A Cross-sectional Study on Grip Ability Test and its Relation with “Hy” Band: Surrogate Marker for Amyloidosis in Patients with Rheumatoid Arthritis
KR Senthil Kumari1, GJ Swetha Varsha2
1 Professor, Department of Physiology, Government Thiruvanamalai Medical College, Thiruvanamalai, Tamil Nadu, India.
2 Final Year MBBS Student, Department of Physiology, Government Villupuram Medical College, Villupuram, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: GJ Swetha Varsha, 1/272, 1st Cross Street, Selvakumar Avenue, Thurai Pakkam, Chennai-97, Tamil Nadu, India.
E-mail: j.swethavarsha@yahoo.in
Introduction
Rheumatoid Arthritis (RA) is a chronic inflammatory disease of autoimmune origin. The disease has specific predilection for small joints of the body especially joints of the hand. Thus, by evaluating the hand grip ability, we can measure the severity of RA. The “Hy” band occurs due to an increase in prealbumin as shown by Serum protein electrophoresis. Few studies on Prealbumin show that increased prealbumin is directly associated with Amyloidosis. Amyloidosis being a known complication of RA drew attention towards “Hy” band.
Aim
To establish Grip Ability Test (GAT) as a predictor of RA severity and find its correlation with presence of “Hy” band.
Materials and Methods
This cross-sectional study was conducted at Government Villupuram Medical College, Tamilnadu, India. The study included 20 RA patients diagnosed by ARA/EULAR 2010 criteria, recruited from the Department of Orthopaedics. After due ethical clearance, all demographic data, DAS28 score, ESR, Duruoz Hand Index were obtained. GAT was performed using Handgrip Dynamometer. “Hy” band was detected by Serum electrophoresis using automated capillary zone electrophoresis. The values were pooled and statistical analysis was performed using epi info version 7.2.2 p-value <0.05 was considered significant.
Results
There was a statistically significant correlation between GAT and disease activity (p=0.001). Statistical significance for correlation between “Hy” band and GAT values was dull (p=0.7279 in dominant hand and 0.3337 in non-dominant hand).
Conclusion
GAT shows significant correlation with disease activity. Hence, GAT will serve as a reliable and objective method of measuring disease severity in RA. GAT may be used as a clinically simple performance based prognostic tool. The presence of “Hy” band shows no correlation with GAT scores.
Disease activity score, Hand strength, Prognosis, Rheumatology, Serum electrophoresis, Transthyretin
Introduction
RA is notable for de-novo origin and haphazard progression. Any clue in understanding the disease further will help us tackle the challenges in therapy. RA has high affinity towards small peripheral joints. Hand involvement is characteristic of RA, leading to difficulties in Activities of Daily Living (ADL). GAT is a quick, easy and objective test for measurement of hand function [1]. Thus, ‘Grip ability test’ is a reliable measure of hand involvement in RA [2,3]. In addition, the grip strength is indicative of overall well being of the patient and denotes the muscle strength, built and endurance [4,5].
Chronic inflammatory diseases are known to produce perturbation of protein metabolism [6,7]. Hence, authors studied the protein electrophoretic pattern in patients with RA. The presence of “Hy” band which migrates with velocity greater than albumin was noted in the previous study [8]. This “Hy” band is a surrogate marker for the risk of Amyloidosis. “Hy” band lies in the prealbumin region indicating an obvious rise in prealbumin [9]. Elevated levels of prealbumin are directly linked with Amyloidosis as shown by previous studies [10,11]. The underlying mechanism is that the prealbumin protein-transthyretin in the wild form or when mutated gets deposited in tissues as amyloid deposits [12,13]. A possible intervention to prevent Amyloidosis is to scavenge the free prealbumin protein by administration of retinol. This is based on the principle that Transthyretin is involved in stabilisation of Retinol-RBP (Retinol Binding Protein) complex [14]. Authors confirmed the presence of this “Hy” band in 70% of RA patients in the previous study [8]. As a way ahead, our hypothesis was to find any relation between presence of “Hy” band and GAT.
Materials and Methods
This cross-sectional study was conducted at Government Villupuram Medical College and Hospital. The sample size used was 21 based on a similar study [9]. Moreover, the presence of “Hy” band in serum of Rheumatoid arthritis was not a highlighted feature in the our parent article. The presence of “Hy” band was confirmed only in the synovial fluid in their study. So in order to confirm the presence of the band in serum, authors did a pilot study [8]. As a step further, authors did GAT for the same patients and tried to find its relation with “Hy” band. Hence, the study included 20 patients with active RA who were diagnosed according to the American College of Rheumatology/European League Against Rheumatism (EULAR) 2010 criteria [15]. The EULAR score was calculated at the first visit and monitored during subsequent follow-ups and those having a score below 6 are considered to be in the inactive stage of disease. The EULAR criteria is a comprehensive criteria which takes into account the number of joints involved, presence of RA factor, presence of Anti-CCP and duration of symptoms. It was developed for the purpose of selecting homogeneous populations for studies [16]. Patients having diabetes mellitus, metabolic diseases, diseases affecting neuromuscular function, renal diseases, hepatic diseases and other autoimmune diseases were excluded from the study.
Institutional ethical clearance for the study was obtained and the study was conducted for a period of two months from June 2018 to August 2018.
All relevant data such as duration of disease, presence of morning stiffness and treatment history were collected. The numbers of tender and swollen joints were counted and the patients were examined for the presence of hand deformities. Duruoz Hand Index (DHI) is a questionnaire evaluating quality of hand function in ADL such as eating, dressing, personal hygiene, etc., [17]. It is suggestive of the overall well being of the patient [4,5] and hence used as a measure of General Health in calculating DAS28. The questionnaire was filled by interview method.
Disease activity was measured by Disease Activity Score 28 [18]:
DAS28=0.56*√TJC28+0.28*√SJC28+0.70*ln(ESR)*1.07 +0.014*GHTJC 28=Tender joint count 28; SJC 28=Swollen joint count 28. The 28 joints are: Shoulder joint (2), Elbow joint (2), Knee joint (2), Wrist joint (2) and Hand’s PIP and MCP joints (20). ESR was measured by Westergren method in the Physiology laboratory. DAS28 is a well known and reliable measure of the severity of Rheumatoid arthritis [18]. The patients were split into three categories based on DAS28 scores as mild (DAS<5), moderate (DAS 5 to7) and severe (DAS>7). After taking consent and following all aseptic precautions, 3 cc blood was collected from each patient and the blood was stored at 4°C for three hours. The serum protein electrophoresis was carried out by automated capillary zone electrophoresis.
GAT was performed using Handgrip Dynamometer. The tests were conducted after 10 am in order to eliminate the influence of morning stiffness. Hand dominance was enquired. Before starting the test, the patient was asked to hold the apparatus and if the patient was unable to hold the apparatus, the GAT scores are taken as zero. If the patient was capable of holding the apparatus, the test was carried out with patient in sitting position, elbow flexed and forearm supinated and the patient was asked to clench the handle of the apparatus. The values are noted in kilograms. Three trials were conducted for each hand and the mean value was noted.
Statistical Analysis
All the readings were tabulated and statistical analysis for correlation between GAT score and disease activity was performed by ANOVA. Student t-test was used for finding correlation between GAT scores and the presence of “Hy” band using epi info software version 7.2.2.
Results
The study included 20 subjects with a male female ratio of 3:17. There was one patient with Juvenile Rheumatoid arthritis (JRA). On classifying patients based on DAS28 scores, three patients were in mild group, nine patients in moderate group and eight patients in severe group. The mean grip strength observed in dominant hand was 6.94±8.59 and in the non-dominant hand was 6.11±9.03 [Table/Fig-1]. On analysing the data using ANOVA test, there was a statistically significant correlation between disease activity and GAT with a p-value of 0.001 in both dominant and non-dominant hand [Table/Fig-2a,b,3 and 4]. As stated earlier, “Hy” band was positive in 70% of cases (n=14) [Table/Fig-5,6]. The presence of “Hy” band showed no correlation with GAT scores with p-value of 0.7279 in Dominant hand and p-value of 0.3337 in non-dominant hand [Table/Fig-7,8]. Deformities were present in eight cases-Boutainnaire (n=8), Swan neck (n=1), Ulnar deviation (n=5), Rheumatic nodules (n=1). The presence of deformities showed no correlation with GAT scores in both dominant and non-dominant hand [Table/Fig-9,10].
| N | Minimum | Maximum | Mean | Std. deviation |
|---|
| Age | 20 | 13.0 | 60.0 | 40.900 | 11.1019 |
| DHI | 20 | 16.0 | 86.0 | 49.550 | 19.8295 |
| DAS28 | 20 | 4 | 8 | 6.51 | 1.207 |
| ESR | 20 | 9.0 | 68.0 | 22.750 | 13.2779 |
| DOM_GAT | 20 | 0.0 | 28.3 | 6.945 | 8.5918 |
| NDOM_GAT | 20 | 0.00 | 30.70 | 6.1120 | 9.03524 |
| Valid N (listwise) | 20 | | | | |
| Sum of squares | df | Mean square | F | Sig. |
|---|
| DOM_GAT | Between groups | 750.461 | 2 | 375.230 | 9.782 | 0.001 |
| Within groups | 652.089 | 17 | 38.358 | | |
| Total | 1402.550 | 19 | | | |
| NDOM_GAT | Between groups | 913.785 | 2 | 456.893 | 12.188 | 0.001 |
| Within groups | 637.292 | 17 | 37.488 | | |
| Total | 1551.077 | 19 | | | |
Multiple comparisons; showing the statistical relation between Grip Ability Test scores and Disease Activity Score 28 analysed using Analysis of Variance test.
| Tukey HSD Dependent variable | Mean difference (I-J) | Std. error | Sig. | 95% Confidence interval |
|---|
| Lower bound | Upper bound |
|---|
| DOM_GAT | Mild | Moderate | 14.8667* | 4.1289 | 0.006 | 4.274 | 25.459 |
| Severe | 18.4125* | 4.1929 | 0.001 | 7.656 | 29.169 |
| Moderate | Mild | -14.8667* | 4.1289 | 0.006 | -25.459 | -4.274 |
| Severe | 3.5458 | 3.0094 | 0.482 | -4.174 | 11.266 |
| Severe | Mild | -18.4125* | 4.1929 | 0.001 | -29.169 | -7.656 |
| Moderate | -3.5458 | 3.0094 | 0.482 | -11.266 | 4.174 |
| NDOM_GAT | Mild | Moderate | 16.17000* | 4.08182 | 0.003 | 5.6987 | 26.6413 |
| Severe | 20.36208* | 4.14510 | 0.000 | 9.7284 | 30.9958 |
| Moderate | Mild | -16.17000* | 4.08182 | 0.003 | -26.6413 | -5.6987 |
| Severe | 4.19208 | 2.97511 | 0.359 | -3.4401 | 11.8243 |
| Severe | Mild | -20.36208* | 4.14510 | 0.000 | -30.9958 | -9.7284 |
| Moderate | -4.19208 | 2.97511 | 0.359 | -11.8243 | 3.4401 |
*The mean difference is significant at the 0.05 level
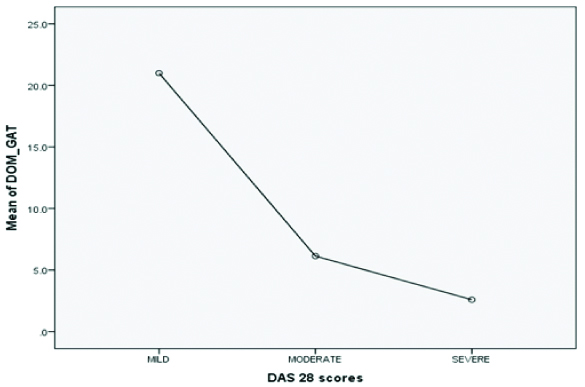
Graph representing the relationship between GAT scores of Dominant hand and DAS28 scores. Note the fall in Handgrip strength/Grip Ability in severe group.
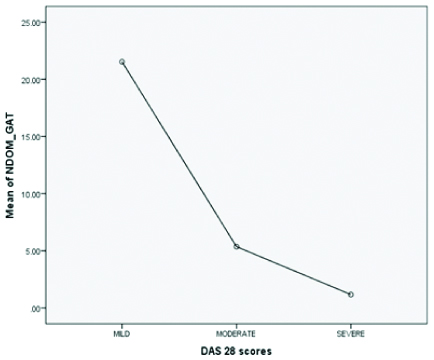
Graph representing the relation between GAT scores of Non dominant hand and DAS28 scores. Note the fall in Handgrip strength/Grip Ability in severe group.
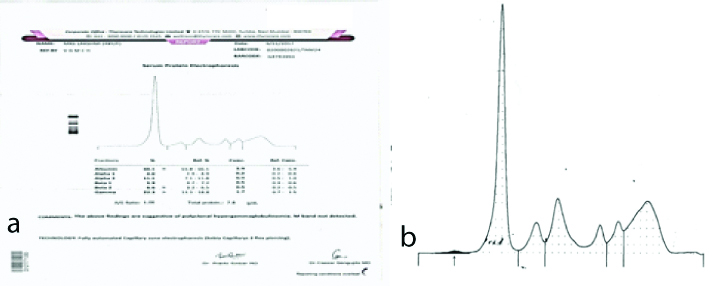
a) Figure showing the presence of “Hy” band in the prealbumin region; b) Magnified version.
The chart shows the number of people having “Hy” band in each group (Grouped according to Das28 scores).
Two sample ‘t’ test with equal variances (DOM GAT, by “Hy” band)

Table showing statistical relation between GAT scores of dominant hand and “Hy” band.
| Ha: diff <0 | Ha: diff=0 | Ha: diff >0 | | |
|---|
| Pr (T<t)=0.6360 | Pr (|T|>|t|)=0.7279 | Pr (T>t)=0.3640 | | |
|---|
| Group | Observation | Mean | Std. Err. | Std. Dev | [95% Conf. Interval] |
|---|
| Present | 14 | 7.4 | 2.451597 | 9.173037 | 2.103646 | 12.69635 |
| Absent | 6 | 5..883333 | 3.127047 | 7.733154 | -2.232114 | 13.99878 |
| Combined | 20 | 6.945 | 1.921177 | 8.591763 | 2.923931 | 10.96607 |
| Diff | | 1.516667 | 4.292371 | | -7.50127 | 10.5346 |
Diff=Mean (present)-Mean (absent); t=0.3533; Ho: Diff=0; Degrees of freedom=18
The table shows the statistical relation between Non Dominant hand Grip Ability Test scores and “Hy” band.
| Ha: diff<0 | Ha: diff=0 | Ha: diff>0 | | |
|---|
| Pr (T<t)=0.8332 | Pr (|T|>|t|)=0.3337 | Pr (T>t)=0.1668 | | |
|---|
| Group | Observation | Mean | Std. Err | Std. Dev. | 95% Confidence interval |
|---|
| Present | 14 | 7.426429 | 2.757082 | 10.31606 | 1.470115 | 13.38274 |
| absent | 6 | 3.045 | 1.702711 | 4.170773 | -1.331958 | 7.421958 |
| Combined | 20 | 6.112 | 2.020342 | 9.035244 | 1.883376 | 10.34062 |
| diff | | 4.381429 | 4.41026 | | -4.884184 | 13.64704 |
Diff=mean (present) – mean (absent); t=0.3533; Ho: diff=0; Degrees of Freedom=18
Table showing the analysis results of the correlation between Grip Ability Test scores of Dominant hand and presence of Deformity.
| Variable | Coefficient | 95% Confidence | Limits | Std. error | F-test | p-value |
|---|
| Deformity | 2.137 | -6.261 | 10.536 | 3.997 | 0.2859 | 0.599388 |
| Constant | 3.525 | -10.528 | 17.578 | 6.689 | 0.2777 | 0.604637 |
| Source | df | Sum of squares | Mean square | F-statistic | p-value |
|---|
| Regression | 1 | 21.9308 | 21.9308 | 0.2859 | 0.5994 |
| Residuals | 18 | 1380.6188 | 76.7010 | | |
| Total | 19 | 1402.5495 | | | |
Linear Regression; Outcome variable: NDOM_GAT; Co-variates: Deformity; Dummy variables: -; Interaction terms: -; Include missing: False; Correlation Coefficient: r^2= 0.02
Showing relation between Grip Ability Test scores of Non–Dominant hand and presence of Deformity.
| Variable | Coefficient | 95% Confidence | Limits | Std. error | F-test | p-value |
|---|
| Deformity | 4.637 | -3.964 | 13.237 | 4.094 | 1.2829 | 0.272224 |
| CONSTANT | -1.307 | -15.698 | 13.085 | 6.850 | 0.0364 | 0.850853 |
| Source | df | Sum of squares | Mean square | F-statistic | p-value |
|---|
| Regression | 1 | 103.1937 | 103.1937 | 1.2829 | 0.2722 |
| Residuals | 18 | 1447.8833 | 80.4380 | | |
| Total | 19 | 1551.0769 | | | |
Linear Regression
Outcome variable: NDOM_GAT; Co-variates: Deformity; Dummy variables: -; Interaction terms: -; Include missing: False; Correlation Coefficient: r^2 = 0.07
Discussion
The relation between grip strength and general disability was established by previous studies [4,5]. GAT value of the dominant hand was found to have a significant positive correlation with handgrip [19]. This confirms the validity of GAT as a measure of handgrip strength. In the present study, authors compared GAT scores with disease activity. The present study revealed significant correlation with GAT and disease activity in both dominant and non-dominant hand. This is in line with a previous study [2] which found significant negative correlation with GAT and disease activity i.e., as Disease activity increases, GAT decreases.
Functional capacity of the patient decreases most rapidly at the early stages of the disease. The functional status and initiation of therapy in their first year of RA is predictive of long-term outcome [20]. In addition, the hand grip function is a sensitive measure of therapeutic response [21]. Hence GAT will serve as a quick and trustworthy tool for predicting prognosis and optimising therapy [Table/Fig-11].
Photograph demonstrating the GAT.

The study included patients on regular medication and patients not under regular medication. The treatment compliance was enquired by history and those who were on regular follow-up (one visit per month for the past two years) were considered to be on regular medication. Most patients were on Methotrexate (n=15) and severe cases were on steroids (n=8). On observation, the patients who were said to be on regular medication were able to perform the GAT test more efficiently. Since most patients did not have proper treatment records, treatment status was not subjected to statistical analysis.
In the present study, the prime focus was to find out the relation between GAT scores (loss of hand function) and the presence of “Hy” band. RA being an autoimmune disorder is known for remissions and exacerbations. A previous study by present authors [8] was a cross-sectional study and investigated the cases only for a short period of time, authors could not asses the inflammatory features present before the time of investigation accurately and the DAS28 score is a subjective measure, calculated only from the patient’s history. Hence there might be a memory recall bias. In order to reduce this bias, GAT scores can be used as a measure of disease activity. Thus, authors analysed the correlation between GAT scores and presence of “Hy” band. The present data revealed that there is no statistically significant relation between presence of “Hy” band and GAT scores.
Limitation
Further studies are required to reveal the exact chemical nature of “Hy” band and confirm its relation with Amyloidosis in case of Rheumatoid arthritis patients. The factors influencing the presence of “Hy” band in RA patients needs to be evaluated. The therapeutic effect of increasing the retinol and retinol binding protein levels in preventing Amyloidosis in Rheumatoid arthritis patients, must be evaluated in a longitudinal study.
Conclusion
Our study concludes that the loss of hand function measured by GAT has positive correlation with disease activity. “Hy” band the surrogate marker of Amyloidosis shows no association with GAT. The treatment status of the patient is a possible confounding factor in the study. Way ahead, studies investigating the factors influencing the presence of “Hy” band are needed.
*The mean difference is significant at the 0.05 level
Diff=Mean (present)-Mean (absent); t=0.3533; Ho: Diff=0; Degrees of freedom=18
Diff=mean (present) – mean (absent); t=0.3533; Ho: diff=0; Degrees of Freedom=18
Linear Regression; Outcome variable: NDOM_GAT; Co-variates: Deformity; Dummy variables: -; Interaction terms: -; Include missing: False; Correlation Coefficient: r^2= 0.02
Linear Regression
Outcome variable: NDOM_GAT; Co-variates: Deformity; Dummy variables: -; Interaction terms: -; Include missing: False; Correlation Coefficient: r^2 = 0.07
[1]. Sollerman C, Ejeskar A, Sollerman hand function testA standardised method and its use in tetraplegic patients. Scand J Plast Reconstr Surg hand Surg 2995 29(2):267-76.10.3109/028443195090343347569815 [Google Scholar] [CrossRef] [PubMed]
[2]. Bircan Ç, Erdinç Gündüz N, Tekgül A, Çetin P, Önen F, Kizil R, Grip ability test in rheumatoid arthritis patients: Relationship with disease activity and hand-specific self-report questionnairesTurkish J Rheumatol 2024 29(3):260-66.10.5606/tjr.2014.4590 [Google Scholar] [CrossRef]
[3]. Palamar D, Er G, Terlemez R, Ustun I, Can G, Saridogan M, Disease activity, handgrip strengths, and hand dexterity in patients with rheumatoid arthritisClin Rheumatol 2027 36(20):2202-08.10.1007/s10067-017-3756-928721628 [Google Scholar] [CrossRef] [PubMed]
[4]. Sayer AA, Syddall HE, Martin HJ, Dennison EM, Roberts HC, Cooper C, Is grip strength associated with health-related quality of life? Findings from the Hertfordshire Cohort StudyAge Ageing 2006 35(4):409-25.10.1093/ageing/afl02416690636 [Google Scholar] [CrossRef] [PubMed]
[5]. Frederiksen H, Gaist D, Petersen HC, Hjelmborg J, McGue M, Vaupel JW, Hand grip strength: a phenotype suitable for identifying genetic variants affecting mid- and late-life physical functioningGenet Epidemiol 2002 23(2):220-22.10.1002/gepi.112712214305 [Google Scholar] [CrossRef] [PubMed]
[6]. Breuillé D, Obled C, Mosoni L, Mercier S, Patureau Mirand P, Chronic inflammation alters protein metabolism in several organs of adult ratsJ Nutr [Internet] 2002 232(7):2922-28.Available from: https://doi.org/20.2093/jn/232.7.292210.1093/jn/132.7.192112097671 [Google Scholar] [CrossRef] [PubMed]
[7]. Gruys E, Toussaint MJM, Niewold TA, Koopmans SJ, Acute phase reaction and acute phase proteinsJ Zhejiang Univ Sci [Google Scholar]
[8]. SwethaVarsha GJ, Senthilkumari KR, “Hy”band-a surrogate marker for the risk of Amyloidosis in Rheumatoid ArthritisBiomedicine 2028 38(2):70-73. [Google Scholar]
[9]. Ropes MW, Perlmann GE, Kaufman D, Bauer W, The electrophoretic distribution of proteins in plasma in rheumatoid arthritisJ Clin Invest 2954 33(3):322-28.10.1172/JCI10289913143075 [Google Scholar] [CrossRef] [PubMed]
[10]. Costa PP, Figueira AS, Bravo FR, Amyloid fibril protein related to prealbumin in familial amyloidotic polyneuropathyProc Natl Acad Sci U S A [Internet] 2978 75(9):4499-503.10.1073/pnas.75.9.4499279930 [Google Scholar] [CrossRef] [PubMed]
[11]. Westermark P, Sletten K, Johansson B, Cornwell GG, Fibril in senile systemic amyloidosis is derived from normal transthyretinProc Natl Acad Sci [Internet] 2990 87(7):2843-45.10.1073/pnas.87.7.28432320592 [Google Scholar] [CrossRef] [PubMed]
[12]. Gertz MA, Benson MD, Dyck PJ, Grogan M, Coelho T, Cruz M, Diagnosis, Prognosis, and Therapy of Transthyretin AmyloidosisJ Am Coll Cardiol 2025 66(22):2452-66.10.1016/j.jacc.2015.09.07526610878 [Google Scholar] [CrossRef] [PubMed]
[13]. Galant NJ, Westermark P, Higaki JN, Chakrabartty A, Transthyretin amyloidosis: an under-recognized neuropathy and cardiomyopathyClin Sci (Lond) 2027 232(5):395-409.10.1042/CS2016041328213611 [Google Scholar] [CrossRef] [PubMed]
[14]. Wei S, Episkopou V, Piantedosi R, Maeda S, Shimada K, Gottesman ME, Studies on the metabolism of retinol and retinol-binding protein in transthyretin-deficient mice produced by homologous recombinationJournal of Biological Chemistry 2995 270:866-70.10.1074/jbc.270.2.8667822324 [Google Scholar] [CrossRef] [PubMed]
[15]. Aletaha D, Neogi T, Silman AJ, Funovits J, Felson DT, Bingham CO, 2020 Rheumatoid arthritis classification criteria: An American College of Rheumatology/European League Against Rheumatism collaborative initiativeArthritis Rheum 2020 62(9):2569-82.10.1002/art.2758420872595 [Google Scholar] [CrossRef] [PubMed]
[16]. Pereira IA, Kairalla RA, Mota LMH da, Fronza LSR, Kawassaki A de M, Bernardo WM, Guidelines for the diagnosis of rheumatoid arthritisRev Bras Reumatol Campinas 2023 53(2):242-257.10.1016/S2255-5021(13)70019-1 [Google Scholar] [CrossRef]
[17]. Poole JL, Cordova KJ, Brower LM, Reliability and validity of a self-report of hand function in persons with rheumatoid arthritisJ Hand Ther 2006 29(2):22-26.quiz 2710.1197/j.jht.2005.10.00116473729 [Google Scholar] [CrossRef] [PubMed]
[18]. Carpenter L, Norton S, Nikiphorou E, Kiely P, Walsh DA, Dixey J, Score (DAS) to the DAS28Rheumatol Int [Internet] 2028 38(22):2297-305.10.1007/s00296-018-4184-030368562 [Google Scholar] [CrossRef] [PubMed]
[19]. Dellhag B, Bjelle A, A grip ability test for use in rheumatology practiceJ Rheumatol 2995 22(8):2559-65. [Google Scholar]
[20]. Mota LMH, Cruz BA, Brenol CV, Pereira IA, Rezende-Fronza LS, Bertolo MB, Diretrizes para o tratamento da artrite reumatoide Guidelines for the drug treatment of rheumatoid arthritisRev Bras Reumatol 2023 53(2):258-83.10.1590/S0482-5004201300020000423856794 [Google Scholar] [CrossRef] [PubMed]
[21]. Eberhardt K, Sandqvist G, Geborek P, Hand function tests are important and sensitive tools for assessment of treatment response in patients with rheumatoid arthritisScand J Rheumatol [Internet] 2008 37(2):209-22.10.1080/0300974070174712918415767 [Google Scholar] [CrossRef] [PubMed]