Low Back Pain (LBP) is a common phenomenon among working individuals and aging adults. Among the Indian population, 23% of the working adults, majority of whom are blue collar job holders, experience LBP. This condition is accompanied with psycho-social issues, absenteeism or shift to new jobs and dissatisfaction of present jobs [1]. Therefore, this condition places a substantial burden on the health care system. One of the numerous negative impacts of LBP is decreased postural control resulting in increased sway of static posture. This may occur due to weak core musculature. The main function of the core is to transmit forces generated from the lower extremities to the upper extremities, maintain alignment of posture and equilibrium dynamically during functional activities, thus negating distorted movement patterns [2].
Postural sway is a natural tendency of the Centre Of Pressure (COP) to shift during quiet standing. The sway occurs as a result of the interactions within neuromotor system and the process of stabilisation of an unstable body [3]. Postural stability has been defined as the ability to control the Center Of Mass (CoM) in relation to the base of support. The main sensory systems involved in postural control are proprioception, the vestibular system and vision, and their afferent pathways within the CNS. Afferent and efferent pathways involve the spinal cord, the brain stem, the cerebellum, the midbrain, and the sensorimotor cortex. All of these are implicated in the development of an internal representation of body posture that is continuously updated constructed on multisensory feedback and is used to forward commands to control body position in space. Increased postural sway is believed to be an attributor for higher risk of falls. It has also been proposed to identify individuals who are at a higher risk of falls from increased postural sway and then to refer these individuals for rehabilitation programs to reduce their respective risks [4]. An increased postural sway may lead to loss of static stability which may require excess muscular recruitment. Following such rehabilitation programs, postural sway could be reduced, the risk of falls and subsequent lower extremity injuries may be lowered as well as unnecessary energy expenditure could be averted.
The effect of four conditioning regimen by Downs DA. program following six weeks of core strengthening, balance, proprioceptive and isokinetic training on postural sway was compared and no difference was found in postural sway in any direction [5]. The examination of transient effect of core stability exercises on postural sway during quiet standing demonstrated that the trajectory of the COP decreases immediately following core stability exercises [6]. There is an evidence that strengthening of the spinal extensors that form part of the body’s core could affect postural stability [7]. Muscle performance depends on the training status of a muscle and varies between individuals as well as between muscles within an individual [8]. Training of groups of muscles that contribute to posture, as the hip and back extensors, may reasonably change not only muscle performance, but also postural stability and its respective central control mechanisms. Training of groups of muscles that contribute to posture, as the hip and back extensors, may reasonably change not only muscle performance, but also postural stability and its respective central control mechanisms. Regular isolated back extensor strength training is established as an effective method for the treatment of chronic musculo-skeletal disorders and is often prescribed for patients suffering from chronic LBP [9]. An increased postural sway may lead to loss of static stability which may require excess muscular recruitment. Following such rehabilitation programs, postural sway could be reduced, the risk of falls and subsequent lower extremity injuries may be lowered as well as unnecessary energy expenditure could be averted.
Thus, purpose of present study was to analyse the effect of core muscle strengthening on minimising postural sway and thereby preventing risk of falls, averting unnecessary energy expenditure and subsequent injury. The objective of present study was to determine if postural sway changes in association with core strengthening program and to investigate whether any changes occur in healthy individuals or in subjects with pain.
Materials and Methods
This case-control study comprising of 30 subjects was conducted in Outpatient and Inpatient Physiotherapy Department of Sri Ramachandra Hospital, Chennai, Tamil Nadu, India, from November 2012 till March 2013. The study was approved by Institutional Ethics Committee, IEC approval number (CSP/12/SEP/25/130) prior to commencement and a written informed consent was obtained from all the participants. The sample size was arrived based on the G power test. The cases were 15 patients of both gender aged 20 to 50 years with LBP of more than three months’ duration of non-traumatic origin. The controls were 15 closely age matched individuals who did not have any complaints of LBP and volunteered to participate in the study.
Inclusion criteria: Gender: both males and females, age: 20-50 years, LBP with or without radicular symptoms of more than three months’ duration of non-traumatic aetiology.
Exclusion criteria: Those subjects with a past history of trauma, spinal surgeries, neuromuscular, balance and vestibular disorders as well as psychologically unstable patients.
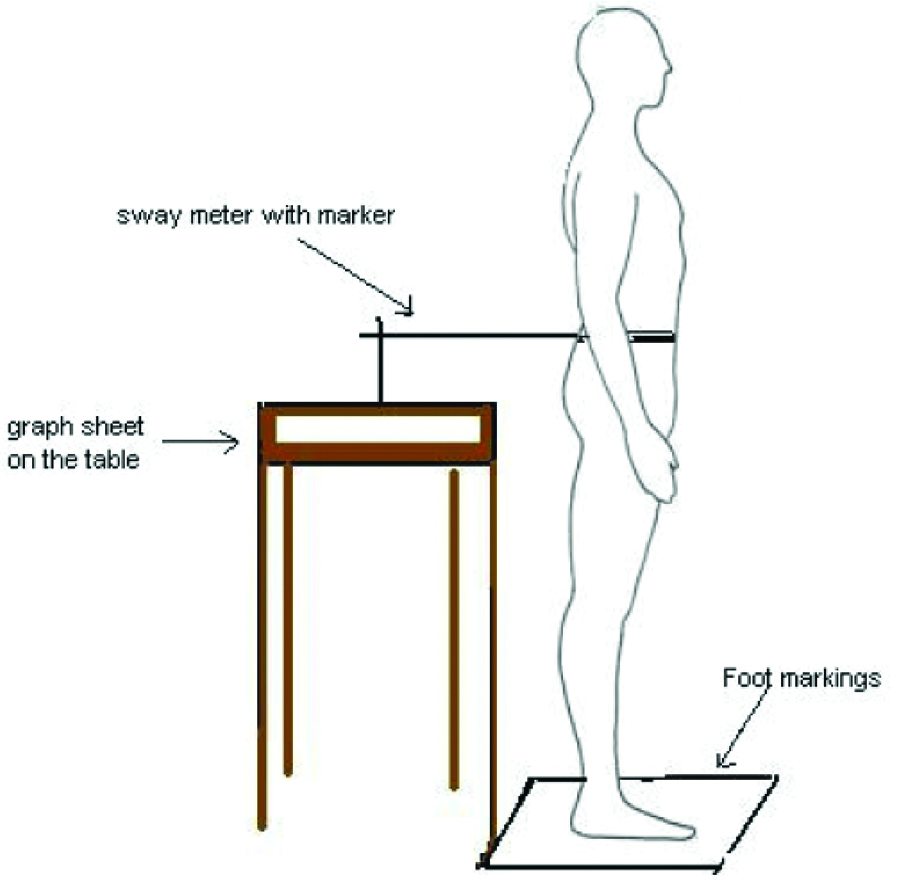
On the initial visit, an evaluation was performed to obtain the baseline measures of postural sway, lumbar lordosis and core strength. The postural sway for each subject was measured using a sway meter as depicted in [Table/Fig-1]. The method was adopted from a study entitled measurement of postural sway with a sway meter-An Analysis [10]. Sway meter considered over sophisticated force plate due to cost-effectiveness and was also an efficient method. Sway was assessed in the Antero-Posterior (AP) and Medio-Lateral (ML) directions [11]. The lumbar lordosis angle was measured using a Flexible ruler (Flexi curve). This method is used to determine the degree of thoracic kyphosis and lumbar lordosis. The equation used to convert the collected data to degree was 4 Arctang 2H/L equation. In the equation, L is the length of two obtained spinous process to the nearest millimeter. The length of a perpendicular line (H) drawn from the L to the curve called H as seen in [Table/Fig-2]. The procedure was as described in a study by Rajabi R et al., wherein a deep point or mid-point of arch would be an accurate method to measure the lumbar curvature angle using flexi ruler [12]. The Sahrmann assessment protocol was utilised for assessing the core musculature.
Measurement of postural sway using sway meter.
Measurement of lumbar lordosis angle.

Sahrmann’s testing progression/scoring criteria for lower abdominal strength/core activation [Table/Fig-3] [13].
Sahrmann’s criteria for lower abdominal strength [13].
| Manual muscle test grade | Criteria |
|---|
| 1/5 | The subject lifts one leg at a time to 90° of flexion with the knees positioned in flexion. From this position the subject lowers one leg at a time to the client position. Back remains flat. |
| 2/5 | The subject successfully performs Level 1, but upon lowering one leg to the table, s/he slides the leg into extension. The heel of the active leg may slide on or touch the surface of the treatment table during execution. The opposite leg must maintain a position of hip flexion of 90°, but no more, and its heel cannot touch the treatment table. Once the active leg has completed the slide into extension, the subject will rest the leg on a table, lift it back off the table, and return to the position of 90° of hip flexion before repeating with the other leg. |
| 3/5 | For Level 3, the subject performs Level 2, but instead of sliding the leg, s/he extends the leg while maintaining it off the treatment table through the entire range of motion. Once the subject completes extension, she rests the leg on the table, lifts the leg from the table, and returns it to the 90° hip flexed position before repeating the motion within the other leg. |
| 4/5 | The subject repeats level 1, but instead of lifting one leg at a time off the table, both legs are lifted simultaneously to the 90° hip flexed position, returned to the hook lying position, and fully extended. The return movement is completed by simultaneously sliding both legs back to the hook lying position followed by a bilateral leg lift into 90° of hip flexion. |
| 5/5 | For Level 5, the subject repeats the task for Level 4, but rather than sliding both legs along the surface of the treatment table, s/he extends both legs simultaneously, rests the legs of the completion of extension, lifts both legs from the table, and finally returns lands to the 90° hip flexed position. |
The exercises chosen for the purpose of strengthening the core musculature were:
Lower abdominal series-level one, where in subject is in crook lying position and instructed to pull the naval inward and upward without a breath-hold.
Semi sit ups-performed in crook lying, taking up the chin towards chest, such that upper back is lifted off the couch.
Sit-ups with rotation-performed in crook lying, arms crossed across the chest taking up the elbow towards the contralateral knee and alternating between both sides.
Lateral bridge- subject in side lying, is instructed to lift the trunk off the couch, while resting the head and foot on the couch.
All the exercises were performed by the participants under the supervision of physiotherapist in the Physiotherapy outpatient department. The exercises were performed in two sets of 10 repetitions each. Both the groups had undergone the exercise program. The outcomes were measured at baseline and one week later following the exercise program as per recommendations of Sahrmann’s core strengthening method.
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS 18.0 for Windows, SPSS, Inc., Chicago, IL) was utilised to conduct all statistical procedures. Wilcoxon signed rank test was used to compare the variables within the groups before and after exercise program. Mann-Whitney test was utilised to analyse variations following exercises between the cases and controls.
Results
Four females and eleven males were present in each of the case and control groups. The average age of the cases was 36.3 years and the controls averaged 34.7 years. Postural sway in any direction for the cases did not show a significant decrease following core strengthening, whereas the controls demonstrated significant decrease in ML sway (p=0.02). The comparison of postural sway between cases and controls is depicted in [Table/Fig-4].
Comparison of postural sway between cases and controls.
| Postural sway | Cases | | Control | | |
|---|
| Pre | Post | | Pre | Post | | |
|---|
| Mean±SD | p-value* | Mean±SD | p-value* | p-value** |
|---|
| Anterior | 1.23±0.99 | 1±0.62 | 0.4 | 0.75±0.46 | 0.580±0.39 | 0.44 | 0.03 |
| Posterior | 0.93±0.42 | 0.98±0.66 | 0.55 | 1±0.52 | 0.94±0.62 | 0.45 | 0.98 |
| Right lateral | 1.22±2.17 | 0.46±0.75 | 0.23 | 1.02±1.69 | 0.22±0.36 | 0.02* | 0.27 |
| Left lateral | 1.17±1.41 | 0.64±0.84 | 0.47 | 0.39±0.89 | 0.36±0.33 | 0.15 | 0.23 |
*p-value; within groups, paired t test. **p-value; between groups, unpaired t test
*p-value <0.05=significant
Following the exercise program of core muscles strengthening, there was a borderline significant difference (p=0.03) between the cases and controls in the AP direction showing that the controls had significantly less sway in this direction compared to the cases. There were no significant differences in the other directions between the groups [Table/Fig-4].
The pre and post-test lumbar lordosis angle for the cases was 33.32° (SD±18.11) and 38.32° (SD±13.81) respectively. The subjects belonging to control group had a lumbar lordosis with of 38.32° (SD±13.81) and 37.47° (SD±12.03) pre and post-test respectively. The comparison of lumbar lordosis angle between the cases and controls has been represented in [Table/Fig-5]. This revealed that, no significant changes in the lumbar lordosis angle had occurred between the groups following intervention.
Comparison of lumbar lordosis angle between cases and controls.
| Lumbar lordosis angle | Cases | Controls | p-value** |
|---|
| Mean±SD | Mean±SD | |
|---|
| Pre | 33.32±18.11 | 38.32±13.81 | |
| Post | 38.32±13.81 | 37.47±12.03 | 0.71** |
| p-value* | 0.33* | 0.75* | |
*p-value; within groups, paired t test; **p-value; between groups, unpaired t test; *p-value <0.05=significant
Among the cases, 12 subjects had Grade 0 on the Sahrmann core stability test and 3 subjects with Grade 1. The number of subjects with Grade 1 had significantly reduced (p=0.04) to 6 following the administration of exercise program. The controls did not demonstrate improvements in their core strength although they had better baseline readings of core strength where 9 subjects with Grade 0, 4 subjects with Grade 1 and 2 subjects with Grade 2. A comparative representation of Sahrmann’s test between the cases and controls has been depicted in [Table/Fig-6].
Comparison of Sahrmann’s test between cases and controls.
| Sahrmann’s test | Cases | Controls | |
|---|
| Pre | Post | p-value | Pre | Post | p-value |
|---|
| Grade | Freq | % | Freq | % | 0.04 | Freq | % | Freq | % | 0.39 |
| 0 | 12 | 80 | 9 | 60 | 9 | 60 | 9 | 60 |
| 1 | 3 | 20 | 6 | 40 | 4 | 27 | 4 | 27 |
| 2 | - | - | - | - | 2 | 13 | 2 | 13 |
Discussion
LBP is accompanied with psychosocial issues, absenteeism or shift to new jobs and dissatisfaction of present jobs. It is associated with decreased postural control resulting in increased sway of static posture, which may occur due to weak core musculature. Incorporating core strengthening programs, postural sway could be reduced; the risk of falls and subsequent lower extremity injuries may be lowered as well as unnecessary energy expenditure could be averted. Hence, the objective of present study was to determine the impact of core strengthening on minimising postural sway.
The results of study show that there is no significant reduction in postural sway following core strengthening. Individuals without LBP had a decrease in ML sway. There were also no significant changes in lumbar lordosis. The core strength of the patients improved significantly following core strengthening exercises.
The findings of sway characteristics correlate with a past study by Kaji A et al., where 5% and 18% of the subjects showed nil sway in the ML directions respectively with the eyes closed and; there was also no absence of sway in posterior direction among both the groups [6].
According to outcome of the present study, among the cases, at baseline, five subjects had an anterior sway of 2 cm and above with a maximum limit of 3.7 cm and a mean of 1.23 cm. Following a program of core muscle strengthening, they showed a decrease in mean sway in anterior direction with a mean of 1 cm (p=0.4). A further observation revealed that one subject did not have any sway and only one subject had a sway of more than 2 cm in anterior direction. As far as posterior direction is concerned almost seven subjects had 1 cm and above with a maximum limit of 1.8 cm and a mean of 0.93 cm. Following the exercise program, the average sway recorded was 0.98 cm (p=0.55) with the same seven cases showing a sway of more than 1 cm; none demonstrated an absence of sway in AP direction. The postural sway in ML direction had a more varied distribution with few subjects had an absence of sway in right or left directions. Almost 6 subjects did not record any sway to the left lateral direction and the maximum extent of sway was 4.2 cm with a mean of 1.93 cm. Among those who had a sway to left lateral direction, the mean was 1.17. Further, 5 subjects did not have a sway with a mean of 0.97. As far as right lateral direction, 7 subjects did not have a sway with a mean of 0.88 and among those who did have a sway the mean was 0.46 (p=0.47). Whereas 9 subjects did not demonstrate postural sway in right lateral direction with maximum of 5.7 cm and a mean of 3.05 cm. Among those who had sway in right lateral direction the overall mean was 1.22 cm.
These findings of sway characteristics correlate with those of Ramachandran S et al., in which, 5% and 18% of the subjects showed nil sway in the right and left directions respectively in eyes closed condition [10]. Also, there was no absence of sway in posterior direction among groups.
According to outcome of the present study, among the control subjects at baseline, one subject did not show sway in the anterior direction. Four subjects had an AP sway of 1 cm or more, nine subjects had less than 1 cm with a maximum of 1.8 cm and a mean of 0.75 cm among the 14 subjects who had sway in the AP direction; Following core strengthening program, the mean anterior sway reduced to 0.58 cm among the controls (p=0.44). For the posterior direction, six subjects showed sway of 1 cm or more and nine subjects less than 1 cm with a maximum of 2.1 cm and a mean of 1 cm; The mean posterior sway was 0.95 cm (p=0.45) post measure. Nine subjects did not show sway to the left lateral direction and the maximum recorded sway was 3.5 cm and a mean of 0.98 cm among those who had sway to the left lateral direction and an overall mean of 0.39 cm and 0.36 cm (p=0.15) after the exercise protocol. In the right lateral direction, five subjects had absence of sway with a mean of 3.22 cm among the subjects who had sway in this direction and overall mean of 1.02 cm for the group with a maximum of 6.2 cm. The sway significantly reduced for the right lateral direction with a mean of 0.23 cm (p=0.02) after the exercises.
These results were comparable to the study by Cairns MC et al., on healthy subjects wherein it was done on healthy young adults [14]. Since the quoted study was done on normal subjects, the findings of the study may be compared to the control subjects of present study. They found no significant difference in pre and post-measurements of AP sway but significant decrease in ML sway was observed. In the present study as well, the changes in AP sway was not noteworthy but there was significant reduction in right lateral postural sway which in turn comprises ML sway. This can be due to the finding that AP sway is under the control of ankle strategy whereas ML sway is under hip control. Since core strengthening does not influence the ankle complex, the indifference in AP sway changes could be explained. The hip and its governing musculature are one of the components of core. Hence, strengthening the core could influence the hip musculature as well. This basis can be accounted for the reduction in ML sway in this study.
The present study’s results contradict with a study by Shirey, which did not find any significant change in postural sway following a core strengthening program. The core muscle activation was associated with improved stability of the vertebral column. Intentional core activation had the utmost effect on lower extremity kinematics among individuals with lower core recruitment scores. These results propose that, individuals with lower core scores may have more to gain from increasing core stability [13]. But significant reduction in right lateral direction was found among the control subjects in this study. This may be attributed to the supervised protocol which lead to adherence of the subjects to the exercise protocol. The continuous mode of training for one week can also account for the difference between these two studies. The continuous mode of exercises for a period of seven days could have lead to enhanced motor relearning and its appropriate results in the present study.
After administration of core strengthening, the control subjects showed significantly less anterior postural sway than the cases (p=0.05). This could be due to the fact that the cases had a higher mean anterior sway (1.23 and 1.01 before and after intervention respectively) than the controls (0.75 and 0.58 before and after intervention respectively).
There was no significant difference (p=0.33) in the lumbar lordosis angle before (mean=33.32°) and after (38.32°) core strengthening among the cases. Neither was there any significant change (p=0.75) among the controls in the lumbar lordosis angle before and after strengthening the core muscles. This can be as a resultant of insufficient duration of the strengthening program. The duration utilised for the present study may be inadequate to significantly alter the lumbar spinal curvature.
The cases had weak core musculature with 80% having Grade 0 and 20% with Grade 1. The control group registered better core muscle strength compared to the cases with 2 of them with grade 2 using the Sahrmann core stability testing. But they did not show improvements in the grading after administration of core strengthening exercises.
Thus the cases significantly improved in their core muscle strength (p=0.04) following the exercise program. A past study by Aggarwal A et al., had produced similar improvements in the core stability upon exposure to core training. The endurance performance improved significantly only for the core stability training group (p<0.01), which concluded that core stability training was effective in improvement of lower trunk endurance performance [15]. Thus the results of the quoted study finding may be accounted upon for the outcome in present study as well. Conversely, the control subjects did not show any substantial improvement in the core strength following the exercise program for one-week duration although the controls had a higher proportion on Grade 1 or more core muscle strength.
Although the patients with LBP did not achieve significant reduction in postural sway after stabilisation program, they attained better core stability by improved core muscles strength. The controls demonstrated significant reduction of postural sway in the right lateral direction, but did not improve their core strength subsequent to the strengthening exercises.
Limitation
The present study had a limited sample size, hence further studies may be considered by undertaking a larger sample of subjects with and without LBP and comparing other forms of core strengthening exercises with a long term follow-up. The study may also be combined with force platforms to have a more precise measurement and to detect subtle variations in postural sway during standing.
Conclusion
There does not appear to be a significant difference in postural sway between patients with LBP and control subjects; to begin with these, LBP patients had a weak core musculature. LBP patients’ postural sway did not alter following core strengthening but readily improved their core muscle strength. The control subjects had a significant reduction in ML sway after strengthening but core strength remains unaltered.
*p-value; within groups, paired t test. **p-value; between groups, unpaired t test
*p-value <0.05=significant
*p-value; within groups, paired t test; **p-value; between groups, unpaired t test; *p-value <0.05=significant