The Semi-automated Software (MyAnkleTM) for Preoperative Templating in Total Ankle Replacement Surgery
Norliyana Mazli1, Mohd Yazid Bajuri2, Azrulhizam Shapii3, Mohd Rohaizat Hassan4
1 Doctor, Department of Orthopaedics and Traumatology, Universiti Kebangsaan Malaysia Medical Centre, Cheras, W.P Kuala Lumpur, Malaysia.
2 Professor, Department of Orthopaedics and Traumatology, Universiti Kebangsaan Malaysia Medical Centre, Cheras, W.P Kuala Lumpur, Malaysia.
3 Doctor, Department of Information Science and Technology, Universiti Kebangsaan Malaysia, Bangi, Selangor, Malaysia.
4 Professor, Department of Public Health, Universiti Kebangsaan Malaysia Medical Centre, Cheras, W.P Kuala Lumpur, Malaysia.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Mohd Yazid Bajuri, Professor, Department of Orthopaedics and Traumatology, Universiti Kebangsaan Malaysia Medical Centre, Cheras, W.P Kuala Lumpur, Malaysia.
E-mail: ezeds007@yahoo.com.my
Introduction
MyAnkleTM software is semi-automated digital templating software for total ankle replacement surgery. This software enables a surgeon to review multiple sizes of implant over the radiograph for implant size determination. It has auto-scaling properties which matches the magnification of the radiograph and template. This software is evaluated by testing the accuracy and inter-observer reliability of pre-operative digital templating for total ankle replacement.
Aim
To evaluate the accuracy and inter-observer reliability of pre-operative digital templating of tibia and talar component size for total ankle replacement using MyAnkleTM digital templating software.
Materials and Methods
This was retrospective study in which digital radiographs of patients who had undergone primary total ankle arthroplasty were evaluated. The operations were done in between year 2014 until 2017 in Universiti Kebangsaan Malaysia Medical Centre (UKMMC). All cases were using non-constrained anatomic shaped 3-component system prosthesis (Hintegra). The digital templating software (MyAnkleTM) was used for templating, by two foot and ankle surgeons from different centres. The predicted implant size was compared with the actual components selected at the time of surgery and its accuracy was measured. The inter-observer reliability was analysed using the linear weighted kappa (κ) analysis.
Results
The size of tibial and talar component was accurate in 83.3% and 91.7% respectively. The accuracy of correct predicted size for second surgeon was 66.7% for talar component size and 58.3% for tibia component size. The inter-observer reliability for tibial and talar component size was substantial, weighted kappa (κ)=0.802 (95% CI, 0.623 to 0.982), p<0.001.
Conclusion
MyAnkleTM software is an effective tool for pre-operative planning in total ankle replacement surgery. It provides rapid, reproducible accurate results and cost-effectiveness.
Ankle joint, Arthroplasty, Osteoarthritis
Introduction
Computer-assisted surgery refers to a surgical method which utilises the computer for surgical planning and guiding during the procedure. The objective of this technology is to achieve better results by combination of accuracy and precision of the computer with the surgeon’s operating skills [1]. The application of computer-assisted surgery in total ankle arthroplasty is still new, compared to hip and knee surgery. Digital templating software is one of the computer-assisted methods for pre-operative planning. The application of scientific visualisation and digital images with integrated computer system in medical field helps to facilitate in diagnosis, surgeries and therapy. This technology can help clinicians and surgeons to improve the quality of care for their patients but experience is still of utmost importance.
MyAnkleTM software is a newly developed, semi-automated computer-aided digital templating software for Total Ankle Replacement (TAR). This software allows a surgeon to review multiple sizes of implant over the radiograph for implant size determination. Hintegra total ankle template was used to create the template image library. It has distinctive special features for manipulation of implant from front or side as well as allowing rotation and flipping of the implant image in two axes. These features permit a better manipulation of implant image to match with the size of patient’s bone in radiograph.
In conventional templating, a surgeon has to deal with the radiographic magnification and acetate template magnification. The template provided by the implant manufacturer is an outline of the implant in various sizes printed on acetate. The surgeon will then overlay this acetate template onto the ankle radiograph to match the size with the anatomy of the patient. To address this problem, the radiograph is taken with a scale marker at the side of joint. The acetate template has a scale marker determined by the manufacturer. The surgeon has to adjust and match the two magnifications manually to determine the size of implant. It involves multiple steps which are time consuming and liable to magnification error. MyAnkleTM has been developed with an auto-scaling program that matches the digital X-ray images and the implant templates to same magnification. This auto-scaling program is able to minimise the time consumption during digital templating and eliminates radiographic magnification error. These advantages facilitate a surgeon in pre-operative planning and provide a better outcome of the surgery.
Pre-operative planning in joint replacement surgery is crucial to assess the need for non-standard implant sizes, plan the levels of bony resection and anticipate the appropriate instruments needed intraoperatively [2]. In total ankle replacement, the aim of the surgery is to restore the anatomy and biomechanics of the diseased ankles as much as possible. To achieve this goal, proper sizing and correct positioning of the implant are important in order to allow the ankle to move about a centre of rotation. A proper sizing is also important to prevent complications e.g., impingement, soft tissue problems and late migration of component [3].
Prior to the development of digital templating software, pre-operative planning was performed using acetate templating and radiograph. This method can contribute to surgical error due to variation in the radiographic magnification factor because acetate templates assume approximately 110-120% magnification [4]. The elimination of printed radiographic film with the advent of digital radiography and Picture Archiving and Communication Systems (PACS) favours the evolution of digital templating software for joint replacement surgery. This technology also offers a rapid and reproducible pre-operative planning in which a permanent record of the template can be saved and is cost-efficient [2-5].
TAR has developed tremendously for the past four decades. After the first total ankle arthroplasty in 1970 by Lord and Marotte, more than 20 different types of ankle arthroplasty were developed [3]. The encouraging short-term, mid-term and long-term results have increased the demand of TAR for treatment of end-stage osteoarthritis [6-9]. Therefore with the advancement of technology and digital imaging, it will be beneficial to have a software for digital templating of TAR for pre-operative planning. This technology can facilitate a surgeon to have a more accurate implant selection and pre-operative planning. A good pre-operative planning and surgical technique will certainly provide a promising outcome [10].
A number of digital templating software for total hip and total knee arthroplasty has been developed and studied for their accuracy and comparison with the acetate template [2,5,11,12]. Levine B et al., studied the accuracy of digital templating software in a series of 269 patients. They concluded that digital templating is an effective means for predicting the size of hip and knee implant [2]. Another studies by Specht LM et al., and The B et al., suggested that digital templating is accurate for predicting a knee implant sizing [5,11].
To the best authors’ knowledge, there was no other study regarding accuracy of digital templating software for total ankle arthroplasty. The aim of this study was to evaluate the accuracy and inter-observer reliability of pre-operative digital templating of tibia and talar component size for TAR using the newly developed MyAnkleTM digital templating software.
Materials and Methods
A retrospective study was conducted on 12 patients who underwent primary total ankle arthroplasty in a period of three years (2014-2017) in Universiti Kebangsaan Malaysia Medical Centre (UKMMC). Selection criteria were patients with ankle osteoarthritis who underwent primary total ankle replacement. Patients with charcot arthropathy, severe ankle trauma complicated with avascular necrosis of talus and revision surgery were excluded from the study. The ankle radiograph was taken in anteroposterior and lateral projection in weight bearing position. The diagnosis for patients in this series is ankle osteoarthritis; primary and post-traumatic. All patients were operated by an experienced foot and ankle surgeon using non-constrained anatomic shaped 3-component system prosthesis (Hintegra). Institutional Ethical Approval was obtained for this study (UKM 1.5.3.5/244/FF-2014-374).
The digital templating software (MyAnkleTM) was used for templating, by two foot and ankle surgeons from different centres. This software only includes templates from Hintegra total ankle implant. The tibia and talar components size ranges from size 0 to size 6. The digital template is created by using Computer-Aided Design (CAD) model. The image format in CAD format must be converted to .gif file format before it is applied to the system. The software development is based on Software Development Life Cycle (SDLC). This method is one of the simplest methods to develop software. SDLC allows for identification and rectification of problems during the development of the software.
The templating process involved selecting the size of prosthesis and positioning of the implant to distal tibia and talus. The tibia and talar component sizes were changed accordingly until an appropriate size is achieved. The size of the implant image can be changed by typing the appropriate size number in the ‘ankle size’ column. The example of a case that has been templated using MyAnkleTM software is shown in [Table/Fig-1]. In patient with ankle deformity, the implant can be rotated to accommodate the deformity [Table/Fig-2]. The final sizes during templating were taken as predicted size of implant.
Example of templating for tibial component using MyAnkleTM software.

Example of templating for talar component using MyAnkleTM software. The implant can be rotated to accomodate the ankle deformity.

Statistical Analysis
The predicted sizes were compared with actual sizes used in the operation and analysed for accuracy and inter-observer reliability. The accuracy means degree of agreement between the predicted size by digital templating and the actual size used intraoperatively. The accuracy was measured for two situations; the predicted size was similar to the actual size used or within one size variation. The inter-observer reliability is assessed using the linear weighted kappa (κ) coefficient of Cohen. Kappa values were interpreted according to guidelines by Landis and Koch [Table/Fig-3] [13]. All statistical analyses were performed by SPSS version 22.0 software.
Interpretation of kappa values.
| Kappa | Strength of agreement |
|---|
| ≤0 | Less than chance agreement |
| 0.0 to 0.20 | Slight agreement |
| 0.21 to 0.40 | Fair agreement |
| 0.41 to 0.60 | Moderate agreement |
| 0.61 to 0.80 | Substantial agreement |
| 0.81 to 0.99 | Almost perfect agreement |
Results
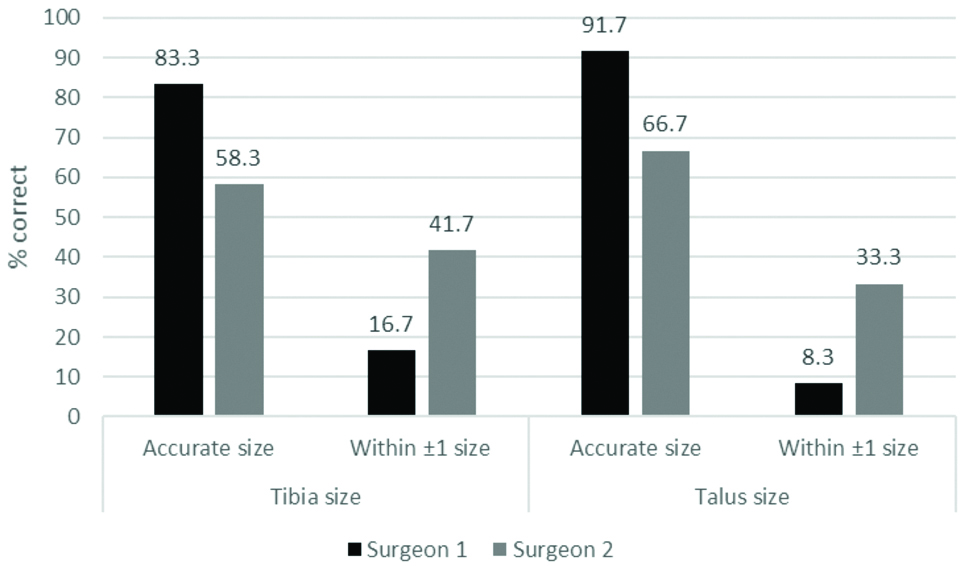
The digital templating was accurate in predicting similar implant size in 91.7% for talar component and 83.3% tibia component [Table/Fig-4]. The accuracy of correct predicted size for second surgeon was 66.7% for talar component and 58.3% for tibia component size. The predicted size of implant was within one size variation in 16.7% for tibial component and 8.3% for talar component by the first surgeon. The second surgeon predicted the size of implant was within one size variation in 41.7% and 33.3% for tibial and talar respectively.
The accuracy in digital templating of tibia and talar component using MyAnkleTM software.
The [Table/Fig-5] shows cross tabulation comparing the templated tibial component size between the two observers. Both surgeons agreed on the tibia component size for nine patients. The overall agreement for tibial component size was substantial, weighted κ=0.802 (95% CI, 0.623 to 0.982), p<0.001. Both surgeons agreed on the talar component size for nine patients [Table/Fig-6]. The overall agreement for tibial component size was substantial, weighted κ=0.80 (95% CI, 0.623 to 0.982), p<0.001.
Cross tabulation of tibial component size between two surgeons.
| Digital Templating-Tibia |
|---|
| Surgeon 2 | Total N (%) |
|---|
| 0 | 1 | 2 | 3 | 4 |
|---|
| Surgeon 1 | 0 | 1 | 1 | 0 | 0 | 0 | 2 (16.7) |
| 1 | 0 | 3 | 0 | 0 | 0 | 3 (25) |
| 2 | 0 | 0 | 2 | 1 | 0 | 3 (25) |
| 3 | 0 | 0 | 0 | 3 | 1 | 4 (33.3) |
| 4 | 0 | 0 | 0 | 0 | 0 | 0 (0) |
| Total N (%) | 1 (8.3) | 4 (33.3) | 2 (16.7) | 4 (33.3) | 1 (8.3) | 12 |
Cross tabulation of talar component size between two surgeons.
| Digital Templating-Talus |
|---|
| Surgeon 2 | Total N (%) |
|---|
| 0 | 1 | 2 | 3 | 4 |
|---|
| Surgeon 1 | 0 | 1 | 1 | 0 | 0 | 0 | 2 (16.7) |
| 1 | 0 | 3 | 0 | 0 | 0 | 3 (25) |
| 2 | 0 | 0 | 2 | 1 | 0 | 3 (25) |
| 3 | 0 | 0 | 0 | 3 | 1 | 4 (33.3) |
| 4 | 0 | 0 | 0 | 0 | 0 | 0 (0) |
| Total N (%) | 1 (8.3) | 4 (33.3) | 2 (16.7) | 4 (33.3) | 1 (8.3) | 12 |
Discussion
Pre-operative planning in joint replacement surgery is crucial for the surgeon to plan the levels of bony resection, anticipate size of implant and the appropriate instruments needed intraoperatively [2]. MyAnkleTM digital templating software provides surgeon with fast, accurate and reproducible results. The availability of digital radiograph and Picture Archiving and Communication Systems (PACS) favours the application of MyAnkleTM software for digital templating. The process of templating will be faster because MyAnkleTM software has an auto-scaling properties and integrated digital implant library. These features eliminate the need to prepare acetate template and manual adjustment to match the radiographic magnification and acetate template magnification. Thus, the risk of surgical error that arises from radiographic magnification error is eliminated. The use of this software is cost-efficient, as there is no need for printing of radiograph and storage.
MyAnkleTM software is user friendly and has distinctive special features for manipulation of implant. It allows rotation and flipping of the implant image in two axes. These features permit a better manipulation of implant image to match with the size of patient’s bone in radiograph. The size of the implant image can be changed by typing the appropriate size number in the ‘ankle size’ column. Hintegra TAR template was used to create the template image library. The results of digital templating can be saved for future references.
Studies have shown varying results in accuracy and inter-observer reliability of digital templating software of hip and knee replacement surgery [5-12,14-16]. In comparison with conventional acetate templating, Specht LM et al., reported that digital technique was more accurate in predicting tibial component size in total knee arthroplasty [5]. However, these two techniques did not differ much in predicting size of femoral component [5]. A retrospective study of 173 hips and 65 total knees showed that digital templating for knee arthroplasty was more accurate than manual templating [11]. The inter-observer reliability was good for templating of knee implant sizes (κ-values 0.63-0.75), but was fair for the hip arthroplasties (κ-values 0.22-0.54) [11].
The B et al., conducted a randomised control trial of 210 total hip arthroplasties to compare the technical and clinical results of digital templating for primary hip replacement with manual templating [12]. The study concluded that digital pre-operative planning slightly surpasses the analogue plans [12]. In the analyses of Pullen WM and Whiddon DR et al., on comparing these two techniques of templating, the acetabular component sizes were accurate in 93% of patients using digital templating and in 96% using acetate templating [14]. Another study by Miller AG and Purtill JJ, on accuracy of digital templating in total knee replacement mentioned that the digital templating benefit the surgeons in two aspects: reliability in prediction of implant size by the surgeon and determination of reliable starting point for implant size and position [15].
This study evaluates the accuracy and inter-observer reliability of digital templating using MyAnkleTM digital templating software. The accuracy of the predicted size is preferably the exact size or within one size variation. The increment within implant sizes is 2 mm; hence results in differences of 4 mm to 6 mm if predicted implant is within two or three size variation. Larger size implants will cause overstuffing and complication such as fracture and limited range of motion.
In this series of 12 total ankle arthroplasties, digital templating was accurate in predicting similar implant size in 83.3% and 91.7% for tibia and talar component respectively. Second observer accurately predicts the exact size in 7 cases (58.3%) for tibia component and 8 cases (66.7%) for talar component. Both surgeons predicted the exact size of implant and within one size variation compared to actual size used intraoperatively for all cases in this series. The differences in accuracy between the two surgeons are possibly attributed to the years of experience in doing total ankle arthroplasty. With regards to inter-observer reliability, both surgeons had agreed on tibia and talar implant size for nine patients. They had good agreement (κ=0.802) for both tibia and talar implant size.
These results were comparable with a study by Trickett RW et al., which demonstrated a good inter-observer agreement for both femoral and tibial component size in total knee replacement [16]. The correct size implant was predicted in 55% of tibial and 48% of femoral components by digital templating [16]. Levine B et al., reported that the correct implant size was predicted accurately in 58% of total hip arthroplasties and 66% of total knee replacement [2].
Digital templating software is a reliable tool for pre-operative planning of joint replacement surgery and act as an adjunct to facilitate a surgeon in reducing the burden of carrying printed radiograph and acetate template.
Limitation
The digital templating software is semi-automated and the predicted size may depend on the skill and experience of the surgeon in dealing with ankle osteoarthritis especially cases with ankle deformity.
Conclusion
MyAnkleTM digital templating software is a reliable tool for surgical planning in TAR surgery. This software will become the first step of technology advancement in foot and ankle surgery. The development of this software will provide a launching pad for more innovation in computer-assisted surgery such as infrared navigation camera, wireless instrument and other intuitive software.
To the best of authors’ knowledge, this was the first study to develop digital templating software for total ankle arthroplasty and evaluate the accuracy and reliability of digital templating. Further evaluation of the software with more number of total ankle arthroplasty cases is recommended.
[1]. Stiehl JB, Heck DA, Computer-assisted surgery: basic conceptsInstr Course Lect 2008 57:689-97. [Google Scholar]
[2]. Levine B, Fabi D, Deirmengian C, Digital templating in primary total hip and knee arthroplastyOrthopedics 2010 33(7):79710.3928/01477447-20100924-04 [Google Scholar] [CrossRef]
[3]. Valderrabano V, Pagenstert G, Hintermann B, TAR- Three-Component ProsthesisTechniques in Foot Ankle Surg 2005 4(1):42-45.10.1097/01.btf.0000152575.86782.8a [Google Scholar] [CrossRef]
[4]. Bono J, Digital templating in total hip replacement: a new gold standard?In Orthopaedic Proceedings 2004 86(SUPP IV):41310.2106/00004623-200412002-0001615691116 [Google Scholar] [CrossRef] [PubMed]
[5]. Specht LM, Levitz S, Iorio R, Healy WL, Tilzey JF, A comparison of acetate and digital templating for total knee arthroplastyClin Orthop Relat Res 2007 464:179-83. [Google Scholar]
[6]. Hintermann B, Knupp M, Zwicky L, Barg A, TAR for treatment of end-stage osteoarthritis in elderly patientsJ Aging Res 2012 http://dx.doi.org/10.1155/2012/34523710.1155/2012/34523722720158 [Google Scholar] [CrossRef] [PubMed]
[7]. Hintermann B, Valderrabano V, Dereymaeker G, Dick W, The HINTEGRA ankle: rationale and short-term results of 122 consecutive anklesClin Orthop Relat Res 2004 424:57-58.10.1097/01.blo.0000132462.72843.e815241144 [Google Scholar] [CrossRef] [PubMed]
[8]. Valderrabano V, Hintermann B, Dick W, Scandinavian TAR- A 3.7-year Average Follow-up of 65 PatientsClin Orthop Relat Res 2004 (424):47-56.10.1097/01.blo.0000132245.18548.09 [Google Scholar] [CrossRef]
[9]. Barj A, Zwicky L, Knupp M, Henninger HB, Hintermann B, HINTEGRA total ankle replacement: survivorship analysis in 684 patientsJ Bone Joint Surg Am 2013 95(13):1175-83.10.2106/JBJS.L.0123423824385 [Google Scholar] [CrossRef] [PubMed]
[10]. Bajuri MY, Tan BC, Das S, Hassan S, Subanesh S, Compression Neuropathy of the Common Peroneal Nerve Secondary to A Ganglion CystClin Ter 2011 162(6):549-52. [Google Scholar]
[11]. The B, Diercks RL, Van Ooijen PM, Van Horn JR, Comparison of analog and digital pre-operative planning in total hip and knee arthroplasties. a prospective study of 173 hips and 65 total kneesActa Orthop 2005 76(1):78-84.10.1080/0001647051003036415788312 [Google Scholar] [CrossRef] [PubMed]
[12]. The B, Verdonschot N, Van Horn JR, Van Ooijen PM, Diercks RL, Digital versus analogue pre-operative planning of total hip arthroplasties: a randomized clinical trial of 210 total hip arthroplastiesJ Arthroplasty 2007 22(6):866-70.10.1016/j.arth.2006.07.01317826278 [Google Scholar] [CrossRef] [PubMed]
[13]. Landis JR, Koch GG, The measurement of observer agreement for categorical dataBiometrics 1977 33(1):159-74.10.2307/2529310843571 [Google Scholar] [CrossRef] [PubMed]
[14]. Pullen WM, Whiddon DR, Accuracy and reliability of digital templating in primary total hip arthroplastyJ Surg Orthop Adv 2012 22(2):148-51.10.3113/JSOA.2013.014823628568 [Google Scholar] [CrossRef] [PubMed]
[15]. Miller AG, Purtill JJ, Accuracy of digital templating in total knee arthroplastyAm J Orthop (Belle Mead NJ) 2012 41(11):510-12. [Google Scholar]
[16]. Trickett RW, Hodgson P, Forster MC, Robertson A, The reliability and accuracy of digital templating in total knee replacementJ Bone Joint Surg Br 2009 91(7):903-06.10.1302/0301-620X.91B7.2147619567854 [Google Scholar] [CrossRef] [PubMed]