Osteoplastic Flap Approach for Posterior Table Leak: A Case Report
Rishikesh Thakur1, David Victor Kumar Irugu2, Hitesh Verma3
1 Senior Resident (ACAD), Department of Ear, Nose and Throat, AIIMS, Delhi, India.
2 Assistant Professor, Department of Ear, Nose and Throat, AIIMS, Delhi, India.
3 Assistant Professor, Department of Ear, Nose and Throat, AIIMS, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Hitesh Verma, Department of Ear, Nose and Throat, AIIMS, Delhi, India.
E-mail: drhitesh10@gmail.com
Frontal sinus Cerebrospinal Fluid (CSF) leak is relatively uncommon. Surgical treatment is indicated when conservative management fails. Here we present a case report of 19-year-old male who presented with delayed CSF rhinorrhea after trauma with one episode of meningitis. On evaluation, frontal sinus posterior vault leak was seen. The repair was done by osteoplastic flap raising approach. Follow-up clinico-radiological assessment showed no evidence of leak or defect. Although endoscopic approach is used most commonly now-a-days, defect in posterior vault may not be adequately dealt especially if defect is laterally or superiorly located as seen in this case. This case is reported to highlight the indication of open approach in endoscopic era.
Cerebrospinal fluid, Frontal sinus, Posterior vault
Case Report
A 19-year-old male was presented with history of watering from left nasal cavity since six months following road traffic accident. Clinically, forward bending aggravates the flow of watery fluid. He suffered from meningitis two months back and it was managed conservatively.
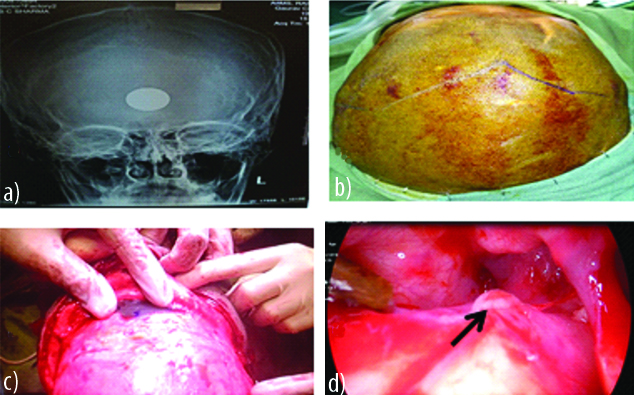
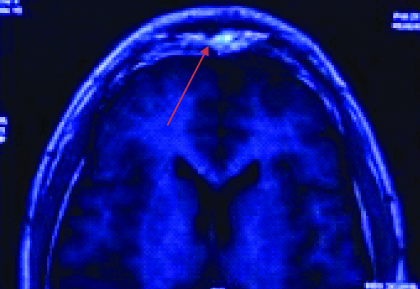
Diagnostic nasal endoscopy was done that revealed watery discharge in left frontal recess and subsequent biochemical analysis supported the diagnosis of CSF rhinorrhoea. Non-contrast Computed Tomography (NCCT) and Magnetic Resonance Cisternography (MRC) of brain pin point the 10 mm diameter defect in posterior table of frontal sinus left side [Table/Fig-1]. The defect was lying slightly higher in posterior table and osteoplastic flap repair was planned. NCCT raised the possibility of fracture line, might run through frontal sinus outflow tract area. Caldwell Luc radiographic view was taken from six feet distance to create the frontal sinus template. Bicoronal incision was made and X-ray template was used to mark outline of frontal sinus. The defect was found in posterior table of left side frontal sinus. Bilateral frontal sinus was demucosalized and meningocele was reduced with bipolar cautery. The defect was closed in multi-layers (both inlay and overlay) by abdominal fat, fascia, surgicel and pericranial flap [Table/Fig-2]. Frontal sinus was obliterated with abdominal fat. Post-operative period was uneventful and he was warranted for regular OPD visit.
(a) Non contrast computed tomography of Paranasal Sinus (PNS)-Sagittal section; (b) MR cisternography head (axial section) showing presence of hyperintensity at defect site of posterior table (red arrow).

a) Caldwell Luc radiographic view at 6 feet distance; b) The figure showing marked bicoronal incision; c) X-ray template was used intraoperatively to mark outline of frontal sinus; d) Intraoperative picture of posterior table defect with meningocele (black arrow).
The first follow-up MRI at three months interval showed healed defect with presence of hyper intense signal within the frontal sinus, which was suggestive of fat without secondary mucocele features [Table/Fig-3].
Post-op MRI T1 image revealing hyper intense signal within frontal sinus (suggestive of fat) with healed posterior table defect.
Discussion
Cerebrospinal Fluid (CSF) rhinorrhea is due to abnormal connection between subarachnoid space to sino-nasal area [1]. Ommaya AK et al., classified it into traumatic and non-traumatic groups [2]. Traumatic posterior table CSF rhinorrhea can be acute or delayed in presentation. The most common presentation is position dependent watery leak [3].
The diagnosis is based on clinical examination and biochemical evaluation. Imaging of NCCT-PNS and MRC provide an added advantage to locate the site of leak [4]. Isolated posterior table leak is uncommon and need surgical management if conservative treatment fails. Surgery can be broadly classified into open (external) and endoscopic approaches. Endoscopic frontal sinus leak repair is still a challenge for surgeon because of variation in anatomy, limited surgical instrument designed and high chance of failure in comparison to others [5]. However, alternate option is open approach in which osteoplastic flap approach is most commonly performed. It was described by Tato JM et al., and provides optimal view of frontal sinus in comparison to any other method, with no cosmetic deformity [6]. The commonly accepted indications are larger size defect, high defect, lateral defect, posterior bony vault defect with more than one table width of displacement, need of cranialisation, severe outflow injury with failed conservative treatment, multiple anterior table fractures [7,8]. Osteoplastic flap is not a popular technique in recent era [9-11]. Literature is more in favour of endoscopic Lothrop for posterior table defect but this technique is time consuming, requires specialised instruments and expertise whereas osteoplastic flap without craniotomy requires minimal instruments, less expertise and it can be done in much shorter time.
In our case, both open and endoscopic approaches were feasible but we opted for osteoplastic flap approach because of relative higher defect and for academic interest. This approach has many advantages-optimum exposure, close handling, good de-mucolisation and applicable for any size posterior table defect. It also provides highly vascularized pericranial flap with minimal surgical morbidity and good acceptable cosmoses [12].
Conclusion
Open surgical management for frontal sinus posterior bony vault CSF leak by osteoplastic flap is still a favourable option in high defect; in centers with basic instrumentation, limited expertise although we have chosen this for high site defect. It has added advantage of optimum exposure leading to high success rate, less complications and good cosmoses.
[1]. Ng M, Maceri DR, Levy MM, Crockett DM, Extracranial repair of pediatric traumatic cerebrospinal fluid rhinorrheaArch Otolaryngol Neck Surg 1998 124(10):1125-30.10.1001/archotol.124.10.11259776191 [Google Scholar] [CrossRef] [PubMed]
[2]. Ommaya AK, Di Chiro G, Baldwin M, Pennybacker JB, Non-traumatic cerebrospinal fluid rhinorrhoeaJ Neurol Neurosurg Psychiatry 1968 31(3):214-25.10.1136/jnnp.31.3.2145303103 [Google Scholar] [CrossRef] [PubMed]
[3]. Oh JW, Kim SH, Whang K, Traumatic cerebrospinal fluid leak: Diagnosis and managementKorean J Neurotrauma 2017 13(2):6310.13004/kjnt.2017.13.2.6329201836 [Google Scholar] [CrossRef] [PubMed]
[4]. Vemuri NV, Karanam LSP, Manchikanti V, Dandamudi S, Puvvada SK, Vemuri VK, Imaging review of cerebrospinal fluid leaksIndian J Radiol Imaging 2017 27(4):441-46.10.4103/ijri.IJRI_380_1629379240 [Google Scholar] [CrossRef] [PubMed]
[5]. Ramadan O, Frontal sinus CSF leak: Current managementJ Otolaryngol-ENT Res 2018 10(6):1-0.10.15406/joentr.2018.10.00385 [Google Scholar] [CrossRef]
[6]. Tato JM, Sibbald DW, Bergaglio OE, Surgical treatment of the frontal sinus by the external routeThe Laryngoscope 1954 64(6):504-21.10.1288/00005537-195406000-0000813175517 [Google Scholar] [CrossRef] [PubMed]
[7]. Ramadan O, Frontal sinus CSF leak: current managementJ Otolaryngol-ENT Res [Internet] 2018 10(6)[cited 2019 Mar 24]. Available from: https://medcraveonline.com/JOENTR/JOENTR-10-0038510.15406/joentr.2018.10.00385 [Google Scholar] [CrossRef]
[8]. Konstantinidis I, Constantinidis J, Indications for open procedures in the endoscopic eraCurr Opin Otolaryngol Head Neck Surg 2016 24(1):50-56.10.1097/MOO.000000000000021926679780 [Google Scholar] [CrossRef] [PubMed]
[9]. Correa AJ, Duncavage JA, Fortune DS, Reinisch L, Osteoplastic flap for obliteration of the frontal sinus: Five years’ experienceOtolaryngol Neck Surg 1999 121(6):731-35.10.1053/hn.1999.v121.a9821810580228 [Google Scholar] [CrossRef] [PubMed]
[10]. Ochsner MC, DelGaudio JM, The place of the osteoplastic flap in the endoscopic era: Indications and pitfallsThe Laryngoscope 2015 125(4):801-06.10.1002/lary.2501425417859 [Google Scholar] [CrossRef] [PubMed]
[11]. Shah A, Sengupta M, Saha PC, Saha S, Frontal sinus osteoplastic flap: is it relevant today?Egypt J Otolaryngol [Internet] 2018 34:229-233.[cited 2019 May 15]. Available from: http://ejo.eg.net/article.asp?issn=1012-5574;year=2018;volume=34;issue=4;spage=229;epage=233;aulast=Shah10.4103/1012-5574.244903 [Google Scholar] [CrossRef]
[12]. Salamone FN, Seiden AM, Modern techniques in osteoplastic flap surgery of the frontal sinusOper Tech Otolaryngol-Head Neck Surg 2004 15(1):61-66.10.1053/j.otot.2004.02.003 [Google Scholar] [CrossRef]