Malakoplakia of the Uterus: A Rare Cause of Postmenopausal Bleeding Mimicking Malignancy
Chinmoyee Sonowal1, Phatik Chandra Kalita2, Arpana Das3, Himajit Rabha4, Anjan Saikia5
1 Junior Consultant, Department of Obstetrics and Gynaecology, GNRC Medical, North Guwahati, Assam, India.
2 Senior Consultant and Head, Department of Obstetrics and Gynaecology, GNRC Medical, Guwahati, Assam, India.
3 Consultant, Department of Obstetrics and Gynaecology, GNRC Medical, Guwahati, Assam, India.
4 Consultant, Department of General Surgery, GNRC Medical, Guwahati, Assam, India.
5 Consultant, Department of Pathology, GNRC Medical, Guwahati, Assam, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Chinmoyee Sonowal, Palm Groove Enclave, Flat No. 307/I, Juripar Path, Guwahati, Assam, India.
E-mail: chinmoyee35@gmail.com
Malakoplakia is a rare chronic granulomatous disease. It was first reported in 1902 by Michaelis and Gutmann. It may involve any part of the body, most commonly affecting the urinary tract, mainly the urinary bladder. The involvement of uterus resulting in post-menopausal bleeding is extremely rare but not unusual. So, in the differential diagnosis of post-menopausal bleeding, this condition should be kept in mind which poses as a diagnostic enigma requiring a high degree of suspicion from the clinician, the radiologist and the pathologist. Due to paucity of data owing to the rarity of the condition, there are no treatment guidelines for this condition, leading to a therapeutic dilemma. We report herein an unusual case of malakoplakia of the uterus with actinomycoses co-infection in a 60-year-old lady with postmenopausal bleeding and an abdominopelvic lump mimicking malignancy.
Inclusion bodies, Michaelis-gutmann bodies, Von-hansemann cells
Case Report
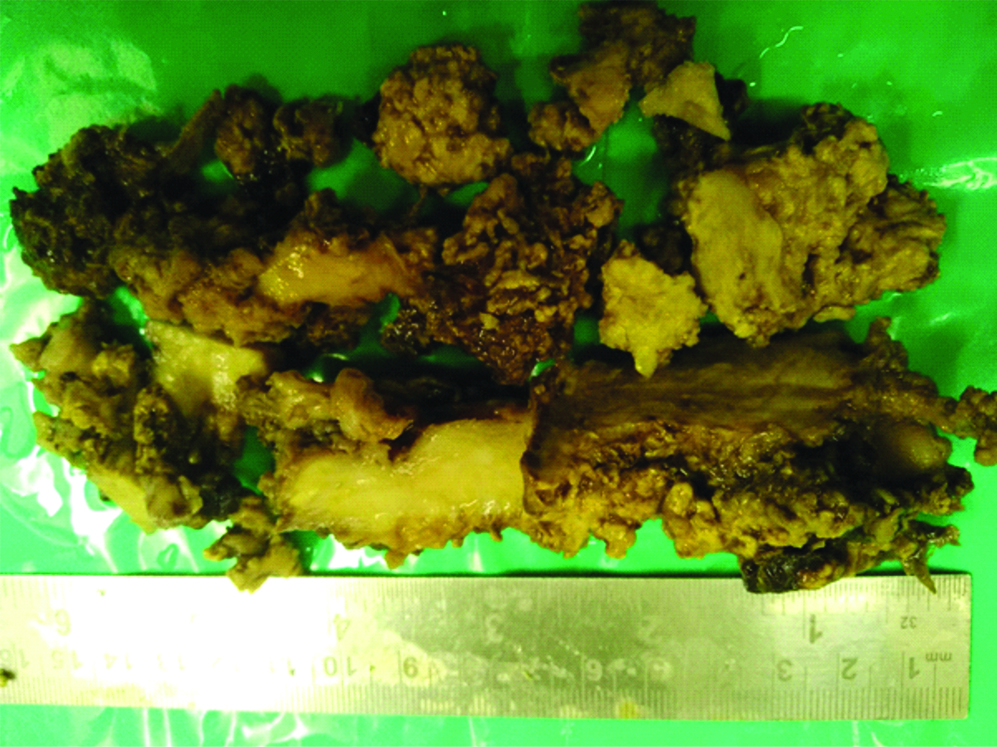
A 60-year-old lady presented with chief complaint of bleeding per vaginum since one month. She had attained menopause 12 years back with three vaginally delivered children. She had also undergone tubectomy 20 years back by mini-laparotomy technique with history of wound infection. She was hypertensive and was taking antihypertensives. On general physical examination, she was an obese lady with severe pallor and stable vitals. Her abdominal examination revealed a 14 weeks abdomino-pelvic mass which was firm in consistency, non-tender, with restricted mobility. Another lump was felt separately on the left side of umbilicus. On per speculum examination, cervix was pulled up, normal when visualised with blood coming out through it. On per vaginal examination, cervix was firm, regular, smooth, uterus was 14 weeks size anteverted, firm, nontender, with restricted mobility with free fornices bilaterally. She had undergone Pap’s smear and therapeutic and diagnostic D&C in another institution 10 days back without any evidence of suspected malignancy in the reports. A plain CT from another institution reported it as a fibroid measuring 50×49×46 mm in posterior wall of the uterus and an ill defined lesion of size 8.67×5.33 cm in the anterior abdominal wall in the region of umbilicus. Her haematological investigation revealed severe anaemia with haemoglobin level of 4.5 gm%. A provisional diagnosis of uterine fibroid with degeneration or malignant transformation, endometrial carcinoma and uterine sarcoma were made. She was transfused three units of packed red blood cells. Despite medical management to control the bleeding, she continued to bleed and therefore she was posted for emergency hysterectomy. On opening the abdomen, there was a sinus tract from the scar of previous sterilisation procedure to the lump near the umbilicus. The abdominal wall was thickened and fibrosed around this area. Loops of bowel were adherent to this thickened area forming a lump. Bowel was also adherent to the entire anterior abdominal wall under the incision and the lateral walls as well. Extensive adhesiolysis was done upto the pelvis. Sigmoid colon was densely adherent to the fundal and posterior surface of the uterus which was removed. Apart from this, the pelvic anatomy was completely distorted. Uterus was densely adhered to the bladder with unidentifiable round ligaments and fallopian tubes. There was extensive fibrosis and thickening in the area of broad ligament with buried fallopian tubes and ovaries. Uterus and the uterine mass had to be removed in piece-meal and cervix and ovaries had to be left behind. Sigmoid colon perforation sustained during adhesiolysis was repaired and a transverse loop colostomy had to be performed. After ensuring haemostasis, abdomen was closed with placement of drain. Grossly the specimen that was taken out consisted of multiple irregular grey white to yellow tissue, measuring 150 grams. The anatomy of the uterus was distorted. Outer surface as well as inner surface showed multiple friable irregular papillary structures [Table/Fig-1].
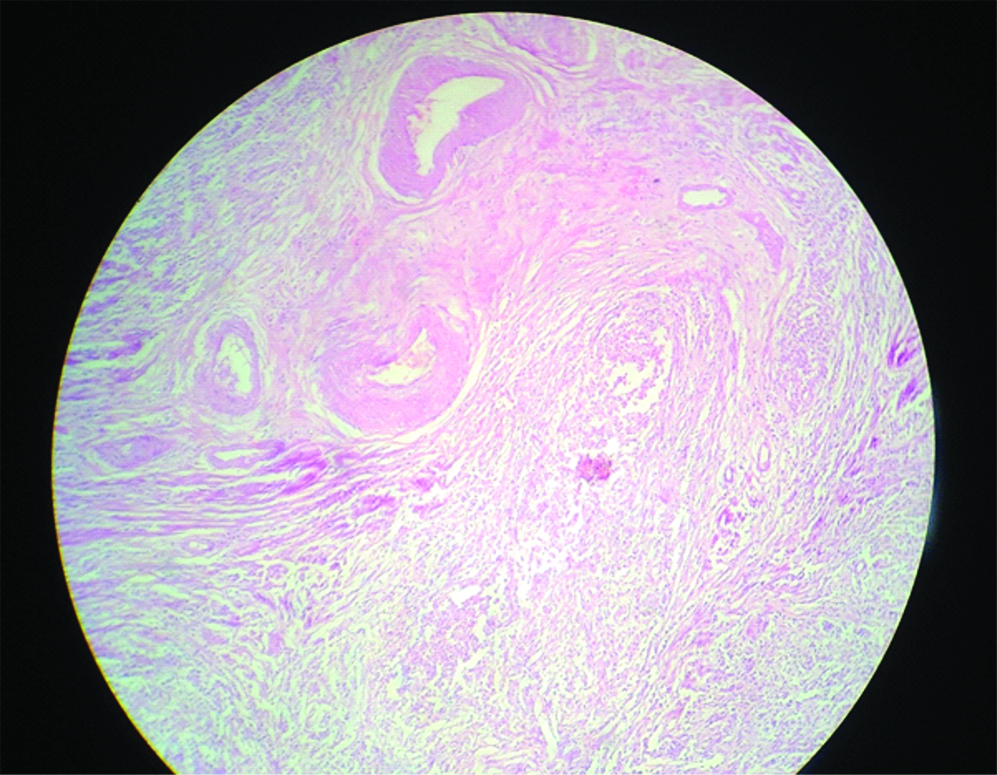
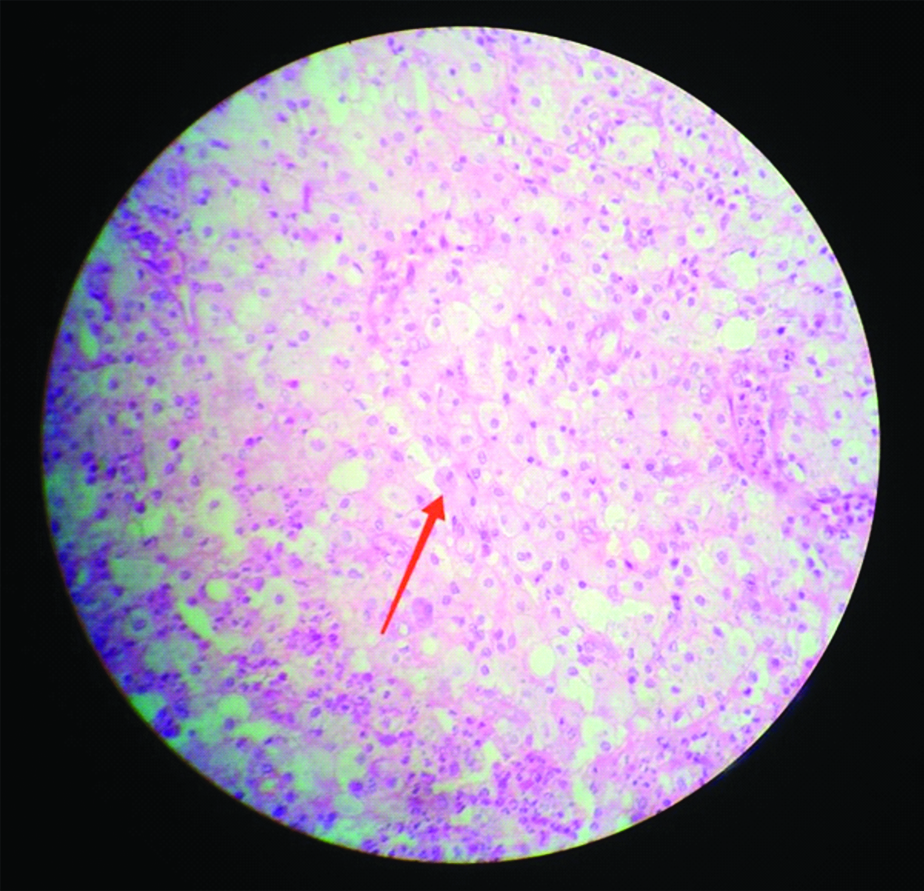
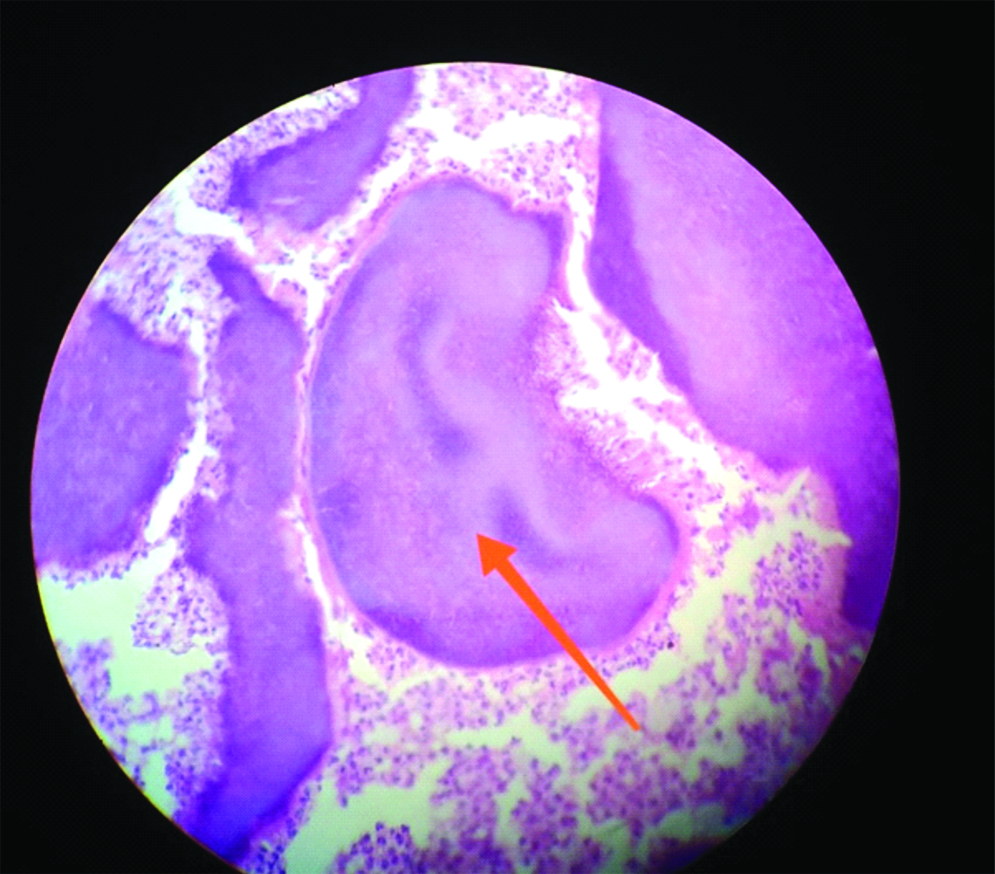
Microscopically, multiple sections showed large areas of foamy histiocytes infiltrating the myometrium of uterus [Table/Fig-2] and pathognomonic Michaelis-Gutmann bodies which are basophilic inclusion bodies within enlarged foamy macrophages [Table/Fig-3]. There was also evidence of Actinomycosis at places [Table/Fig-4]. No evidence of malignancy was seen. Based on the histopathological report, a final diagnosis of malakoplakia of the uterus was made. Postoperatively she was started on cotrimoxazole after going through literature. She responded well and has remained asymptomatic so far.
Photomicrograph shows foamy histiocytes infiltrating myometrium (H&E Stain, 4x).
Photomicrograph showing abundant foamy histiocytes with michaelis-gutmann body (Arrow) (H&E Stain, 40x).
Photomicrograph showing basophilic sulphur granules with periphery showing filamentous bacteria consistent with actinomycoses (H&E 40x).
Discussion
Malakoplakia is an extremely rare condition with fewer than 1000 cases reported in the USA per year and fewer still in India [1]. So far there has not been any report of uterine malakoplakia from India. It is a chronic inflammatory disease, which although is benign may take a morbid course. The patients are usually above 50 years with a female preponderance. The female to male ratio is 2:1 [2]. It occurs rarely in children. Most patients have associated conditions related to immuno-suppression as in organ transplants, autoimmune conditions requiring steroid use, chemotherapy, chronic systemic disease, alcohol abuse, poorly controlled diabetes, AIDS [3]. Nearly, 90% of patients have coliform bacteria detected in urine, blood or tissue, suggesting an infectious cause and 40% has immuno-deficiency or any autoimmune disease [4]. The most commonly found bacterium is Escherichia coli, but Klebsiella, Proteus, Pseudomonas, Mycobacterium avium, Mycobacterium tuberculosis, Shigella, Staphylococcus aureus, Enterococcus spp. were also found [5,6].
The exact pathogenesis of this condition is still unknown. It is believed that there is an acquired defect in the lysosomal activity of lysosomes triggered by infectious agents, mainly by gram negative bacilli, and associated with immunosuppression. There is defective bacterial digestion leading to accumulation of calcium and iron in residual bacterial glycolipids. Microscopically, there is an accumulation of typical macrophages called as Von-Hansemann cells which are enlarged macrophages with foamy cytoplasm and eccentric, hyperchromatic, round nuclei. They may contain PAS positive and Von Kossa positive intra-cytoplasmic and extra-cytoplasmic inclusions called as Michaelis-Gutmann bodies which are considered pathognomonic of this condition. These bodies arise from phagocytosis of bacterial degradation products providing a matrix for deposition of needle like crystals, resembling hydroxyapatite. These are round-ovoid, basophilic, concentric laminated inclusions in the Von-Hanseman cells. However, Michaelis-Gutmann bodies may not be seen in early stages of the disease and are not absolutely necessary for the diagnosis [7,8]. In our case, we observed that the disease developed in a site of possible prior contamination by bacteria with the history of post-tubectomy infected wound in this case and the presence of the sinus tract with signs of chronic inflammation around it.
Radiologically and grossly, this condition may simulate other inflammatory process or neoplasm. It may be misdiagnosed clinically as a malignant condition. Thus, ruling out malignancy is a concern especially in a menopausal lady. The possible gynaecological presentation can be post-menopausal bleeding, abnormal uterine bleeding in a menstruating women, abnormal cervical smears, a malignant looking cervical growth or a pelvic mass.
Pelvic malakoplakia was reported in a 30-year-old AIDS patient after disseminated M. Simiae infection. She underwent laparotomy for the same which revealed a large lobulated mass arising out of right adnexa with extensive adhesion to surrounding structures. Only partial resection and biopsy of the mass were performed and histopathological examination revealed malakoplakia. However the outcome was not known as the patient was lost to follow-up [3]. Shaikh H et al., reported malakoplakia of uterus in a 28-year-old parous lady. She had undergone laparotomy and later on started on ciprofloxacin to which she responded well [9]. Eckford SD et al., reported an 81-year-old lady with postmenopausal bleeding who presented with an ulcerating polypoidal bleeding lesion in cervix mimicking malignancy. The polyp was excised and the histopathological examination revealed features of malakoplakia without any evidence of malignancy or infection [10]. Hall V, reported another case of cervical malakoplakia wherein the entire cervix was replaced by a fungating mass which reached half of the vagina. Histology of the biopsied specimen showed chronic inflammatory granulomata with pathognomonic Michaelis-Gutmann bodies without any evidence of malignancy [11]. A case of malakoplakia in cervico-vaginal smear was reported in a 54-year-old lady which consisted of abundant histiocytes with characteristic Michaelis-Gutmann bodies, polymorphonuclear leukocytes, lymphocytes and plasma cells. Colposcopic examination of the same revealed friable, easily bleeding tissue in the uterine cervix and vaginal fornix [12]. Ehara T et al., reported malakoplakia in an endometrial curettage specimen of an 87-year-old post-menopausal lady presenting with vaginal bleeding [13]. Chou SC et al., reported a case of malakoplakia extensively involving the ovary, fallopian tube and uterus in a 47-year-old lady with poorly controlled diabetes mellitus. They proposed that it was the result of poorly controlled diabetes leading to impaired leukocyte function and combined with E.coli infection as evident from cultures led to the extensive malakoplakia [14]. Kiely NP et al., reported a case of uterine malakoplakia with post-menopausal bleeding in an immunocompromised lady [15]. Another case of extensive malakoplakia of pelvic organs causing bilateral hydronephrosis due to ureter involvement was reported in a 49-year-old lady with type 2 diabetes, obesity, asthma, and congestive cardiac failure. She received long term antibiotics resulting in shrinkage in size of pelvic mass [16].
Management is challenging as there are no guidelines. Going through literature, we found that treatment option depends on presentation. It can be medical, surgical or both. Type of surgical intervention depends on extent and location of the disease, which may range from simple excision to long complex abdominal surgeries if bowel, urinary bladder or ureter is involved. Antibiotics like aminoglycosides, ciprofloxacin, cephalosporin, cotrimoxazole with their macrophage concentrating capacity have been tried with good results. Van der Voort HJ et al., compared treatment options and concluded that surgical excision achieved higher cure rate (90%) and on comparing antibiotics, Quinolones were found to be superior [17].
Conclusion
Malakoplakia of uterus is a rare condition. However, to the best of our knowledge malakoplakia of uterus with actinomycoses co-infection as a cause of post-menopausal bleeding has not been reported so far. A high degree of clinical suspicion is needed to diagnose this condition. This case highlights the importance of keeping this condition in the differential diagnosis while evaluating a case of postmenopausal bleeding. Extensive pelvic malakoplakia can be mistaken for invasive cancer and so careful histopathological diagnosis is essential.
[1]. Ho M, Wu J, Skinnider B, Kavanagh A, Prostatic malakoplakia: A case report with review of the literatureJ Surg Case Rep 2018 3:01-03.10.1093/jscr/rjy050 [Google Scholar] [CrossRef]
[2]. Long JP Jr, Althausen AF, Malacoplakia: A 25-year experience with a review of the literatureJ Urol 1989 141:1328-31.10.1016/S0022-5347(17)41297-3 [Google Scholar] [CrossRef]
[3]. Chitasombat MN, Wattanatranon D, Disseminated Mycobacterium simiae with pelvic malakoplakia in an AIDS patientClin Med Insights Case Rep 2015 8:89-91.10.4137/CCRep.S3175126483613 [Google Scholar] [CrossRef] [PubMed]
[4]. Jung SJ, Kang HC, Choi JJ, Malakoplakia of the kidney extending to the descending colon in a patient with secondary adrenal insufficiency: A case reportKorean J Fam Med 2011 32(6):367-72.10.4082/kjfm.2011.32.6.36722745875 [Google Scholar] [CrossRef] [PubMed]
[5]. Stanton MJ, Maxted W, Malacoplakia: A study of the literature and current concepts of pathogenesis, diagnosis and treatmentJ Urol 1981 125:139-46.10.1016/S0022-5347(17)54940-X [Google Scholar] [CrossRef]
[6]. Yuoh G, Hove MG, Wen J, Haque AK, Pulmonary malakoplakia in acquired immunodeficiency syndrome: An ultrastructural study of morphogenesis of Michaelis-Gutmann bodiesMod Pathol 1996 9:476-83. [Google Scholar]
[7]. Afonso JPJM, Ando PN, Padilha MHV, de Q, Michalany NS, Porro AM, Cutaneous malakoplakia: Case report and reviewAn Bras Dermatol 2013 88(3):432-37.10.1590/abd1806-4841.2013179023793204 [Google Scholar] [CrossRef] [PubMed]
[8]. An T, Ferenczy A, Wilens SL, Melicow M, Observations on the formation of Michaelis-Gutmann bodiesHum Pathol 1974 5:753-58.10.1016/S0046-8177(74)80044-4 [Google Scholar] [CrossRef]
[9]. Shaikh H, Khan PE, Faridi N, Malakoplakia of the uterusJ Pak Med Assoc 1994 44:76-77. [Google Scholar]
[10]. Eckford SD, Hirschowitz L, Brown I, Akande V, Malakoplakia of the uterine cervix-A rare cause of postmenopausal bleedingJ Obstet Gynaecol 1994 14:51-52.10.3109/01443619409025971 [Google Scholar] [CrossRef]
[11]. Hall V, Malakoplakia of the cervix uteriJ Obstet Gynaecol 1996 16:6210.3109/01443619609028393 [Google Scholar] [CrossRef]
[12]. Chun YK, Hong SR, Kim HS, Kim JY, Cytologic findings of malakoplakia of the uterine cervix and the vagina-A case reportKorean J Cytopathol 2008 19(2):164-67.10.3338/kjc.2008.19.2.164 [Google Scholar] [CrossRef]
[13]. Ehara T, Korematsu M, Kawamura K, Shimoji K, Matsui H, Shimizu K, Malakoplakia of the endometriumJ Jpn Soc Clin Cytol 2013 52(2):139-42.10.5795/jjscc.52.139 [Google Scholar] [CrossRef]
[14]. Chou SC, Wang JS, Tseng HH, Malacoplakia of the ovary, fallopian tube and uterus: A case associated with diabetes mellitusPathol Int 2002 52:789-93.10.1046/j.1440-1827.2002.01420.x12588449 [Google Scholar] [CrossRef] [PubMed]
[15]. Kiely NP, Anderson L, Arora H, Benness C, A novel cause of postmenopausal bleeding in an immunosuppressed patientBMJ Case Rep 2018 10.1136/bcr-2018-22564229991552 [Google Scholar] [CrossRef] [PubMed]
[16]. Dong H, Dawes S, Philip J, Chaudhri S, Subramonian K, Malakoplakia of the urogenital tractUrol Case Rep 2015 3:06-08.10.1016/j.eucr.2014.10.00226793484 [Google Scholar] [CrossRef] [PubMed]
[17]. van der Voort HJ, ten Velden JA, Wassenaar RP, Silberbusch J, Malacoplakia: two case reports and a comparison of treatment modalities based on a literature reviewArch Intern Med 1996 156:577-83.10.1001/archinte.1996.004400501370158604965 [Google Scholar] [CrossRef] [PubMed]