Shoulder impingement syndrome is a commonly seen shoulder disorder and it is amongst prime causative factor for persistent disability. Shoulder impingement syndrome is a problem for not only athletes. It’s likely a larger problem for people that are not athletes. This disorder affects the athlete in multipronged manner by creating functionality problems, economic issues and by decreasing the quality of life [1]. Approximately, one out of three patients are affected by shoulder pain which accounts for around 1% physician related visits [2,3]. The resultant disability from the shoulder disorder impairment is an important public health issue nowadays [4]. The prevalence of shoulder impingement ranges between 6-20% depending on the overhead sport being investigated [5-7]. Thus, it is clear that shoulder impingement syndrome is a dimension which merits consideration from clinical context.
A number of varied means can be utilised to examine the deficits caused by shoulder problems. In past as well as in present the patient assessment revolves around evaluating range of motion, pain and strength. Activity restriction evaluation is more important for the athletes which had been examined to lesser extent in past [8,9]. Recently, there has been a significant growth and development of patient rated shoulder rating measures [10-12]. Psychometric properties inclusive of validation, reliability and responsiveness have been examined for some of them. The SPADI is popular subjective shoulder measurement instrument. It was developed by Kathryn roach to quantify and subdivide the effect of shoulder pathologies/disorder into pain and disability [13]. The SPADI scale is undoubtedly the more popular and widely used scale for measurement of shoulder pathologies [14]. The SPADI has also been cross culturally validated into a number of other languages like Greek, Spanish, Thai, Tamil etc., [15-18]. However, the construct validity of Hindi SPADI for assessing overhead athletes has not been firmly established. In today’s world, there is lot of diversity of population and cultures living in the same region, hence it becomes imperative to develop and validate outcome scales in groups different from those used in the original scale.
To our knowledge, there is dearth of evidence with respect to validation of already existing Hindi language version SPADI [Annexure-1]. The literature review suggest that there are only two researches to validate a regional Indian languages (Tamil and Telugu) and these studies were conducted on general shoulder pain patients rather than on athletes with shoulder impingement syndrome [18,19]. In spite, of the presence of multiple linguistic versions of SPADI there are limited studies which have carried out CFA for these translated scales.
To retain the equivalency between the original and translated version, any outcome measure should undergo psychometric scrutiny which will help in examining its performance. The initial work demonstrated bi-dimensional model of original SPADI comprising the pain and disability constructs [13]. However, five factor solutions has been empirically demonstrated using Exploratory factor analysis (EFA) for the Hindi version SPADI scale [20]. Previous research has shown that there are several shortcomings associated with EFA approach when determining the validity of the latent constructs of a scale [21]. Thus, the primary purpose of the study was to test the theoretical structure of the Hindi SPADI via the CFA.
Materials and Methods
Design
This study was cross-sectional study which was performed in the physiotherapy department of the Jamia Millia Islamia, New Delhi. The study was performed from August 2014 to August 2017. This methodological study with quantitative approach was registered retrospectively under Clinical trial Registry of India (CTRI/2018/05/013892).
Participants
The sample size was based on power analysis (80%) where we considered at least 6 individuals for each item (question) of the scale. This gave a sample size of 78 participants (6 x 13 SPADI questions) [21]. Overhead athletes are those who participate in any overhead sports and their upper arm or shoulder arcs over the athlete’s head [22]. Overhead athletes were enrolled from the university physiotherapy clinic. The athletes had the shoulder impingement syndrome since at least one month. The shoulder impingement syndrome was confirmed clinically by following criteria where at least two out of five tests should be positive [23].
Positive neers sign: Neers sign is considered positive if the athlete’s reports pain while the examiner passively flexes the arm while it is internally rotated and scapula stabilised.
Positive hawkins sign: Hawkins sign is considered positive if the athletes reports pain while the examiner internally rotates the shoulder while keeping the shoulder and elbow in 90 degrees of flexion.
Positive jobes sign: Jobes sign is considered positive if the athletes reports pain or weakness with resistance while the examiner applies a downwardly directed force while the arm is in scaption and full internal rotation, elbow extended and forearm pronated.
Pain with apprehension test: Apprehension test is considered positive if the athlete reports pain while the examiner applies an external rotation force to the abducted shoulder held at 90 degrees and elbow flexed at 90 degrees.
Positive relocation test: Relocation test is considered positive if the athlete reports reduction in pain while the examiner applies posteriorly directed force to the shoulder which is held in position of apprehension.
The exclusion criteria for the study were: a) previous shoulder dislocation; b) Acromioclavicular (AC) joint pathology; c) prior surgery on the symptomatic side; d) cervical spine radiculopathy; e) positive drop arm test [23]. The research had been approved by the Institutional ethical committee (IEC) of the authors affiliated institution. A written informed consent was taken from all athletes fulfilling the inclusion criteria.
Procedure
The study was conducted at the physiotherapy department of the university. After applying the inclusion/exclusion criteria, 80 university overhead athletes diagnosed with shoulder impingement syndrome were recruited for the study and asked to complete the Hindi version SPADI questionnaire [24]. All the participants were assessed for demographic data (age, height, weight, affected side and sports discipline). Prior to administering the scale, all the participants were familiarised to the testing procedure. SPADI scale is a 13-item patient reported outcome questionnaire designed to assess the impairment and pain in patients with shoulder pathology. The items are classified into two categories pain and disability. Each item can be scored from 0 (no pain/no difficulty) to 10 (maximum pain/unable to do). The maximum score is 130 [13]. The time required to fill Hindi SPADI took around 20 minutes.
Statistical Analysis
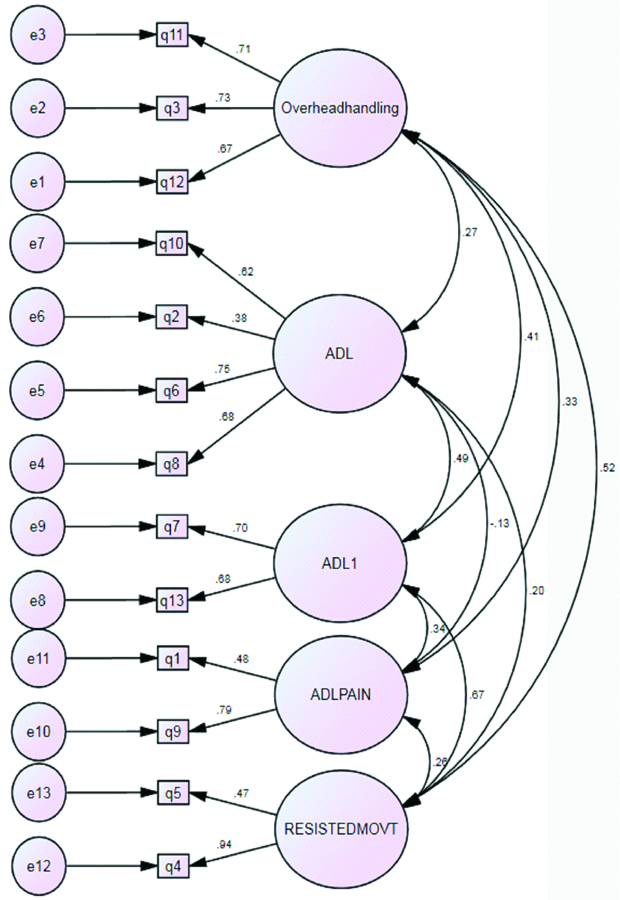
The CFA was performed with the help of SPSS AMOS 25.0 version (Armonk, NY, IBM Corp.) [Table/Fig-1]. Means±standard deviation, range, floor and ceiling effect were calculated as component of descriptive statistics. The floor and ceiling effects means that there is further inconsistency in the concept than our question(s) were able to determine. For a ceiling effect there would have been higher scores than we observed, but our measure did not extend far enough to capture them. Similarly in floor effect, there would be lower scores than we observed but our measure did not extend low enough to capture it. In this study, we kept the limits of floor and ceiling effects at 16% [25]. Univariate normality analysis for all the items of the scale was calculated using the skewness and kurtosis values. The distribution of respondent scores was also calculated to assess the variation in percentage of scores.
A CFA for the five factor model of the Hindi version SPADI (SPPS AMOS 25.0 Version) (n=80).
Construct validity (CFA): The five factors/domains explored by exploratory factor analysis in the Hindi version of SPADI scale were examined by CFA [20]. A number of goodness of fit parameters was examined: Comparative fit index (CFI), Goodness of fit index (GFI), Absolute goodness of fit index (AGFI), Root Mean Squared Error of Approximation (RMSEA) and chi-square/degrees of freedom. CFI, GFI, AGFI with the values greater than 0.80, RMSEA with a measure of less than 0.08 and chi-square/degrees of freedom value less than 3 were considered acceptable [26].
The standardised regression weight and factor loadings threshold cut-off value was taken at 0.3 or greater for each item [26]. This helped in deciding which items of the scale would be fit to be removed during CFA. CR was derived from factor loadings obtained from factor analysis. It is the square of the sum of loading variances obtained from extracted factors and dividing by sum of error variance and loading variances:
CR=(∑ factor loadings)2/(∑ factor loadings)2+∑(sum of error variance)…{1}Error variance is synonymous with Average variance extracted (AVE). It is calculated by subtracting squared factor loading from one.
Error variance extracted (AVE)=1-(factor loading)2…{2}As per the criteria, composite reliability values of 0.60 and greater and AVE of 0.50 or greater were considered acceptable [21,26,27].
Results
Demographic Characteristics and Normality of Data
A total of 80 participants were recruited for the study. All the participants were Hindi speaking male athletes. The average age was 21.50 years (SD=2.20), with an age range of 17-25 years. In terms of affected side, 64(80%) athletes had impingement syndrome of their right shoulder. In terms of their sports discipline background, 31.25% were cricket players, 30% volleyball players, 32.50% basketball players, 5% badminton players and 1.25% belonged to javelin sports The characteristics are summarised in [Table/Fig-2].
Descriptive characteristics (N=80).
| Demographic details mean |
|---|
| Age (years) | 21.50±2.20 |
| Range (age) | 17-25 |
| Affected shoulder (n) |
| Right | 64 (80%) |
| Left | (20%) |
| SPADI Total score (H) | 57.98±10.33 |
| Sports discipline (n) |
| Cricket | 25 (31.25%) |
| Volleyball | 24 (30%) |
| Basketball | 26 (32.5%) |
| Badminton | 4 (5%) |
| Javelin | 1 (1.25%) |
The mean±SD of Hindi SPADI score was 57.98±10.33. [Table/Fig-3] represents the means, standard deviation and the percentage of patients scoring at floor (zero) and ceiling levels (maximum possible score). There was no floor and ceiling effect as the proportions were less than 16% for all the factor domains. There was no missing data of the Hindi version SPADI. Skewness and kurtosis was investigated to determine the distribution of scores on the continuous variables. If the distribution is perfectly normal one would obtain skewness and kurtosis value of 0 (rather uncommon occurrence in the health sciences). The skewness value provides an indication of the symmetry of the distribution. The coefficient of skewness ranged from -0.626 to 0. 945. Reviews suggest that a skewness statistic between -1.0 and +1.0 would be regarded as acceptable [28]. The highest point of scores distribution is called as kurtosis. The coefficient of kurtosis was in the range of -0.730 to 1.522. The normative kurtosis statistic should be between -2.0 and +2.0.
The Mean±SD, score spectrum and number (%) of athletes reporting maximum score (ceiling effect) and lowest score (floor effect) for the Hindi version SPADI (n=80).
| Extracted factors | Mean | SD | Range | Floor effect n (%) | Ceiling effect n (%) |
|---|
| Overhead handling | 6.24 | 2.01 | 1-10 | 0 (0) | 12 (15) |
| ADL | 5.58 | 2.15 | 0-10 | 12 (15) | 4 (5) |
| ADL1 | 6.45 | 2.12 | 0-10 | 2 (2.5) | 5 (6.2) |
| ADL PAIN | 4.78 | 1.70 | 0-10 | 3 (3.7) | 3 (3.7) |
| Resisted movement | 6.38 | 2.03 | 1-10 | 0 (0) | 9 (11.2) |
Respondent score of Hindi SPADI
Response scores to the 13 item Hindi version SPADI scale ranged from 0(no pain/no functional limitation) to 10(maximum pain/maximum functional limitation). On a question-by-question basis, 2.5% (2/80) to 6.3% (5/80) of the 80 respondents stated a score of 0, while 2 (2.5) to 22 (28.3) stated a score of 5 and 2.5% (2/80) to 6.3% (5/80) stated a score of 10 [Table/Fig-4].
Distribution of respondent scores of the Hindi version SPADI (n=80).
| Items scores |
|---|
| 0, n (%) | 1, n (%) | 2, n (%) | 3, n (%) | 4, n (%) | 5, n (%) | 6, n (%) | 7, n (%) | 8, n (%) | 9, n (%) | 10, n (%) |
| Item 1 | 0 (0) | 0 (0) | 0 (0) | 3 (3.8) | 9 (11.6) | 22 (28.3) | 24 (28.8) | 22 (27.5) | 0 (0) | 0 (0) | 0 (0) |
| Item 2 | 0 (0) | 0 (0) | 1 (1.3) | 1 (1.3) | 3 (3.8) | 8 (10) | 17 (21.3) | 19 (23.8) | 17 (21.3) | 14 (17.5) | 0 (0) |
| Item 3 | 0 (0) | 1 (1.3) | 2 (2.5) | 4 (5) | 5 (6.3) | 6 (7.5) | 25 (31.3) | 14 (17.5) | 11 (13.8) | 9 (10.5) | 3 (4.7) |
| Item 4 | 0 (0) | 1 (1.3) | 3 (3.8) | 3 (3.8) | 8 (10) | 15 (18.8) | 17 (21.3) | 11 (13.8) | 11 (13.8) | 6 (7.5) | 5 (6.3) |
| Item 5 | 0 (0) | 1 (1.3) | 1 (1.3) | 2 (2.5) | 8 (10) | 13 (16.3) | 15 (18.8) | 10 (12.5) | 12 (15) | 14 (17.5) | 4 (5) |
| Item 6 | 4 (5) | 2 (2.5) | 3 (3.8) | 8 (10) | 7 (8.8) | 13 (16.3) | 13 (16.3) | 16 (20) | 7 (8.8) | 5 (6.3) | 2 (2.5) |
| Item 7 | 0 (0) | 3 (3.8) | 3 (3.8) | 0 (0) | 9 (11.3) | 8 (10) | 15 (18.8) | 19 (23.8) | 12 (15) | 6 (7.5) | 5 (6.3) |
| Item 8 | 3 (3.8) | 3 (3.8) | 4 (5) | 8 (10) | 7 (8.8) | 16 (20) | 13 (16.3) | 7 (8.8) | 7 (8.8) | 10 (12.5) | 2 (2.5) |
| Item 9 | 3 (3.8) | 5 (6.3) | 17 (21.3) | 27 (33.8) | 12 (15) | 8 (10) | 4 (5) | 0 (0) | 3 (3.8) | 1 (1.3) | 0 (0) |
| Item 10 | 5 (6.3) | 4 (5) | 6 (7.5) | 7 (8.8) | 17 (21.3) | 13 (16.3) | 11 (13.8) | 10 (12.5) | 7 (8.8) | 0 (0) | 0 (0) |
| Item 11 | 0 (0) | 0 (0) | 5 (6.3) | 6 (7.5) | 7 (8.8) | 12 (15) | 15 (18.8) | 14 (17.5) | 12 (15) | 4 (5) | 5 (6.3) |
| Item 12 | 0 (0) | 0 (0) | 4 (5) | 1 (1.3) | 19 (23.8) | 2 (2.5) | 16 (20) | 16 (20) | 9 (11.3) | 9 (11.3) | 4 (5) |
| Item 13 | 2 (2.5) | 3 (3.8) | 2 (2.5) | 2 (2.5) | 17 (21.3) | 6 (7.5) | 22 (27.5) | 13 (16.3) | 6 (7.5) | 7 (8.8) | 0 (0) |
CFA and Fit Indices
The five factor structure model suggested by exploratory factor analysis was tested by confirmatory factor analysis. Following the identification of the model, we assessed the universal fit focusing on the quality of the model using the statistical package. Hindi version SPADI was subjected to CFA using Structural equation modelling (SEM). [Table/Fig-3] illustrates the observed items and unobserved factors synthesised through CFA, with standardised regression weights ranging from 0.94 to 0.38. The relative chi-square was 73.841, indicative of acceptable fitness of the model (p=0.05). All comparative fit indices in the model: CFI, GFI, AGFI were greater than 0.80(0.913, 0.872, 0.80 respectively), showing excellent goodness of fit for the data [Table/Fig-5]. The models RMSEA value was 0.065 {95% Confidence interval (CI) (0.009-0.102}, also suggesting an acceptable fit for Hindi SPADI scale. This is a frequently utilised means to examine model fitness and it works as separate entity on comparison with other fit indices. The cut off point for an acceptable RMSEA index is ≤0.065. Our model has the RMSEA less than the above mentioned value hence demonstrating fit acceptability.
GFI in the confirmatory factor analysis of the Hindi version SPADI for all the sample (n=80).
| GFI | Factors |
|---|
| χ2 | 73.84 |
| df | 55 |
| χ2/df | 1.343 |
| p | 0.06 |
| CFI | 0.913 |
| GFI | 0.872 |
| AGFI | 0.80 |
| RMSEA (95% CI) | 0.065 (0.009-0.102) |
| P CLOSE | 0.248 |
*CFI: Comparative fit index, CI: Confidence interval, GFI: Goodness of fit index, AGFI: Absolute goodness of fit index, RMSEA: Root mean square error of approximation, P CLOSE: Fit Indices in Confirmatory Factor Analysis, p=level of significance <0.05, χ2: chi-square, df: degree of freedom
Reliability Analysis
The reliability analysis showed that each construct/Factor loading had a good measure of reliability as the coefficient values are above the threshold values of 0.60 and 0.50 for composite reliability and average variance extracted. The composite reliability is considered to a better indicator of the reliability of the scale as it derived from the composed values of sum of factor extracted and error variance [Table/Fig-6].
Confirmatory factor analysis factor loadings, Composite reliability (CR) and Average variance extracted (AVE) of the Hindi version SPADI scale.
| Construct | Items | Factor loading | CR (≥0.6) | AVE (≥0.5) | CA |
|---|
| Overhead handling | q 11 | 0.71 | 0.74 | 0.50 | 0.74 |
| Q 3 | 0.73 | | | |
| Q 12 | 0.67 | | | |
| ADL | q 10 | 0.62 | 0.70 | 0.61 | 0.70 |
| q 2 | 0.38 | | | |
| q 6 | 0.75 | | | |
| q 8 | 0.68 | | | |
| ADL1 | q 7 | 0.70 | 0.64 | 0.50 | 0.70 |
| q 13 | 0.68 | | | |
| ADL pain | q 1 | 0.48 | 0.60 | 0.50 | 0.70 |
| q 9 | 0.79 | | | |
| Resisted movement | q 5 | 0.47 | 0.68 | 0.55 | 0.70 |
| q 4 | 0.94 | | | |
*q1 to q10 (questions/items of Hindi SPADI scale); **CA-Cronbach’s alpha
Chi-Square value
The Chi-square significance was taken at p<0.05 for the chi-square. However, the good model fit is suggested if p-value is non-significant, While, significant p-value denotes non-acceptable model solution. In our study, the chi-square was non-significant at 73.84 based on 55 degrees of freedom (p=0.05) for the subjects. The chi-square/degrees of freedom ratio were found to be 1.343 [Table/Fig-5]. Chi-square values of <3 was considered for the model acceptance. The result of the study demonstrated the chi-square ratio of 1.345 which can be concluded as good fit.
Discussion
This is the first study using confirmatory factor analysis for establishing the factor structure proposed by the exploratory factor analysis. CFA is used to verify the extracted factor units of measurement instrument. Eighty individuals completed the Hindi SPADI and this was followed by statistical analysis of the instrument reliability, item statistics and confirmatory factor analysis.
Reliability Analysis
The reliability analysis yielded an acceptable result. The result of composite reliability of the derived subscale was found to be in range of 0.60 to 0.74 for overhead handling, ADL activities, ADL1 activities; ADL activity related Pain and resisted movement. Past research has concluded that alpha in divisioned scale to be in the spectrum of 0.7 to 0.8 to indicate acceptable reliability [15-18,20,29]. The subscale reliability results moderately to strongly agree with earlier studies carried out on this instrument which provides evidence for the reliability of this scale. The result demonstrates a structural validity of the scale through the sub factor analysis.
CFA and Fit Indices
The result of the current study is in accordance with study exploring the Spanish version of SPADI where also the correlation between the two factors was 0.78 (p<0.001) [30]. The indices of goodness of fit helped determine the type of model fit (where a value of 0.80- 0.90 was considered a good fit). CFI, GFI and AGFI values suggested a good model fit for the model. The five-factor solution also received acceptance with RMSEA value [31]. The non-significance of the chi-square concluded a good model fit [32-34]. These findings correlate with the truncated item scale (ten questions) a two-factor solution, suggested in the Spanish version of SPADI. In this study, the questions number 1, 11, 12 were found to have poor correlations, henceforth they were deleted from item list to achieve best fit indices. Although in the current study we did not have to use modification indices to achieve best fit, but there was deviation in factor structure from the original English version SPADI [13,30].
Strengths
A major strength of the present study was the use of confirmatory analysis which allowed for a critical psychometric analysis beyond that possible with classical theory alone. Secondly the group was homogenous i.e., subjects with specific diagnosis and same playing characteristics were only recruited which increases its generalisability.
Limitation
There are few limitations of this study. Firstly, the data was gathered from a single university clinic. This could limit the generalisability of the results because of single source derivation of data hence proving a threat to external validity. Secondly, divergent validity and responsiveness of scale have not been determined.
Future recommendation: Further studies, to evaluate participants with different shoulder disorders and multicentre trials are needed. Further research to investigate Hindi version SPADI may be needed for more definite conclusions.
Conclusion
To summarise, the thirteen questions/items Hindi version of SPADI with the five factor solution exhibited an acceptable degree of fit indices and was found to be reliable tool for Hindi speaking shoulder impingement syndrome overhead athletes. The factorial structure would help the clinician to identify in which domains of the scale an athlete is most and least affected. This could direct clinical decision making accordingly.
This study helps to contribute to research by addressing the factorial structure of Hindi SPADI and favour the monitoring of overhead athletes with shoulder impingement syndrome within the care model of the health delivery system.