Endodontic Management of Maxillary First Molar Teeth with Double Canal System in Each Root: A Case Series
Sana Farooq1, Mousumi Goswami2, Tanu Nangia3, Bushra Rahman4, Shriyam Sharan5
1 Student, Department of Pedodontics, ITS Dental College, Hospital and Research Centre, Greater Noida, Uttar Pradesh, India.
2 Professor and Head, Department of Pedodontics, ITS Dental College, Hospital and Research Centre, Greater Noida, Uttar Pradesh, India.
3 Reader, Department of Pedodontics, ITS Dental College, Hospital and Research Centre, Greater Noida, Uttar Pradesh, India.
4 Student, Department of Pedodontics, ITS Dental College, Hospital and Research Centre, Greater Noida, Uttar Pradesh, India.
5 Student, Department of Pedodontics, ITS Dental College, Hospital and Research Centre, Greater Noida, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Sana Farooq, ITS Dental College and Hospital, Near Surya Hospital, 47, Knowledge Park III, Greater Noida, Uttar Pradesh, India.
E-mail: sanafarooq0000@gmail.com
The root canal aberrations and variations in maxillary first permanent molars is a constant challenge and successful endodontic management with latest adjuncts decreases the failure of missing a canal. We present a series of three cases of maxillary first permanent molar with six canals wherein it was noted an unusual morphology of double canal system in each root using recent adjuncts like Cone Beam Computed Tomography, endodontic microscope and magnifying loupes.
Cone beam computed tomography, Vertucci, Wein
Case Series
The importance of having the adequate knowledge to recognise and diagnose additional root canals especially in the maxillary permanent molars in children and adolescents and their locations with respect to the main respective canal determines the endodontic success of the tooth. This case series discusses the successful endodontic management of permanent maxillary first molars with double canal systems in each root.
Case 1
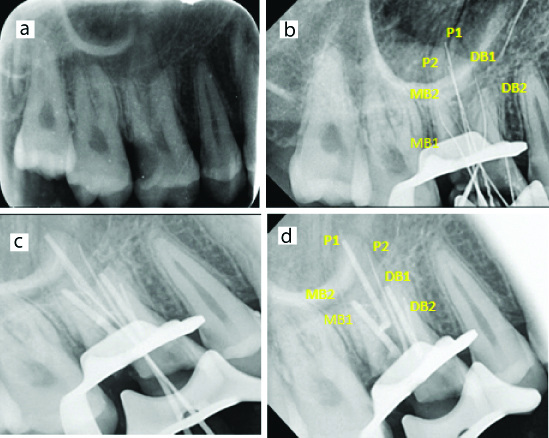
A 13-year-old male patient reported to the Department of Pedodontics with chief complaint of spontaneous pain in the right upper back tooth that aggravated on lying down at night and relieved by analgesics. On examining the tooth was tender to percussion. Cold test revealed no response and delayed response with electric pulp test. The tooth was diagnosed with irreversible pulpitis [Table/Fig-1a]. Anaesthesia was achieved with 1.8 mL of lidocaine hydrochloride containing 1:200,000 adrenaline (Themicaine AD) using inferior alveolar nerve block followed by rubber dam isolation. A triangular access cavity was modified to trapezoidal one revealed 3 principal root canal systems. Small haemorrhagic points were noted on probing with a sharp DG16 endodontic explorer (Hu-Friedy, Chicago, IL) 2 mm palatal to the MB and DB canals suggesting extra canals. Working length was established by placing pathfinder files no 10. There seemed 2 distinct apical foramina in all three roots. The biomechanical preparation was performed using ProTaper Nickel-Titanium rotary instruments (Neoendo rotary files) using crown down technique with copious irrigation using 2.5% sodium hypochlorite solution. The canals were dried with paper points and calcium hydroxide dressing was placed with a lentirospiral (MANI paste carriers) for two weeks. An interim restoration of Cavit (3 M Espe, Germany) was placed in the pulp chamber.
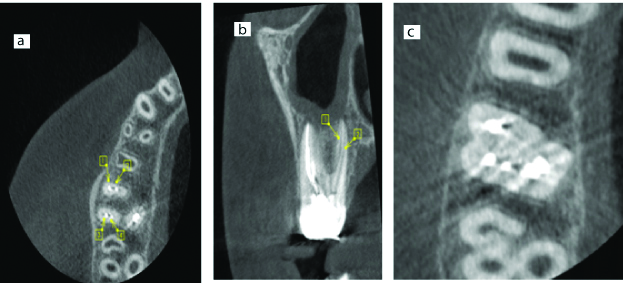
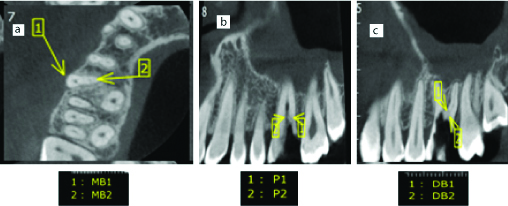
After confirming with a master cone radiograph [Table/Fig-1b], all the 6 canals were obturated [Table/Fig-1c]. The tooth was restored with a miracle mix (GC Corporation, Tokyo) and a stainless steel crown was placed [Table/Fig-1c]. To confirm this unusual canal morphology CBCT [Table/Fig-2] imaging was done which confirmed the presence of six canals post obturation.
a) Diagnostic radiograph irt 16; b) Master cone radiograph irt 16; c) Obturation and Stainless steel crown irt 16.
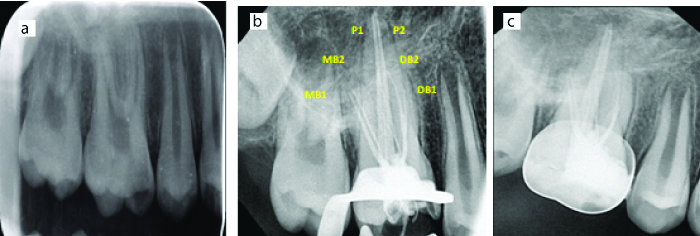
CBCT images: a) 1) MB1 2) MB2 3) DB1 4) DB2; b) 1) MP 2) DP; c) Axial sections showing 6 canals.
Case 2
An 18-year-old male patient reported to Department of Pedodontics with an intermittent type of pain in left upper back tooth region since 1-week which increased on lying down. A diagnosis of chronic irreversible pulpitis was made irt 26 [Table/Fig-3a].
a) Diagnostic radiograph irt 26; b) Working length radiograph irt 26; c) Obturation radiograph irt 26.
Under rubber dam isolation, access cavity was prepared with endo access bur (Dentsply, Switzerland). Working length was determined with the help of ISO 10 K-file. A total of six root canals were identified [Table/Fig-3b]. Instrumentation with ProTaper rotary Ni-Ti instruments (Neoendo rotary files) using crown down technique followed by irrigation with 5.25% sodium hypochlorite. The cavity was sealed with interim restoration. CBCT images [Table/Fig-4] confirmed presence of 6 canals. Calcium hydroxide dressing was placed and patient recalled after three weeks. Obturation [Table/Fig-3c] of six canals with gutta-percha cones (Aurum pro, Meta biomed, Korea) was done followed by a composite restoration and a crown.
Cone Beam Computed Tomography cross sections in various planes.
Case 3
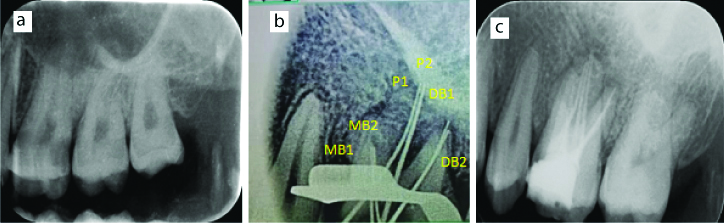
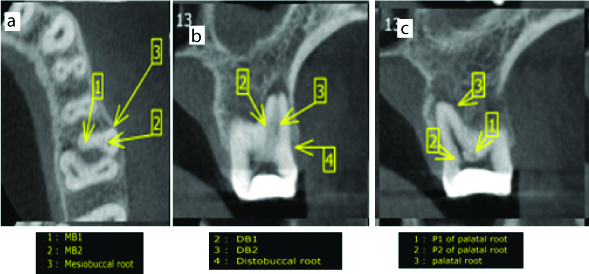
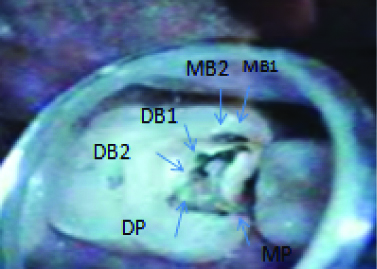
An 18-year-old male patient presented to the Department of Pedodontics with a chief complaint of intermittent pain in upper right back tooth region since 5 days. A negative response was elicited with electronic pulp stimulation and chronic irreversible pulpitis irt 16 was diagnosed [Table/Fig-5a]. An endodontic access cavity was established after administering local anaesthesia. DG 16 endodontic explorers revealed MB2 as a small haemorrhagic pin point palatal to the main MB orifice and accessory palatal canal distal to the main palatal canal. Working length radiograph [Table/Fig-5b] and CBCT confirmed 6 canals [Table/Fig-6]. Biomechanical preparation with Protaper nickel-titanium rotary instruments followed by irrigation with normal saline, 2.5% sodium hypochlorite solution, 17% EDTA and 2% chlorhexidine digluconate was done. Under a dental operative microscope (7X, Seiler IQ, Chicago, USA) additional canals were identified [Table/Fig-7]. The canals were dried and tooth sealed with temporary filling material. The following week all canals obturated using gutta-percha [Table/Fig-5c,d]. The tooth was restored with a posterior composite resin (3M Dental Products, St Paul, MN) and a porcelain fused to metal crown.
a) Diagnostic radiograph irt 16; b) Working length radiograph irt 16; c) Obturation radiograph irt 16; d) Obturation radiograph showing double canals irt 16.
Cone Bean Computed Tomography cross sections in various planes.
Microscopic endodontic picture irt 16.
Discussion
The inability to recognise variations may leave additional canals undiagnosed, infected and non-treated leading to endodontic failure [1]. The incidence of a fourth canal as Mesiobuccal MB2 ranges between 50.4% to 95% and a fifth canal is 2.25% [2]. Maxillary first molar is the commonly treated tooth with frequent failures due to undetected canals, mostly the mesiobuccal second canal MB2. Also, there are limited chances to find MB2 in maxillary second molars [3]. Alavi AM et al., and Thomas RP et al., reported double canals in the distobuccal root as 1.90% and 4.30% respectively [4,5]. The incidence of two canals in the palatal root is 2% to 5.1% [6,7]. Case reports with five to eight canals have been reported but they are mostly in vitro studies [8]. Weine FS et al., concluded that the maximum number of failures in maxillary first molars is due to MB root [9]. The frequency of MB2 was 92.85% based on (in vitro results), 95.63% (clinical results) and 95.45% (CBCT results), whereas DB2 showed 1.15% (in vitro) and 3.75% (clinically) and P2 amounted to 2.05% (in vitro), 0.62% (clinically) and 4.55% (CBCT) of cases [10,11]. Weine FS et al., reported MB2 to be 71.1%, 62.5%, and 17.2% when viewed using microscope, dental loupes, and unaided respectively [9].
Diagnostic measures like use of magnifying loupes (4.5 magnification), multiple radiograph, examining pulpal floor with DG16 endodontic explorer, troughing of grooves with ultrasonic tips, staining chamber floor with 1% methylene blue dye, performing hypochlorite champagne bubble test and visualising canal bleeding points help in locating root canal orifices [12]. Clinicians using an endodontic microscope are significantly more likely to locate an MB2 canal (which often has a microscopic orifice) or additional canals to the 3-4 typically found in maxillary molars compared to the unaided ones [13,14]. Microcomputed Tomography X-ray has revealed 10.53% of first permanent molar had 6 pulp canal orifices, 35.09% had 5 pulp canal orifices, 47.37% had 4 pulp canal orifices and 7.01% had 3 pulp canal orifices [15].
In the present case series firstly proper exploration of the pulpal floor dentinal map and locating haemorrhagic points followed by use of loupes and endoscopic microscope for magnification helped to locate additional canals. Though radiographic examination is a gold standard however due to superimposition of canals CBCT is the best intervention which must be advised judiciously.
To confirm the unusual morphology a multiple slice CBCT scan (Care stream CS9300 select) was performed with CS 9300 scanner at resolution (0.20 mm × 0.20 mm × 0.20 mm) with FOV 5×5, tube voltage of 100KV and tube current of 8 mA was taken after informed consent. The tooth morphology was obtained in transverse, axial, and sagittal cross-sections at 1 mm interval of 0.5 mm thickness.
The first case showed palatal root with Vertucci type V, distobuccal and mesiobuccal with Vertucci type IV and Weines type III classification. In second case Weines type III and Vertucci type IV classification in mesial, distal and palatal root was observed. In third case Weines type III and Vertucci type IV classification was seen.
The working length was estimated by means of an electronic apex locator (Root ZX; Morita, Tokyo, Japan). The radiographs and CBCT confirmed the unusual simultaneous presence of double canal system.
Conclusion
A successful endodontic management demands a knowledgeable and well equipped clinician ready to encounter any anatomical variations and presence of additional root canals in first permanent molar teeth even if a rare incidence is seen. A proper illumination for visualisation of pulpal floor, use of DG16 endodontic explorer and use of latest adjuncts like CBCT, magnifying loupes and endodontic microscope decreases the endodontic failure caused by neglecting extra canals.
[1]. Sharma S, Mittal M, Passi D, Grover S, Management of a maxillary first molar having atypical anatomy of two roots diagnosed using cone beam computed tomographyJ Conserv Dent 2015 18(4):342-45.10.4103/0972-0707.15975626180423 [Google Scholar] [CrossRef] [PubMed]
[2]. Kaushik M, Mehra N, Maxillary first molars with six canals diagnosed with the aid of cone beam computed tomography: a report of two casesCase Reports in Dentistry 2013 2013:40692310.1155/2013/40692323984111 [Google Scholar] [CrossRef] [PubMed]
[3]. Shah M, Patel P, Desai P, Patel JR, Anatomical aberrations in root canals of maxillary first and second molar teeth: an endodontic challengeBMJ Case Rep 2014 2014:bcr201320131010.1136/bcr-2013-20131024445844 [Google Scholar] [CrossRef] [PubMed]
[4]. Alavi AM, Opasanon A, Ng YL, Gulabivala K, Root and canal morphology of Thai maxillary molarsInt Endod J 2002 35(5):478-85.10.1046/j.1365-2591.2002.00511.x12059921 [Google Scholar] [CrossRef] [PubMed]
[5]. Thomas RP, Moule AJ, Bryant R, Root canal morphology of maxillary permanent first molar teeth at various agesInt Endod J 1993 26:257-67.10.1111/j.1365-2591.1993.tb00570.x8300257 [Google Scholar] [CrossRef] [PubMed]
[6]. Stone LH, Stroner WF, Maxillary molars demonstrating more than one palatal root canalOral Surg Oral Med Oral Pathol 1981 51:649-52.10.1016/S0030-4220(81)80017-56942365 [Google Scholar] [CrossRef] [PubMed]
[7]. Al Qahtani A, Abdulrab S, Alhadainy H, Management of a failed endodontic treatment for a maxillary second molar with two separate palatal rootsClin Case Rep 2018 6(9):1735-38.10.1002/ccr3.1708 [Google Scholar] [CrossRef]
[8]. Kottoor J, Velmurugan N, Surendran S, Endodontic management of a maxillary first molar with eight root canal systems evaluated using cone-beam computed tomography scanning: A case reportJ Endod 2011 37:715-19.10.1016/j.joen.2011.01.00821496678 [Google Scholar] [CrossRef] [PubMed]
[9]. Weine FS, Healey HJ, Gerstein H, Evanson L, Canal configuration in the mesiobuccal root of the maxillary first molar and its endodontic significanceOral Surg Oral Med Oral Pathol 1969 28:419-25.10.1016/0030-4220(69)90237-05257186 [Google Scholar] [CrossRef] [PubMed]
[10]. Du Y, Soo I, Zhang CF, A case report of six canals in a maxillary first molarChin J Dent Res 2011 14(2):151-53. [Google Scholar]
[11]. Martinez-Berna A, Ruiz-Badanelli P, Maxillary first molars with six canalsJ Endod 1983 9(9):375-81.10.1016/S0099-2399(83)80188-56579196 [Google Scholar] [CrossRef] [PubMed]
[12]. Vertucci FJ, Root canal morphology and its relationship to endodontic proceduresEndod Top 2005 10:03-29.10.1111/j.1601-1546.2005.00129.x [Google Scholar] [CrossRef]
[13]. Mamoun JS, The maxillary molar endodontic access opening: A microscope-based approachEur J Dent 2016 10(3):439-46.10.4103/1305-7456.18415327403069 [Google Scholar] [CrossRef] [PubMed]
[14]. Kakkar P, Singh A, Maxillary first molar with three mesiobuccal canals confirmed with spiral computer tomographyJ Clin Exp Dent 2012 4:e256-59.10.4317/jced.5085024558566 [Google Scholar] [CrossRef] [PubMed]
[15]. Ashiry EAE, Farsi NM, Prevalence of extra root canal orifices of maxillary first permanent molars in a saudi subpopulation utilizing microcomputed tomographyJ Contemp Dent Pract 2018 19(11):1312-16.10.5005/jp-journals-10024-2424 [Google Scholar] [CrossRef]