A Study of Serosal Covering of the Appendix
S Swayam Jothi1, Sreelekha Dorairaj2, N Sujatha3
1 Professor, Department of Anatomy, Shri Sathya Sai Medical College and Research Institute, Ammapettai, Chengalpet Taluk, Kancheepuram District, Tamil Nadu, India.
2 Assistant Professor, Department of Anatomy, Sree Balaji Medical College and Hospital, Chromepet, Tamil Nadu, India.
3 Tutor, Department of Anatomy, Shri Sathya Sai Medical College and Research Institute, Ammapettai, Chengalpet Taluk, Kancheepuram District, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sreelekha Dorairaj, New No. 15, Old No. 7, Third Canal Cross Road, Gandhinagar, Adyar, Chennai, Tamil Nadu, India.
E-mail: sreedorai@gmail.com
Introduction
Vermiform Appendix is a part of caecum and hence a part of large intestine. Normally, it does not present with a true mesentery. However, sometimes a peritoneal fold called mesenteriole or mesentery of the appendix may be present. The characteristic features of large intestine namely the appendices epiploicae is not seen in caecum, appendix and rectum. During our routine cadaveric dissection, we came across a few specimens of appendix with appendices epiploicae.
Aim
To study the mesentery of the appendix and the presence of small Appendices Epiploicae in appendix macroscopically and microscopically.
Materials and Methods
During our routine cadaveric dissection, over a period of 5 years, we observed the appendix of 75 cadavers macroscopically for the presence of mesentery and appendices epiploicae. Simultaneously, during the same period 116 post-appendicectomy specimens that came to pathology department for reporting was studied macroscopically and microscopically for the same. The post-appendicectomy specimens were obtained from our institute Shri Sathya Sai Medical College and Research Institute, Kancheepuram.
Results
Appendices Epiploicae was observed macroscopically in 7 out of 75 cadaveric specimens and only microscopically in 76 out of 116 Appendix specimens removed at surgery.
Conclusion
This less reported finding is presented for its clinical importance, wherein presence of Appendices Epiploicae of Appendix can lead to torsion and inflammation of Appendix and can be considered in the differential diagnosis of acute abdomen.
Appendices epiploicae, Lymphoid infiltration, Mesentery, Torsion
Introduction
The vermiform appendix is a narrow, worm shaped tube, which springs from the postero-medial wall of the caecum, 2 cm or less below the end of the ileum. In view of its high vascularity and microanatomy, it may be more appropriately considered as a specialised rather than as a vestigial structure. Microscopically the layers of the appendix are serous, muscular, submucous and mucous towards the lumen. The serous coat forms a complete investment for the tube, except along the narrow line of attachment of its Mesentery (M) [1]. Since the appendix is a part of the caecum and the latter has no true mesentery, the appendix does not either; however, there is usually a peritoneal fold enclosing the artery to the appendix which is commonly referred to as the mesenteriole or mesentery of the appendix [2]. The mesentery attaches to the caecum as well as the proximal appendix. It contains the appendicular artery. The mesentery frequently appears to be too short for the appendix which may be sharply bent on itself [3].
Appendices Epiploicae (AE) is small peritoneal masses of protruding fat present everywhere in the large intestine except on the appendix, the caecum and the rectum [4]. They are of unknown function. They occur more frequently close to the taenia coli of colon [5]. The taenia coli are continuous with the longitudinal muscle of the appendix and on the caecum, ascending, descending and sigmoid colons are situated on their anterior, postero-lateral and postero-medial aspects. On the transverse colon, they occupy anterior, superior and inferior positions [4].
A very few cases have been reported in which fusion of two appendices epiploicae around the portion of the circumference of the large intestine has produced obstruction of it [6]. Partial obstruction due to intussusception of an appendix epiploica has also been reported [7]. Though references were available for the Appendices Epiploicae of large intestine there was a lacuna in references for Appendices Epiploicae of appendix. Search in literature reveals 3 studies [8-10] with reference to appendices epilploicae of appendix, of which in 2 studies, the torsion of appendices epiploicae of appendix presenting as acute abdomen was observed [9,10]. During our routine cadaveric dissection, a few specimens of appendix presented with appendices epiploicae. This instigated an interest to study the appendix and observe for the presence of appendices epiploicae and also extend to study the same in post-appendectomy specimens to understand its clinical importance. Hence, the present study was conducted with the aim to observe the mesentery of the appendix and the presence of small Appendices Epiploicae in appendix macroscopically and microscopically.
Materials and Methods
A descriptive cross-sectional study was carried out at Shri Sathya Sai Medical College, Hospital and Research Institute (SSSMC&RI), Kancheepuram, over a period of 5 years from 2012 to 2017. During our routine cadaveric dissection, over a period of 5 years we observed the appendix of 75 cadavers for the presence of mesentery and appendices epiploicae macroscopically. Simultaneously, during the same period, 116 post-appendicectomy specimens removed at surgery in our institute, that came to pathology department for reporting was studied macroscopically and microscopically for the same. Appendix specimens with intact epithelial lining and serosal covering were included in the present study. Ischaemic and necrosed appendix specimens were excluded from the study.
In the 75 cadavers, the presence and extent of mesentery, presence of appendices epiploicae and the number of rows of appendices epiploicae were observed macroscopically.
In the 116 post-appendectomy specimens, the presence of appendices epiploicae, number of rows of AE, relation of AE to thickened areas of muscle coat, presence of blood vessels and lymphoid infiltration in the wall of AE were observed microscopically.
Results
As appendices epiploicae are peritoneal outpocketings laden with fat, we observed the mesentery as well as the appendices epiploicae in the wall of the appendix, macroscopically in 75 cadaveric specimens. Of the 116 post-appendectomy specimens from pathology department, we did not observe appendices epiploicae in any of the 116 specimens macroscopically. Hence sections were prepared and stained with Eosin and Haematoxylin stain and the slides were observed microscopically under 10x magnification.
Macroscopic Findings
The following findings were observed macroscopically in 75 cadavers.
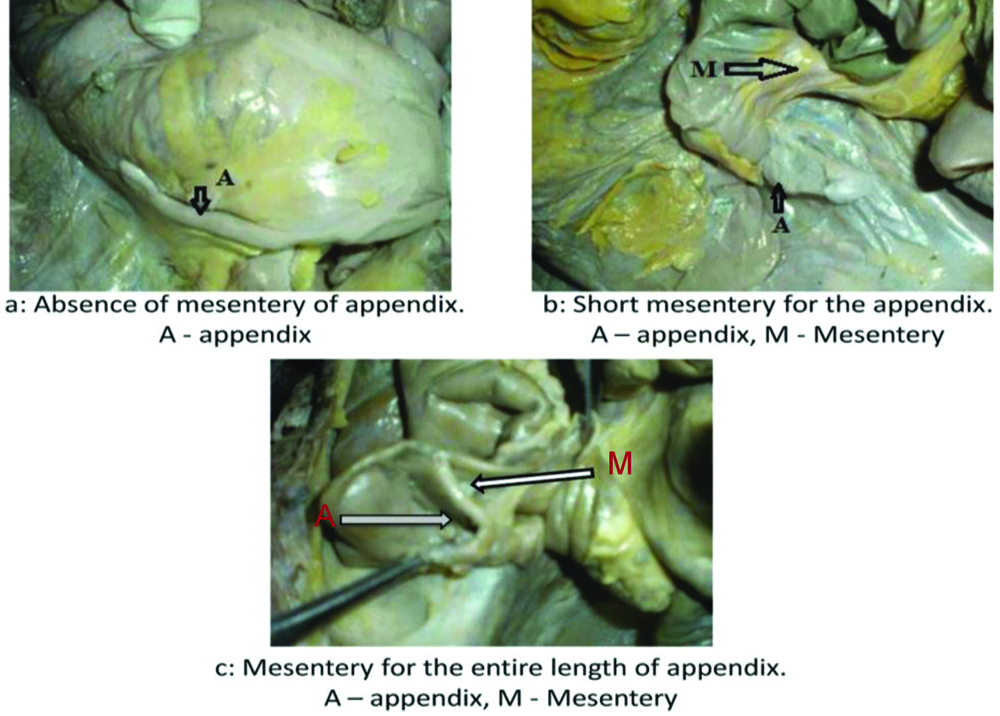
Mesentery was absent in the appendix of 12 cadavers [Table/Fig-1,2]. It was short (partial) in 29 cadavers. The mesentery extended along the entire length (complete) of the appendix in 34 cadavers.
Extent of mesentery in cadaver specimens of appendix.
| Mesentery of appendix | Findings observed in number of cadavers | Percentage |
|---|
| Complete | 34 | 45% |
| Partial | 29 | 39% |
| Absent | 12 | 16% |
Showing: (a) absent; (b) partial; and (c) complete mesentery.
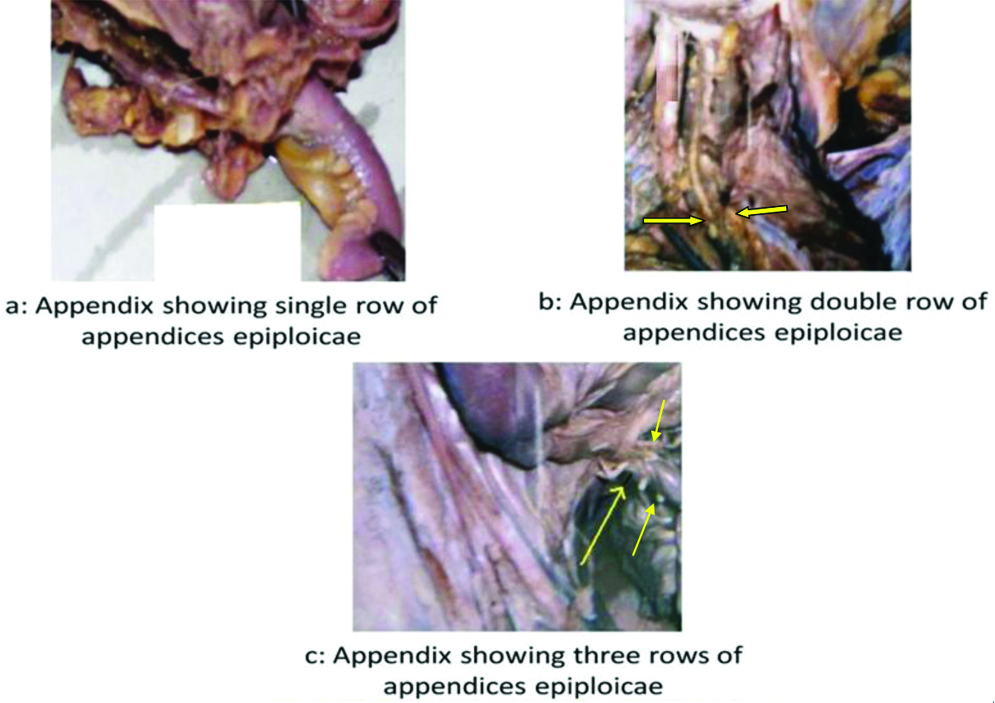
Appendices Epiploicae was seen in only 7 cadavers out of the 75 cadavers observed [Table/Fig-3]. Single row of appendices epiploicae was seen in appendix in 4 cadavers (13%). Two rows of Appendices epiploicae were observed macroscopically in 1 cadaver (3.3%). Three rows of Appendices epiploicae were seen in 2 cadavers (6.6%).
Showing: (a) single row; (b) double row; and (c) three rows of appendices epiploicae.
Microscopic Findings
Of the 116 appendectomy specimens observed, only 76 specimens showed the histological presence of appendices epiploicae. The following findings were observed in 76 specimens microscopically.
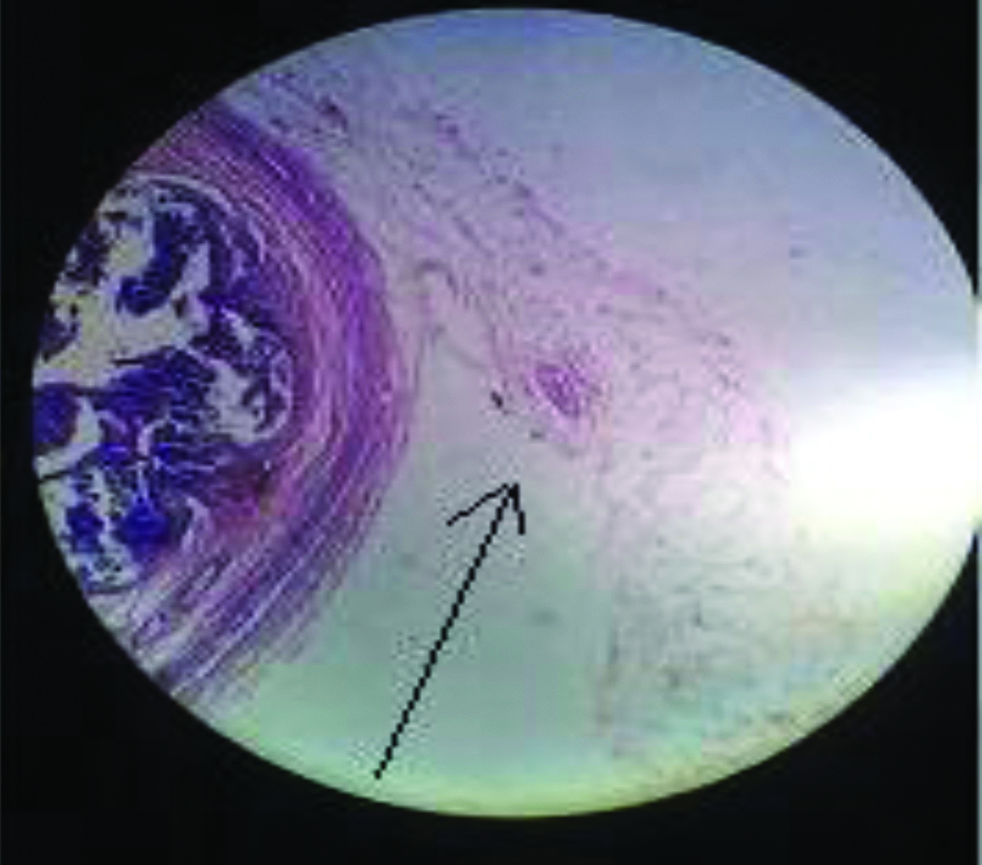
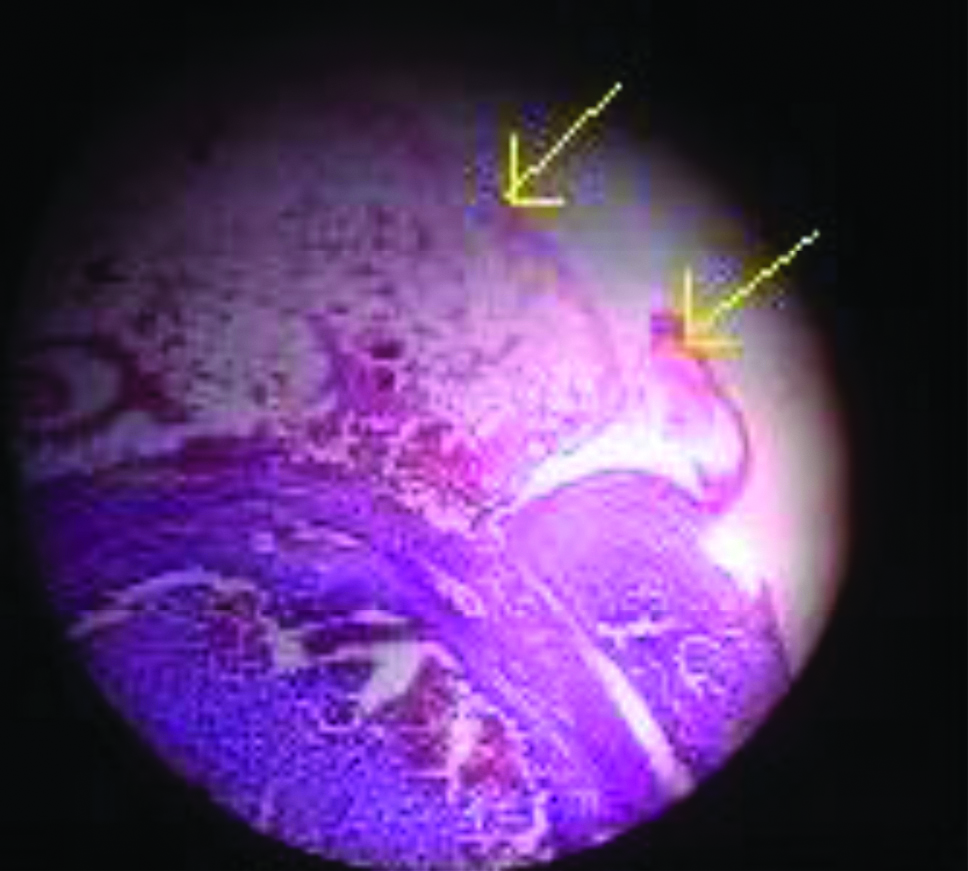
[Table/Fig-4] shows the histopathological findings in the 76 specimens which presented with appendices epiploicae. Single row of AE were present in 71 cases (61.2%) [Table/Fig-5], two rows of AE were present in 2 cases (1.7%) [Table/Fig-6] and three rows of AE were present in 3 cases (2.5%) [Table/Fig-7].
Number of rows of appendices epiploicae observed histopathologically.
| Rows of appendices epiploicae observed | Findings observed in number of slides | Percentage |
|---|
| Single | 71 | 61.2% |
| Double | 2 | 1.7% |
| Three rows | 3 | 2.5% |
Showing single row of appendices epiploicae (H&E stain, 10x magnification).
Showing double rows of appendices epiploicae (H&E stain, 10x magnification).
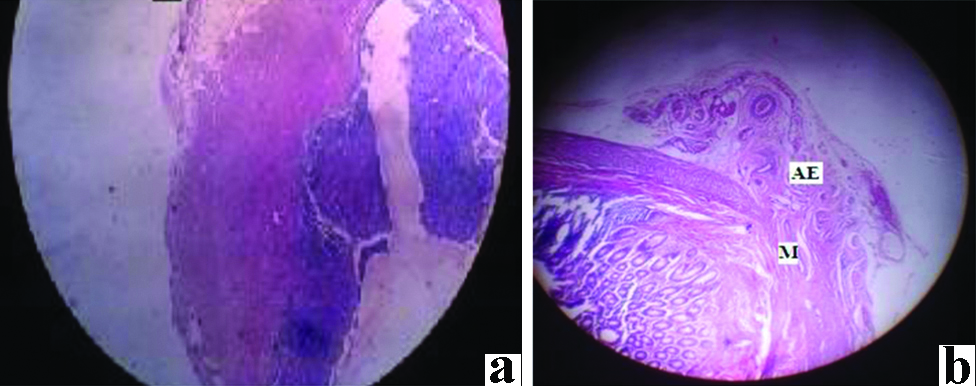
Showing (1,2&3) three rows of appendices epiploicae over thickened area of the muscle coat (H&E stain 10x magnification).

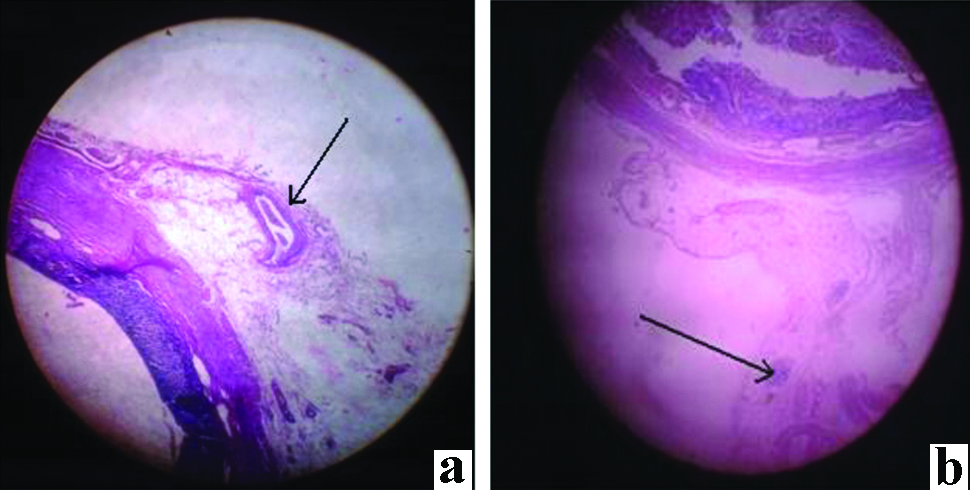
The AE were seen over thickened areas of the muscle coat [Table/Fig-8a] of the Appendix resembling taenia coli in 72 specimens (62%) and they were observed over thin areas of the muscle coat [Table/Fig-8b] in 3 specimens (2.5%) and over normal area in one specimen. The Appendices Epiploicae had blood vessels [Table/Fig-9a] in 34 specimens (29.3). In 8 specimens [Table/Fig-9b] (6.8%) lymphoid infiltration was seen.
a) AE were seen over thickened areas of the muscle coat; b) AE were seen over thin areas of the muscle coat (H&E stain, 10x magnification).
a) Appendices epiploicae showing blood vessels; b) Appendices epiploicae showing infiltration of lymphoid tissue in it (H&E stain, 10x magnification).
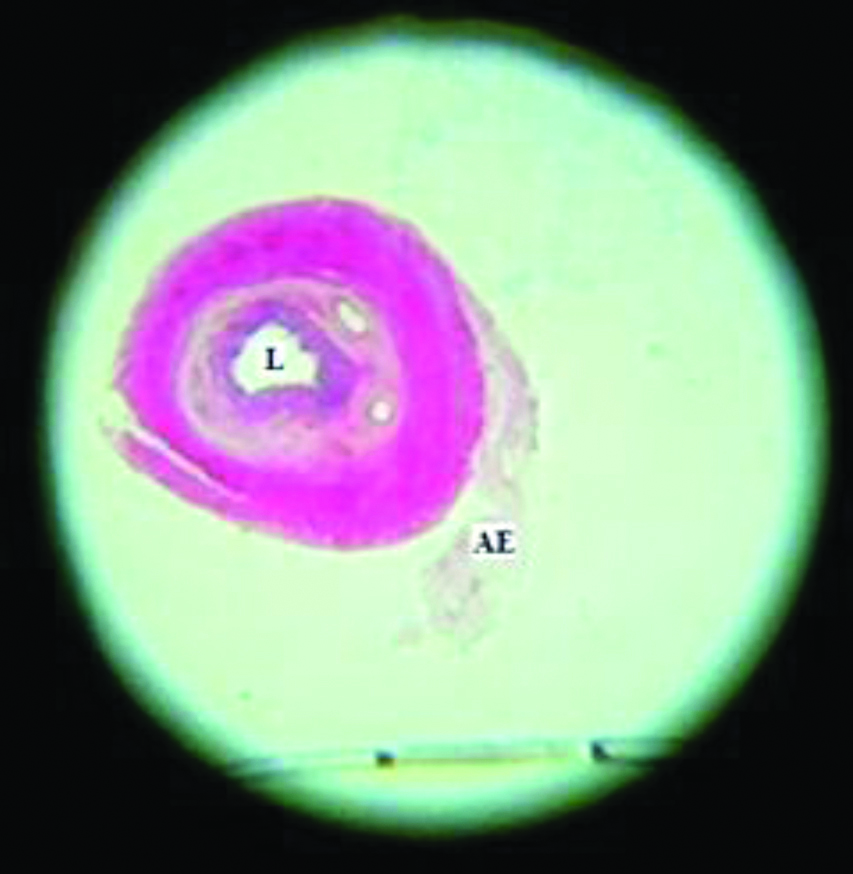
The Appendices epiploicae were from the serosal coat and was not extending from the lumen [Table/Fig-10]. This can be differentiated from diverticula which extend from lumen.
Transverse section of the lumen showing intact nature and only the serosa forming the Appendices epiploicae. L-Lumen (H&E stain, 10x magnification).
Discussion
In the present study, of the 75 cadaveric specimens observed macroscopically, mesentery was absent in the appendix of 12 cadavers, it was short (partial) in 29 cadavers and the mesentery extended along the entire length (complete) of the appendix in 34 cadavers. Of the 116 post-appendectomy specimens, no Appendices epiploicae could be observed macroscopically. In the same 116 specimens which were stained (H&E) and studied microscopically under 10X magnification, 76 specimens showed the histological presence of appendices epiploicae.
The presence of Appendices Epiploicae in Appendix has been reported very rarely, as in two studies, which reports the torsion of an Appendices Epiploicae present in Vermiform Appendix as a rare cause of acute abdomen [9,10]. According to Aslam MB et al., extensive omental adhesions due to previous surgery, diverticular disease or some congenital acquisition are the suggested causes of acquiring an appendix epiploica near the vermiform appendix [10]. The out-pocketing may be the site of inflammation, thrombosis and infarction causing an acute abdomen requiring investigation and surgery [11-13].
These small out-pocketings should not be mistaken for miniature diverticulae as they are only confined to the serosal covering and neither involves the lumen nor the mucosal lining. Diverticula of the appendix have been reported in previous studies [14-16]. According to Shehan JJ, the epiploic appendages are supplied by one or two small end arteries that branch from the vasa recta longa of the colon and are drained by a tortuous vein passing through its narrow pedicle. The limited blood supply in combination with a pedunculated shape and excessive mobility makes it susceptible to undergo torsion and ischaemic or haemorrhagic infarct [17].
Similar to the findings reported by Legome EL et al., in the absence of a mesentery, whenever there was chronic inflammation and oedema of the appendix, the stretched peritoneal covering may form small
out-pocketing which gets deposited with fat giving rise to microscopically seen Appendices Epiploicae as observed in the present study [11]. Also, in the present study, the presence of appendices epiploicae over thickened areas of the muscle coat is also in line with this hypothesis and was mostly observed in chronic appendicitis cases which also showed hypertrophy of lymphoid tissue.
Limitation
In the present study, the observation of appendices epiploicae was made for the first time in 2012 cadaveric dissection, during which importance was given only to the findings and latter this was extended to histopathological study of post-appendectomy specimens also. Hence details of inclusion and exclusion criterias along with data analysis have not been clearly mentioned in the study. Review of literature shows that these findings have very few references. Present work relating to the significance of appendix and its serosal covering may provide insight into the clinical significance of this lymphoid tissue.
Conclusion
When mesentery is absent, the blood vessels lie on the wall of the appendix and the thrombosis of these vessels can lead to inflammation. In chronic inflammation, the distension and oedema of the appendix stretches the serosal covering and when the inflammation subsides, it may form loose folds into which fat gets deposited to form appendices epiploicae. In them when blood vessel and lymphoid infiltration occurs they may be the cause for inflammation. These Appendices Epiploicae may even undergo torsion presenting as an acute abdomen.
Future Recommendation
Further cadaveric and histopathological studies may throw some light on the significance of these appendices epiploicae and whether these findings may need to be looked for and reported during rountine imaging techniques.
[1]. Williams PL, Warwick R, Splanchnology: The vermiform appendixGray’s Anatomy 1980 36th EditionLondon and EdinburghChurchill-Livingstone:1353 [Google Scholar]
[2]. Hollinshead WH, Anatomy for Surgeons: The Thorax, Abdomen and Pelvis 1956 vol. 2New YorkHoeber-Harper:493 [Google Scholar]
[3]. Skandalakis JE, Surgical anatomy: the embryological and anatomic basis of modern surgery 2004 volume 2International editionPaschalidis medical publications:851 [Google Scholar]
[4]. Romanes GJ, Cunningham’s Textbook of Anatomy, 12th edition. Edited by Romanes GJ 1981 OxfordOxford University Press:462 [Google Scholar]
[5]. Hollinshead WH, Anatomy for Surgeons: The Thorax, Abdomen and Pelvis 1956 vol. 2New YorkHoeber-Harper:487 [Google Scholar]
[6]. Baumeister C, Hargens CW, Morsman CP, Obstruction due to appendices epiploicaeAnn Surg 2007 107(1):153-54.10.1097/00000658-193801000-00021 [Google Scholar] [CrossRef]
[7]. Harte MS, Chronic partial intestinal obstruction due to intussusception of an appendix epiploicaSurgery 1943 13(4):555-60. [Google Scholar]
[8]. Ghahremani GG, White EM, Hoff FL, Gore RM, Miller JW, Christ ML, Appendices epiploicae of the colon: Radiologic and pathologic featuresRadiographics 1992 12(1):59-77.10.1148/radiographics.12.1.17344821734482 [Google Scholar] [CrossRef] [PubMed]
[9]. Iyer G, Seenu V, Bhat A, Sharma MC, Mathew R, Verma G, Torsion of Appendix epiploica: a rare cause of acute right iliac fossa painOman Med J 2010 25(1)10.5001/omj.2010.18 [Google Scholar] [CrossRef]
[10]. Aslam MB, Hasan N, Torsion of an appendix epiploicae present at the vermiform appendix: a rare cause of acute abdomenTurkish Journal of Trauma & Emergency Surgery 2009 15(5):509-10. [Google Scholar]
[11]. Legome EL, Bolton AL, Murray RE, Rao PM, Novelline RA, Epiploicappendagitis: The emergency department presentationJ Emerg Med 2002 22:9-13.10.1016/S0736-4679(01)00430-9 [Google Scholar] [CrossRef]
[12]. Barbier C, Denny P, Pradoura JM, Bui P, Rieger A, Bazin C, Radiologic aspects of infarction of the appendix epiploicaJ Radiol 1998 79:1479-85. [Google Scholar]
[13]. Diaco JF, Diaco DS, Brannan AN, Endoscopic removal of an infarcted appendix epiploicaJ Laparoendose Surg 1993 3:149-51.10.1089/lps.1993.3.149 [Google Scholar] [CrossRef]
[14]. Collins DC, Diverticula of the vermiform appendixAnn Surg 1936 104(6):1001-12.10.1097/00000658-193612000-0000617856883 [Google Scholar] [CrossRef] [PubMed]
[15]. Favara BE, Multiple congenital diverticula of the vermiform appendixAm J Clin Pathol 1968 49:60-64.10.1093/ajcp/49.1.604965687 [Google Scholar] [CrossRef] [PubMed]
[16]. Kugnanaeswaran E, Fisher JK, Giant sigmoid diverticulum: A rare manifestation of the diverticular diseaseSouthern Medical Journal 1998 91(10):952-55.10.1097/00007611-199810000-00011 [Google Scholar] [CrossRef]
[17]. Shehan JJ, Organ C, Sullivan JF, Infarction of the appendices epiploicaeAm J Gastroenterol 1966 46:469-76. [Google Scholar]