swelling in the floor of the mouth but in 30% of cases they present with difficulty in feeding, swallowing, respiration or speech [4]. The present case presented with difficulty in speech and chewing of solid food because of its large size and location in the floor of the mouth. Peptic ulceration in cyst with gastric lining, sinus formation with chronic mucus secretion have been reported. Malignant transformation has been reported in a long standing case of foregut cyst of head and neck [2]. MRI is recommended to delineate the extent of these cysts but it shows overlapping features with more common cystic lesions occurring at this location [5].
Manor Y et al., have histologically reviewed 52 cases of lingual cysts out of which only three involved the floor of the mouth [6]. They reported one case of lingual cyst on the tongue lined by respiratory epithelium. Age ranged from new born to 42 years with a mean age of 5 1/2 years. Cysts were more common in males as compared to females with a male female ratio of 1.6:1. Grossly the size varied from 1 cm to 6.5 cm with a mean size of 2.3 cm. Out of the 52 cases of foregut cyst reviewed histologically, 12 contained mainly respiratory epithelium, 21 cases contained mainly gastric epithelium, three cases contained mainly intestinal epithelium, one contained both gastric and intestinal epithelium and 15 were composed of combination of respiratory and gastric or intestinal epithelium. As these cysts were reported by different names Manor recommended a uniform nomenclature with a descriptive diagnosis based on histopathological examination. He referred them as foregut cysts with gastric epithelium, foregut cysts with respiratory epithelium and foregut cysts with respiratory and gastric epithelium [6]. Peters SM et al., have reported 2 cases of foregut cysts lined with respiratory epithelium which is similar to our case [7]. On review of literature they have found only 19 similar cases reported earlier which had only respiratory lining with absence of gastric epithelium. Patients presented with swelling on the dorsal tongue, ventral tongue and floor of the mouth [8-17]. The present case is thus the 22rd case to be reported [Table/Fig-5].
Cases of lingual cyst lined by respiratory epithelium with absence of gastric epithelium.
| Sr. No. | Author (Year) | No. of cases | Age (Years) | Sex | Site | Clinical symptoms | Histopathologic features (Cyst lining) |
|---|
| 1. | Fink (1963) [8] | 1 | 5 | Male | Dorsum tongue, anterior third | Difficulty in eating and drinking. | Pseudostratified ciliated columnar+cuboidal epithelium |
| 2. | Constantinides et al., (1982) [9] | 1 | 9 month old | Female | Ventral tongue | Difficulty in eating and closing of mouth | Pseudostratified ciliated columnar+squamous+cuboidal epithelium |
| 3. | Wiersma et al., (1992) [10] | 7 | Various (neonate-6 years) | | Anterior two-thirds of tongue | Asymptomatic; Difficulty in feeding | Pseudostratified ciliated columnar+squamous+cuboidal+columnar epithelium |
| 4. | Naidoo (1997) [11] | 1 | 42 | Male | Centre of dorsum of tongue | Difficulty in eating and speaking | Pseudostratified non-ciliated columnar+squamous+cuboidal+ciliated columnar epithelium |
| 5. | Kim et al., (1998) [12] | 1 | 27 | Male | Sublingual | Non-specific | Pseudostratified ciliated columnar+squamous epithelium |
| 6. | Manor Y et al., [6] | 1 | 11 | Male | Body of tongue | Difficulty in speaking and swallowing | Pseudostratified ciliated columnar+cuboidal epithelium+goblet cells |
| 7. | Azanero (2009) [13] | 2 | 4 | Male | Right ventral tongue | Difficulty in breastfeeding | Pseudostratified ciliated columnar+squamous epithelium+goblet cells |
| 21 | Male | Anterior middle third of dorsum of tongue | Difficulty in eating and speaking | Pseudostratified ciliated columnar+squamous epithelium+goblet cells |
| 8. | Boffano P et al., [14] | 1 | 35 | Female | Floor of mouth | Asymptomatic | Pseudostratified ciliated columnar+goblet cells |
| 9. | Chai RL et al., [5] | 1 | 6 month old | Female | Ventral tongue | Difficulty in feeding | Pseudostratified ciliated columnar |
| 10. | Junejo et al., (2011) [15] | 1 | 1 | Female | Anterior dorsal tongue | Difficulty in eating | Pseudostratified ciliated columnar+squamous epithelium |
| 11. | Fortier et al., (2013) [16] | 1 | 17 month old | Male | Left anterior tongue | Asymptomatic | Pseudostratified ciliated columnar+some mucinous glands |
| 12. | Kwak EJ et al., [17] | 1 | 2 | Female | Ventral tongue | Asymptomatic | Pseudostratified ciliated columnar |
| 13. | Peters SM et al., [7] | 2 | 10 | Male | Floor of mouth | Asymptomatic | Ciliated columnar |
| 27 | Female | Floor of mouth | Asymptomatic | Pseudostratified ciliated columnar+goblet cells |
| 14. | Current case | 1 | 10 | Male | Floor of mouth | Difficulty eating and speaking | Pseudostratified ciliated columnar |
There are many overlapping theories for the development of these lesions; hence the exact pathogenesis remains debatable. They could arise from developmental derangement of the foregut. During the 3rd week of embryogenesis, the ventral part of the foregut gives rise to respiratory tract and the dorsal part to proximal gastrointestinal tract. The pharyngeal arches lie at proximity to the primitive foregut; hence the pluripotent cells of the foregut may sometimes get entrapped between the developing tongue and when exposed to varying influences and environment differentiate into respiratory or gastro-intestinal epithelium [2,18].
Cystic lesions in the floor of the mouth have a wide range of differential diagnosis and include ranula, dermoid cyst, thyroglossal duct cyst, lymphangioma, haemangioma, lymphoepithelial cyst and salivary gland neoplasms [5,14,17]. Clinically it is difficult to differentiate among these lesions. Diagnosis is made after excision and histopathological examination. Oral cysts lined by respiratory epithelium are benign lesions and are treated by surgical excision.
Conclusion
Lingual cysts lined by respiratory epithelium are a rare cause of cystic lesion in the floor of the mouth with only 21 cases reported in literature. Early diagnosis and excision of foregut cyst is necessary because it can cause difficulty in feeding, speech, swallowing and respiration. As foregut cysts have a varied terminology it is recommended to label it as a foregut cyst followed by the type of epithelial lining.
[1]. Luo Y, Shillingford N, Koempel JA, Histopathologic finding of both gastric and respiratory epithelia in a lingual foregut cystCase Reports in Medicine 2015 :e1-e6.10.1155/2015/27837626294913 [Google Scholar] [CrossRef] [PubMed]
[2]. Kieran SM, Robson CD, Nosé V, Rahbar R, Foregut duplication cysts in the head and neck: presentation, diagnosis, and managementArch Otolaryngol Head Neck Surg 2010 136(8):778-82.10.1001/archoto.2010.12720713753 [Google Scholar] [CrossRef] [PubMed]
[3]. Karam O, Pfister RE, Extermann P, La Scala GC, Congenital lingual cystsJ Pediatr Surg 2007 42(4):E25-27.10.1016/j.jpedsurg.2007.01.06017448749 [Google Scholar] [CrossRef] [PubMed]
[4]. Said-Al-Naief N, Fantasia JE, Sciubba JJ, Ruggiero S, Sachs S, Heterotopic oral gastrointestinal cyst: report of 2 cases and review of the literatureOral Surg Oral Med Oral Pathol Oral Radiol Endod 1999 88(1):80-86.10.1016/S1079-2104(99)70197-6 [Google Scholar] [CrossRef]
[5]. Chai RL, Ozolek JA, Branstetter BF, Mehta DK, Simons J, Congenital choristomas of the oral cavity in childrenLaryngoscope 2011 121(10):2100-106.10.1002/lary.2175821826675 [Google Scholar] [CrossRef] [PubMed]
[6]. Manor Y, Buchner A, Peleg M, Taicher S, Lingual cyst with respiratory epithelium: an entity of debatable histogenesisJ Oral Maxillofac Surg 1999 57(2):124-29.10.1016/S0278-2391(99)90222-7 [Google Scholar] [CrossRef]
[7]. Peters SM, Park M, Perrino MA, Cohen M, Lingual cyst with respiratory epithelium: Report of two cases and review of the literatureOral Surg Oral Med Oral Pathol Oral Radiol 2018 126(6):e279-e284.10.1016/j.oooo.2018.05.01129929866 [Google Scholar] [CrossRef] [PubMed]
[8]. Fink HA, Retention cyst of the tongue (glossocele)Oral Surg Oral Med Oral Pathol 1963 16:1290-93.10.1016/0030-4220(63)90401-8 [Google Scholar] [CrossRef]
[9]. Constantinides CG, Davies MR, Cywes S, Intralingual cysts of foregut originS Afr J Surg 1982 20:227-32. [Google Scholar]
[10]. Wiersma R, Hadley GP, Bosenberg AT, Intralingual cysts of foregut originJ Pediatr Surg 1992 27:1404-06.10.1016/0022-3468(92)90186-B [Google Scholar] [CrossRef]
[11]. Naidoo LC, Median lingual cyst: review of the literature and report of a caseJ Oral Maxillofac Surg 1997 55:172-75.10.1016/S0278-2391(97)90238-X [Google Scholar] [CrossRef]
[12]. Kim Y, Ahn SK, Lee SH, Sublingual foregut cystJ Dermatol 1998 25:476-8.10.1111/j.1346-8138.1998.tb02438.x9714983 [Google Scholar] [CrossRef] [PubMed]
[13]. Azanero WD, Mazzonetto R, Leon JE, Lingual cyst with respiratory epithelium: a histopathological and immunohistochemical analysis of two casesInt J Oral Maxillofac Surg 2009 38:388-92.10.1016/j.ijom.2009.01.00319217261 [Google Scholar] [CrossRef] [PubMed]
[14]. Boffano P, Zavattero E, Campisi P, Gallesio C, Surgical treatment of an oral cyst with respiratory epitheliumJ Craniofac Surg 2009 20(4):1275-77.10.1097/SCS.0b013e3181ae179419625847 [Google Scholar] [CrossRef] [PubMed]
[15]. Juneja M, Boaz K, Srikant N, Lingual cyst lined by respiratory epithelium: a case report and review of literatureFetal Pediatr Pathol 2011 30:225-32.10.3109/15513815.2011.55580721434827 [Google Scholar] [CrossRef] [PubMed]
[16]. Fortier A, Boyer C, Ducasse H, Bronchogenic cyst of the tongue in an infantRev Laryngol Otol Rhinol 2013 134(3):157-59. [Google Scholar]
[17]. Kwak EJ, Jung YS, Park HS, Jung HD, Oral foregut cyst in the ventral tongue: a case reportJ Korean Assoc Oral Maxillofac Surg 2014 40(6):313-15.10.5125/jkaoms.2014.40.6.31325551098 [Google Scholar] [CrossRef] [PubMed]
[18]. Daley TD, Wysocki GP, Lovas GL, Smout MS, Heterotopic gastric cyst of the oral cavityHead Neck Surg 1984 7(2):168-71.10.1002/hed.28900702126511438 [Google Scholar] [CrossRef] [PubMed]