Dengue is most widely spread vector-borne disease which is a major public health threat globally. The disease is caused by four serotypes of dengue virus belonging to Flavivirus genus: DENV-1, DENV-2, DENV-3, and DENV-4 which are transmitted by infected Aedes mosquitoes species in tropical and subtropical regions. World Health Organisation (WHO) had classified the symptomatic dengue virus infection into Dengue Fever (DF), Dengue Haemorrhagic Fever (DHF) and Dengue Shock Syndrome (DSS) in 1997 [1]. Later in 2009, WHO has categorised the dengue patients according to the severity of clinical manifestations such as dengue without warning signs, dengue with warning signs (abdominal pain, vomiting, mucosal bleeding, fluid accumulation, lethargy, liver enlargement, increased hematocrit with decreasing platelets) and severe dengue [2,3]. Dengue is endemic in more than 100 countries and the majority of cases are reported from the America, South-East Asia and Western Pacific regions. Approximately, 390 million cases of dengue infection are reported every year and nearly 2.5 billion people are at risk for infection worldwide, with no vaccine or antiviral approved to reduce disease burden [1,2].
Dengue is endemic in almost all states of India and has become a leading cause of hospitalisation. Few decades earlier, dengue fever had a predominant distribution in urban areas, but in the current scenario it is also frequently reported from peri-urban as well as rural areas [4-6]. In India, the surveillance for dengue fever is being conducted through the National Vector Borne Disease Control Program (NVBDCP) comprising a network of more than 600 sentinel hospitals, Integrated Disease Surveillance Program (IDSP) and a network of 52 Virus Research and Diagnostic Laboratories (VRDL) established by Department of Health Research-Indian Council of Medical Research (DHR-ICMR) [6,7]. The detection of dengue cases, management of these cases and control of their vector are the main approaches of the program. An estimated 33 million cases had occurred in our country in 2010 [8,9]. The NVBDCP reported more than 100,000 laboratory confirmed cases of dengue in 2016 [7]. The high disease burden, endemicity, and frequent outbreaks are the serious cause of drain of country’s economy and stress on the health systems. Although systematic improvements are being made, however current gaps in epidemiological data and surveillance implies that the burden of dengue in India probably is much more higher [9]. Moreover, data related to its exact incidence in many parts of India is still lacking [9].
Accurate and affordable diagnostic tests are a crucial factor in combating this devastating vector-borne infection. These tests would allow timely diagnosis of dengue which leads to clinical management of patients. Differential diagnosis on the basis of clinical manifestation is very challenging due to the symptoms such as fever, aches and fatigue may usually overlap with other infections. However, mortality due to the dengue can be decreased from 20-30% to less than 1% by proper fluid intake with supportive care, which is significantly assisted by early and accurate diagnosis [10,11].
Detection of viral RNA using Reverse Transcription Polymerase Chain Reaction (RT-PCR), virus isolation and further immunofluorescence Assay (IFA) are the conventional methods used in diagnosis of dengue. However, all the methods are useful only during the initial five days of disease. So, their sensitivity also decreases as the viremia dimnishes with time [12,13]. Moreover, RT-PCR requires costly reagents, kits, instruments and trained personnel, while virus isolation is tedious and takes 5-15 days to complete. Enzyme-Linked Immunosorbent Assay (ELISA) is the most widely used method for the diagnosis of dengue that detects IgM or IgG antibodies against the dengue virus in patient serum. However, these antibodies are undetectable within the 3-4 days Post Symptom Onset (PSO) [10,14] and a second blood sample between 5-15 days is required for a definitive diagnosis. Thus, antibodies based diagnosis is unable to provide instant management decisions during acute illness. Several molecular assays have been developed for the detection of nucleic acid of dengue virus during the acute phase of illness [15]. These molecular or RT-PCR assays have several limitations to perform in resource constraint settings and are not available in point-of-care format [10].
On the other hand, other new assays are being developed or available in the market for diagnosis of dengue during the acute illness. In 2000, a new ELISA based on the capability of detection of dengue virus Nonstructural Protein-1 (NS1) antigen was developed. NS1 antigen is a highly conserved marker for dengue virus and is found in both membrane and is soluble [16]. During the dengue virus infection, NS1 antigen, a soluble hexameric form of it is released which accumulates in high concentrations (up to 50 mg/mL) in human serum [17]. It is detectable on the first day of fever of both primary and secondary dengue infections before the appearance of IgM antibodies [18]. Hence, the importance of NS1 antigen levels in clinical samples is an attractive target for diagnostic assay development [19]. Recently, NS1 tests have also been found to be effective for detection of dengue virus in vector populations [20,21]. Thus, these tests may play a potential role in both clinical management and vector surveillance program [14,22].
Considering the above points, the aim of this study was to examine the diagnostic efficacy of two commercially available dengue NS1 and IgM ELISA tests and to know the incidence of laboratory-confirmed dengue cases among clinically suspected patients. The present study also report the prevalence of the dengue fever outbreak in the Bundelkhand region in the 2018. This study adds the evidence-based data to the literature which would assist NVBDCP and community in order to know the current epidemiology to prevent and control this devastating vector-borne infection.
Materials and Methods
Study Settings
The study was conducted at Department of Microbiology, Maharani Laxmi Bai Medical College (MLBMC), Jhansi, Uttar Pradesh, India, a tertiary care hospital in Bundelkhand region. The department is recognised as a referral center under the IDSP program. The study was based on the data collected between January 2018 and December 2018 which were analysed retrospectively. All the samples which were submitted to the laboratory for dengue diagnosis as routine patient care service were included in the study. A total of 1794 blood samples of suspected dengue patients over the year 2018 (January to December) from the OPD/Wards of Medical College and nearby hospitals of Bundelkhand region sent to our department for routine dengue diagnosis were included in the study. The relevant clinical details were noted at the time of the sample receiving.
Serum separation: All the blood samples were collected in plain vials by venipuncture and were processed within 2-3 hours of collection. Samples were centrifuged at 4000 rpm for 5 minutes. Serum was collected with the help of sterile pipette and used for the ELISA testing [10].
ELISA Testing for Detection of NS1 Antigen
ELISA testing for the detection of dengue NS1 antigen was performed by using the commercially available “RecombiLISA Dengue Ag ELISA kit” as per the manufacturer’s instructions (CTK Biotech, Inc., San Diego, CA). The test is based on the principle of solid-phase sandwich ELISA for the qualitative detection of dengue NS1 antigen in serum or plasma. The kit contains a solid 96 microwells pre-coated plate with rabbit anti-pan dengue NS1 antibody and liquid conjugates having monoclonal antibodies against NS1 antigen conjugated with Horseradish Peroxidase (HRP) {HRP-anti-dengue NS1 Conjugates}.
During the assay, 50 μL of sample diluent was added into each well and 50 μL test serum into the respective test well. In the control wells, 50 μL of dengue NS1 positive control and 50 μL dengue NS1 negative control was added into the designated wells respectively. After gently shaking the wells for 20 seconds and covering the wells with a sealer, it was incubated at 37°C for one hour to bind the dengue NS1 antigen to the antibody coated on the microwell surface. Then after, test plate was washed 5 times with wash buffer by using the automated washer (AM 2600 microplater washer, Alere) to remove the unbound antigen. Hundred microliters of HRP-anti-dengue NS1 conjugates was added into each well and further incubated at 37°C for one hour. The unbound conjugates complex was then removed by washing the plate 5 times. After washing, 50 μL of 3,3’,5,5’-Tetramethylbenzidine (TMB) substrate A and B were added into each well which allows the development of a blue color resulting from a reaction between the enzyme and substrate in the presence of the conjugate complex in a positive reaction. This reaction was stopped by adding 100 μL stop solution (0.16M sulfuric acid) into each well. The absorbance (OD) was measured at 450 nm by using spectrophotometer (AM 2100 microplate reader, Alere).
Testing of IgM ELISA
Dengue IgM ELISA was performed by using “National Institute of Virology (NIV) dengue IgM capture ELISA kit” as per the manufacturer’s protocol (Kit insert, ICMR-NIV, Pune, India). The kit was developed by National Institute of Virology, Pune-ICMR in 1984 and its performance was evaluated by Christian Medical College (CMC), Vellore in 2002. The kit is based on IgM Antibody Capture (MAC) ELISA principle, intended for the qualitative detection of IgM antibodies present in human serum or plasma. For the testing, 50 μL diluted serum sample (1:100) was added into the prewashed anti-human IgM coated well. In the control wells, 50 μL of dengue IgM positive control and 50 μL dengue IgM negative control was added into the designated control wells, respectively. The plate was covered with aluminum foil to prevent evaporation of samples. The plate was kept in a closed humidified box (A bread box with a soaked cotton/tissue paper) inside the incubator and incubated the plate at 37°C for one hour. At the end of incubation, washing the plate five times with wash buffer was done. Tapped the plate after last wash on a tissue paper to remove traces of wash buffer content. Then after, 50 μL of dengue antigen was added into each well and incubated again at 37°C for one hour as same above. After the incubation, 50 μL of avidin-HRP was added to each well and incubated again at 37°C for 1 hour as same above followed by five times washing. After washing, 100 μL of Liquid TMB substrate was added to each well and incubate the plate at room temperature in Dark for 10 minutes. The reaction was stopped after 10 minutes with the addition of 100 μL stop solution. The absorbance at 450 nm within 10 minutes of reaction termination was measured.
Quality Control
Quality control of testing was maintained as per kit protocol. Each kit contains one vial of “Positive control” and one vial of “Negative control”. These work as marker of kit performance. If OD of the negative control is more than 0.18 or If OD of the positive control is less than 6 times the OD of negative control. In both situations, the test was considered invalid and was repeated.
Interpretation of Results
The results were interpreted as per kit protocols. If OD value of sample tested was less than OD of negative control by a factor 2.0 (sample OD ≤ negative control OD x 2.0), the sample was considered as “Negative”. If OD value of sample tested exceeds OD of negative control by a factor 3.0 (sample OD ≥ negative control OD x 3.0), the sample was considered as “Positive”. If OD value of sample tested exceeds OD of negative control by a factor 2.0 (sample OD ≥ negative control OD x 2.0) but was less than OD of negative control by a factor 3.0 (sample OD ≤ negative control OD x 3.0), the sample should be considered as “Equivocal”.
Results
The total 1794 clinical samples of suspected dengue cases were included in the study. Of them, 1014 (56.52%) were males and 780 (43.47%) females. Majority {1344 (74.9%)} of patients were more than 15 years of age with the mean age of 29.2±12.8 while 450 (25.1%) patients were aged less than 15 years with mean age of 9.1±3.72. Of the 1344 adult cases, 759 (56.47%) were males within age range of 16 to 76 (28.9±12.4) years and remaining being females 585 (43.5%) within age range of 17 to 81 (29.8±13.5) years. Out of 450 paediatric cases, 255 (56.67%) were boys with the mean age of 9.1±3.6 years followed by girls {195 (43.3%)} with the mean age of 9.0±3.8 years. Similar to the adult group, the percentage of male cases were higher in paediatrics group also. However, no major difference was observed in male to female ratio between both the groups. As a tertiary care hospital, MLB Medical College, Jhansi attends the patients from a different part of the Bundelkhand region and other nearby areas. In the present study, blood samples were received from the patients who hailed from different districts [Table/Fig-1]. District wise distribution the patients showed that majority of the patients (1361; 75.86%) were resident from Jhansi followed by Jalaun (99; 5.51%), Lalitpur (69; 3.85%); Datia (57, 3.06%), Tikamgarh (50; 2.78%), Shivpuri (31; 1.7%), Mahoba (30; 1.67%), Hamirpur (24; 1.3%), Chatarpur (20; 1.14%), Banda (19; 1.05%) and 34 (1.8%) cases were from Niwari, Kanpur, Chitrakut, Bhind, Agra, Gwalior and Jaunpur combinedly. Moreover, similar to the above distribution, the maximum incidence of dengue was observed in Jhansi (38.8%), followed by Lalitpur (37.6%), Banda (26.3%) and Jalaun (20.2%) [Table/Fig-1,2]. The geographical distribution of dengue cases from the different district of Bundelkhand region have been illustrated in [Table/Fig-2].
District-wise distribution of the cases.
| Districts | Number of cases (%) | NS1 ELISA +ve (%) | IgM ELISA +ve (%) | Total lab confirmed dengue cases (NS1 and/ or IgM ELISA +ve (%) |
|---|
| Banda | 19 (1.059) | 3 (15.78) | 2 (10.52) | 5 (26.3) |
| Chatarpur | 20 (1.14) | 1 (5) | 1 (5) | 2 (10) |
| Datiya | 57 (3.06%) | 7 (12.72) | 4 (5.45) | 9 (15.7) |
| Hamirpur | 24 (1.337) | 5 (20.83) | 1 (4.16) | 5 (20.8) |
| Jalaun | 99 (5.51) | 11 (11.11) | 11 (11.11) | 20 (20.2) |
| Jhansi | 1361 (75.86) | 378 (27.77) | 179 (13.55) | 529 (38.8) |
| Mahoba | 30 (1.67) | 3 (10) | 1 (3.33) | 4 (13.3) |
| Tikamgarh | 50 (2.78) | 3 (6) | 4 (8) | 7 (14) |
| Shiv Puri | 31 (1.727) | 6 (19.35) | 4 (12.90) | 10 (32.2) |
| Lalitpur | 69 (3.85) | 21 (30.4) | 15 (21.7) | 26 (37.6) |
| Other districts* | 34 (1.9) | 7 (20.3) | 1 (2.9) | 8 (23.5) |
| Total | 1794 | 445 (24.8) | 223 (12.4) | 625 (34.8) |
*Niwari, Kanpur, Chitrakut, Bhind, Agra, Gwalior and Jaunpur combinedly
Geographic distribution of dengue cases from different districts of Bundelkhand region (map adopted from http://www.bundelkhandtourism.in/).

Fever was the most common clinical manifestation in the suspected dengue patients. Of them, majority of patients (1002; 55.97%) had the complaint of fever for 1-5 days while 573 (31.33%) patients for 6-10 days and 219 (12.20%) patients had fever for more than 10 days. Decreased level of platelets count was observed in 1219 (68%) patients.
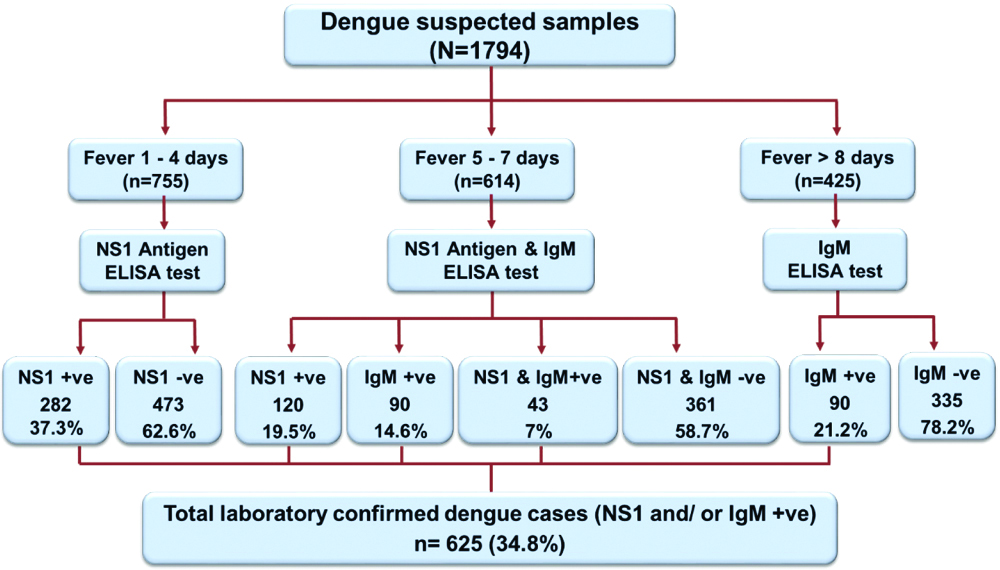
A total of 1369 (76.25%) patient’s samples that were reported with the complaint of fever for 1-7 days were tested by NS1 ELISA for the diagnosis of dengue. Of them, 445 (32.5%) samples were found to be positive (402 samples were positive for NS1 only and 43 samples were positive for both NS1 and IgM) and 924 (67.4%) were negative against the NS1 antigen [Table/Fig-3]. On the clinical correlation, all the patients which were positive for NS1 antigen their platelet counts were also found to be lower than the normal range.
The patients who had fever for more than 7 days were tested for dengue IgM ELISA. Out of 425 samples tested for dengue IgM antibodies, 223 (52.47%) were positive and 202 (47.5%) negative by IgM ELISA. A total of 614 patients had fever from 5 to 7 days these were tested for both NS1 and IgM ELISA. Of them, 120 (19.5%) were NS1 positive and 90 (14.5%) were IgM positive while 43 (7%) were found to be positive by both the tests (NS1 and IgM ELISA). Hence, 120 (19.5%) samples which were IgM negative were picked up by NS1 ELISA while 14.5% NS1 negative samples were detected as positive by IgM ELISA [Table/Fig-3]. Thus, out of 1794 cases, 625 (34.8%) patients were found to be dengue positive by NS1 and/ or IgM dengue ELISA. The present study has demonstrated that the use of NS1 antigen-based ELISA in combination with IgM ELISA can enhance the sensitivity of dengue diagnosis in all stages of the disease. The overall detailed comparative results of these tests are shown in the [Table/Fig-4]. The lower platelet count was observed in all the ELISA positive samples.
Clinical correlation of NS1 and IgM ELISA tests results with the status of fever.
| Fever (in days) | Number of cases | NS1 | IgM | NS1 and IgM | Total |
|---|
| 1-4 | 755 | 282 (37.3) | - | - | 282 (37.3) |
| 5-7 | 614 | 120 (19.5) | 90 (14.5) | 43 (7) | 253 (41.2) |
| >8 | 425 | | 90 (21.1) | | 90 (21.1) |
| Total | 1794 | 402 (22.4) | 180 (10) | 43 (2.3) | 625 (34.8) |
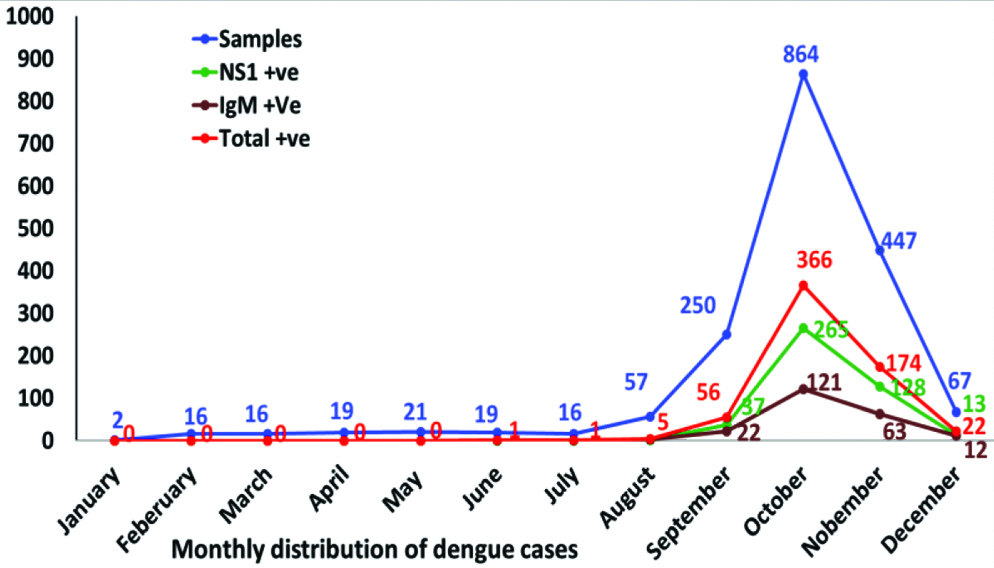
The month-wise distribution of the dengue cases has mentioned in [Table/Fig-5,6]. In the present study, the first dengue ELISA positive case of 2018 was detected in the last week of June. The highest positivity rate was observed in October (42.3%), followed by November (38.9%), December (32.8%), September (22.4%), August (8.7%), July (6.2%) and June (5.2%). However, no sample was found to be dengue serology positive from January to May. Similarly, the maximum number of specimens was also received in October (864; 48.1%), followed by November (447; 24.9%). Gender and age-wise analysis of laboratory-confirmed dengue cases showed that the percentage of male and adult cases was higher among ELISA positive cases. However, a similar pattern of NS1 and IgM ELISA positivity rate was observed in both the adult and paediatric group [Table/Fig-7].
Monthly distribution of dengue cases.
| Months (n) | NS1 ELISA | IgM ELISA | Both NS1 and IgM ELISA | Total NS1 +ve | Total IgM +ve | Total dengue cases confirmed by ELISA |
|---|
| n | +ve | n | +ve | n | NS1+ve | IgM +ve | NS1 and IgM+ve |
|---|
| January (2) | 2 | - | - | - | - | - | - | - | - | - | - |
| February (16) | 16 | - | - | - | - | - | - | - | - | - | - |
| March (16) | 16 | - | - | - | - | - | - | - | - | - | - |
| April (19) | 19 | - | - | - | - | - | - | - | - | - | - |
| May (21) | 17 | - | 2 | - | 2 | - | - | - | - | - | - |
| June (19) | 14 | - | 2 | - | 3 | - | 1 | - | - | 1 | 1 (5.2) |
| July (16) | 9 | - | 6 | 1 | 1 | - | - | - | - | 1 | 1 (6.2) |
| August (57) | 22 | 1 | 19 | 1 | 16 | 1 | 2 | - | 2 | 3 | 5 (8.7) |
| September (250) | 102 | 23 | 80 | 8 | 68 | 11 | 11 | 3 | 37 | 22 | 56 (22.4) |
| October (864) | 325 | 170 | 193 | 50 | 346 | 75 | 51 | 20 | 265 | 121 | 366 (42.3) |
| November (447) | 191 | 82 | 107 | 24 | 149 | 29 | 22 | 17 | 128 | 63 | 174 (38.9) |
| December (67) | 22 | 6 | 16 | 6 | 29 | 4 | 3 | 3 | 13 | 12 | 22 (32.8) |
| Total (1794) | 755 | 282 | 425 | 90 | 614 | 120 | 90 | 43 | 445 | 223 | 625 (34.8) |
Month-wise analysis of dengue cases in 2018 year.
Gender wise analysis of laboratory-confirmed dengue cases.
| Cases | N (%) | Mean age±SD (in years) |
|---|
| NS1 positive | 445 | |
| Adults | 324 (72.8) | 28.7±9.65 |
| Male | 217 (66.97) | 24.88±6.51 |
| Female | 107 (33.02) | 27.9±9.24 |
| Paediatrics | 121 (27.19) | 9.11±3.82 |
| Male | 69 (57.02) | 9.97±4.22 |
| Female | 52 (42.97) | 7.87±3.90 |
| IgM positive | 223 | |
| Adults | 159 (71.3) | 29.01±10.73 |
| Male | 110 (69.18) | 28.9±9.67 |
| Female | 49 (30.81) | 30.4±11.33 |
| Paediatrics | 64 (28.69) | 9.55±44.41 |
| Male | 37 (57.81) | 9.18±3.91 |
| Female | 27 (42.8) | 10.17±4.98 |
Discussion
Dengue is the most rapidly spreading mosquito-borne viral disease, affects tropical and subtropical regions of the world. In the last few decades, its incidence has increased more than 30-fold along with the extension to new countries and, in the current scenario, from urban to rural settings [2,8,23,24]. With the rising incidence, dengue infection causes significant morbidity and mortality especially in resource-poor developing countries and causes a huge burden on their economies [25]. Till date, there is no specific treatment or vaccine available for the prevention of the disease. However, early diagnosis of dengue infection would help in the timely implementation of appropriate treatment along with supportive care, thus greatly improving the consequence of the disease and also for effective public health control of dengue outbreaks [26,27]. Currently, several methods are available for the diagnosis of dengue infection such as detection of the virus, viral RNA, antigens or antibodies, or a combination of these methods. Virus isolation by tissue culture is considered the gold standard but it is time-consuming, expensive and laborious, requires high infrastructure, expertise and requires early 0-5 days post onset samples [28].
The Non-Structural protein 1 (NS1) antigen of dengue virus appears at the beginning of the fever and before the dengue IgM and/or IgG, emerge as a suitable option for dengue diagnosis [29]. World Health Organisation (WHO) has recommended the use of NS1 antigen for the timely detection of dengue infection [2,30].
In the present study, the diagnostic efficacy of two commercially available dengue NS1 and IgM ELISA tests were examined to know the incidence of laboratory-confirmed dengue cases among clinically suspected patients and the results revealed that the dengue fever outbreak in 2018 in Bundelkhand region. In our study, suspected dengue patients reported the complaint of fever for 1-7 days and more than 7 days were tested by NS1 and IgM ELISA for the diagnosis of dengue respectively. Of them, NS1 was able to diagnose more dengue cases than IgM ELISA test. Other studies have also found the efficiency of NS1 test for early diagnosis of dengue virus infection as it is detectable on the first day of fever of both primary and secondary dengue infections before the appearance of IgM antibodies [2,18-21]. However, the patients who had fever from 5 to 7 days these were tested for both NS1 and IgM ELISA. Interestingly, 19.5% IgM negative samples were picked up by NS1 ELISA which reinforce the utility of NS1 antigen detection while 14.5% NS1 negative samples were also detected as positive by IgM ELISA. Overall, 34.8% laboratory-confirmed dengue positive cases diagnosed by NS1 and/ or IgM dengue ELISA were found in our study. A similar rate (38.9%) of laboratory-confirmed dengue cases was also reported during the dengue fever outbreak in Delhi region [31]. However, Prakash O et al., in the year 2015 reported a lower rate of detection (22%) from Lucknow, Uttar Pradesh, India. The most plausible reason for this difference could be the variation in sample size and sampling sites. The study reported by him was based on more than double sample size than the present study [32]. Moreover, in this study samples were collected from the northern region, while the present study included samples from the central region of India. Although, several studies have been published on dengue outbreaks in India, maximum of these reports are comparatively based on small case series lacking useful evidence on important factors such as age, gender, urban/rural distribution of cases, seasonality of outbreaks and trends in the circulation of serotypes [5].
Initially, dengue was considered an urban disease as rapid development of urban areas in mid-twentieth century resulted in unauthorised or unplanned housing colony, improper water supply and wastewater management systems create the ideal conditions for the proliferation of the vector [5,32,33]. Therefore, the outbreak of dengue is continuously reported from the large cities of India: Delhi [5,31,34-36], Chandigarh [37], Pondicherry [38], Bangalore [39,40], Gwalior [41], Vellore and Chennai [38], Lucknow in Uttar Pradesh [32,42] and Calcutta in West Bengal [43,44]. The comparison of laboratory confirmed dengue cases reported from different regions of India have been shown in [Table/Fig-8] [45-47].
Comparison of laboratory confirmed dengue cases reported from different regions of India [45-47].
| Authors [Ref] | Study year | Laboratory confirmed cases | Region |
|---|
| Goswami L et al., 2018 [45] | 2013-2017 | 20% | North-East |
| Murhekar M, et al., 2019 [46] | 2014-2017 | 35.4% | North |
| 2014-2017 | 40.1% | North-East |
| 2014-2017 | 32.3% | East |
| 2014-2017 | 16.0% | West |
| 2014-2017 | 25.5% | South |
| Mørch K et al., 2017 [47] | 2011-2012 | 16% | North-East and South India |
| Present study | January to December 2018 | 34.8% | Central India |
As a tertiary care hospital, MLB medical college and hospital attends the patients from the different part of the Bundelkhand region and other nearby areas. In the present study, samples were received from the patients who hailed from different districts and found the occurrence of huge number of dengue cases in rural areas of many districts. Similar to our findings, several studies have also reported the dengue cases from rural areas in Uttar Pradesh [5,48], Madhya Pradesh [49], Maharashtra [50,51], Kerala [52] and West Bengal [53]. Thus in the current scenario, dengue is progressively spreading from urban to rural areas also. The most probable reason may be related to human ecological and socio-economic changes, such as increased transportation, mobility, development and rapidly spreading of peri-urbanisation, which lead to the invasion and proliferation of A. aegypti mosquitoes. Thus, dengue has now become a widespread health concern in India.
The role of environmental factors in the spreading of vector-borne diseases is well-known. The correlation between dengue occurrence and environmental factors such as rainy seasons, humid, post-monsoon season is clearly evident, which is related to favorable conditions for growth of vector mosquito Aedes aegypti and shorten the extrinsic incubation period [24]. In the present study, the maximum number of laboratory-confirmed dengue cases were recorded in the post-monsoon period (October and November), which is in agreement with previous studies [5,6,31].
In this study, the maximum number of laboratory-confirmed dengue cases belonged to age group more than 15 years with male preponderance, our findings correlated with the previous studies reported by Kumar A Ch et al., and Kumar A et al., Deshwal R et al., [24,40,54]. The male to female ratio was 1.6:1, which was in accordance with the previous studies [24,32,40]. However, Deshwal R et al., reported a slightly higher ratio of 2.67:1 [54]. Notably, male preponderance among the affected individuals has been reported in almost all the studies.
Limitation
The present study is based on the data collected between January 2018 and December 2018. The limitation of this study was that results were analysed retrospectively and the patient could not be followed for the final clinical outcome.
Conclusion
The report is based on the data analysed retrospectively which revealed the experience of dengue fever outbreak in the Bundelkhand region in 2018. Both NS1 and IgM ELISA tests were useful for the laboratory confirmation of dengue. NS1 in combination with IgM ELISA offers most sensitive diagnosis for dengue. Dengue fever in India occurs frequently during and shortly after the monsoon and the cases generally starts to increase onwards August. Hence, continuous monitoring of dengue virus is important for prevention and control during post-monsoon when the peak of dengue virus infection was observed.
*Niwari, Kanpur, Chitrakut, Bhind, Agra, Gwalior and Jaunpur combinedly