Asymmetric Skeletal Open Bite Treated with Unilateral Sagittal Split Osteotomy and Tongue Reduction
Jasmine Nindra1, Maninder Singh Sidhu2, Namrata Dogra3, JK Dayashankara Rao4, Seema Grover5
1 Senior Lecturer, Department of Orthodontics, SGT University, Gurgaon, Haryana, India.
2 Professor and Head, Department of Orthodontics, SGT University, Gurgaon, Haryana, India.
3 Senior Lecturer, Department of Orthodontics, SGT University, Gurgaon, Haryana, India.
4 Professor and Head, Department of Oral Surgery, SGT University, Gurgaon, Haryana, India.
5 Professor, Department of Orthodontics, SGT University, Gurgaon, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Namrata Dogra, Senior Lecturer, Department of Orthodontics, SGT University, Gurgaon, Haryana-122505, India.
E-mail: namratasgt@gmail.com
Treatment of mandibular asymmetry with skeletal open bite poses big challenge for orthodontists. Presence of macroglossia is another aggravating factor that makes open bite worse. Masticatory function is highly compromised in cases where anterior open bite extends to posterior regions. Treatment of mandibular asymmetry with complete anterior and posterior open bite with occlusal canting has not been described in the past. There are very few case reports which describe treatment of severe open bite with contact only in second molar regions. Bilateral Sagittal Split Osteotomy is preferred surgical option for most mandibular asymmetries but unilateral sagittal split osteotomy has been attempted by very few. This case report describes treatment of Asymmetric Skeletal Openbite with customised surgical procedure in combination with orthodontics. Here, anterior and posterior open bite was treated with Unilateral Sagittal Split Osteotomy (USSO), paramedian ostectomy and partial glossectomy. After the treatment, the patient’s masticatory function was enhanced in addition to improvement in aesthetics.
Macroglossia, Paramedian ostectomy, Partial glossectomy
Case Report
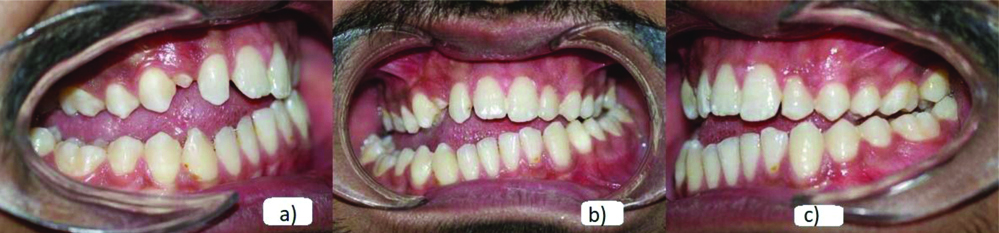
A 20-year-old male patient, presented to Department of Orthodontics with chief complaint of inability to close upper and lower teeth since childhood. He was concerned about his appearance on smiling and difficulty in chewing. Patient had visited a private dentist at the age of 12 years when his upper left canine was extracted by him since it was erupting out of the arch and was told by the dentist that his skeletal malrelationship could not be corrected and requires surgical intervention. Patient did not have any relevant medical history. Patient gave history of accident when he was 16 years of age, he fell on right side of the face, after which his inability to close the teeth became more noticeable to him. Patient had consulted other private dentists and was referred to this university for a thorough examination and treatment. He also gave history of extracted canine in upper left front region. Extraoral examination revealed facial asymmetry with chin deviated towards right side and depressed nasal bridge [Table/Fig-1]. Patient gave history of dull constant pain on right side of cheek and in front of the ear, however only while eating hard foods. On TMJ palpation no abnormality was detected. The mastication was mainly unilateral on the left side. Mandibular movements were normal. Intraoral examination revealed complete anterior and posterior open bite, more on the right side with contact only at left upper and lower second molars [Table/Fig-2]. U-shaped maxillary arch with missing upper left canine and a partially erupted upper right canine and broad squarish mandibular arch were found [Table/Fig-3]. Imprints of posterior teeth were observed on the lateral aspect of tongue that indicated true macroglossia [1]. The patient exhibited a grossly enlarged and wide, broad and flat tongue, Open bite in anterior as well as posterior teeth, Chronic posturing of the tongue between the teeth at rest, infraoccluded lower right posterior molars, Crenations on the tongue, along with lateral tongue thrust habit confirming the presence of macroglossia.
a) Pre-treatment Extraoral frontal photograph; b) Pre-treatment Extraoral photograph showing anterior teeth; c) Pre-treatment Extraoral profile photograph.

a) Pre-treatment Intraoral right lateral photograph; b) Pre-treatment Intraoral frontal photograph; c) Pre-treatment Intraoral left lateral photograph.
a) Pre-treatment Occusal maxillary photograph; b) Pre-treatment Occlusal mandibular photograph.

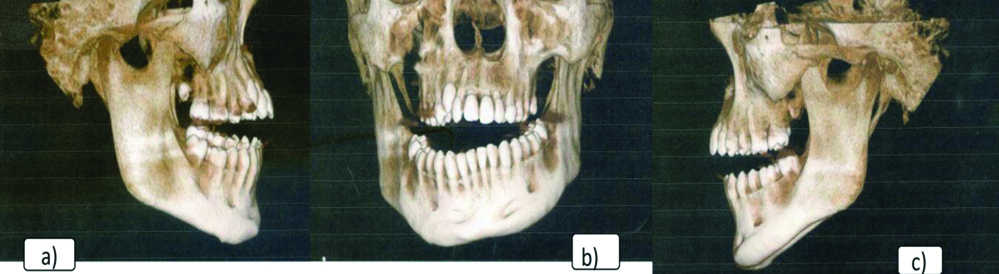
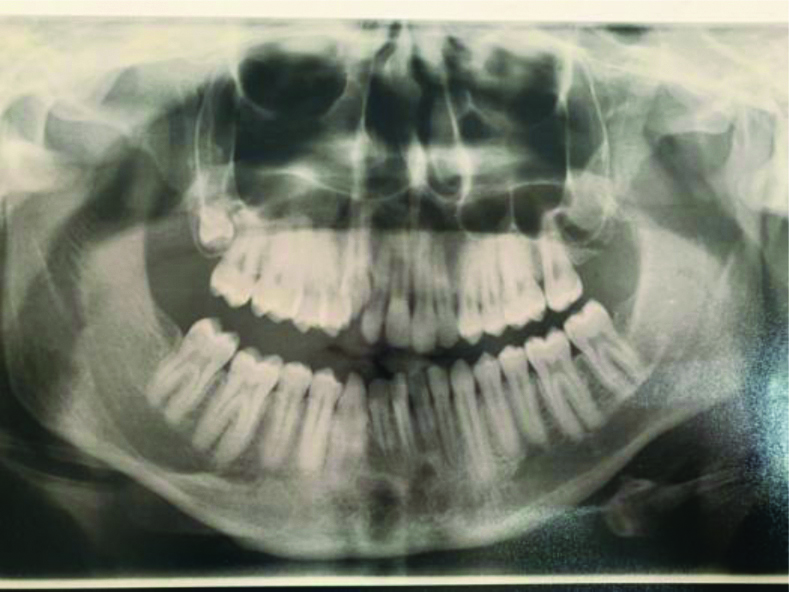
Patient was advised to get a CBCT scan done since the patient presented with skeletal malrelationship that required a three-dimensional radiological examination to obtain information regarding the cause of the patient’s facial asymmetry and examine any abnormalities in the TMJ area which is not clearly appreciable on the OPG or Lateral cephalogram. On CBCT evaluation, skeletal open bite was evident [Table/Fig-4]. Right condylar head was hyperplastic mediolaterally with decreased height of sub-condylar region. Shallow sigmoid notch on right side and a well-formed coronoid process was seen. The right zygomatico-maxillary region was not well formed which might have led to the constriction of maxillary arch. No abnormalities were seen in relation to left side condylar and zygomatico-maxillary region. Deviation of nasal septum towards right side was evident with hypertrophied right inferior turbinate. Integrity of nasal bone and cartilage was seen to be compromised. CBCT derived Pre-treatment OPG showed partially erupted upper right canine [Table/Fig-5].
a) Pre-treatment right lateral CBCT; b) Pre-treatment frontal CBCT; c) Pre-treatment left lateral CBCT.
*It was noticed that there was a breach in the continuity of zygomatic bone in image b). Also, the patient had a history of fall at the age of 16 years which suggested that there may be a fracture in that region, but the patient showed no clinical sign and symptoms of fracture since his accident. On deeply studying the CBCT, it was found that on the right side, the zygomatic maxillary region was not well formed. No symptoms of pain were reported by the patient, thus there was no fracture. Also, in [Table/Fig-10], the break in the continuity of zygomatic bone on the right side is not present. Hence, no significance was attached.
Pre-treatment OPG derived from CBCT.
Clinical examination showed that the patient had asymmetrical skeletal open bite deformity, with facial asymmetry due to hyperplasia of right condylar head and malformed right zygomatico-maxillary region leading to constricted maxillary arch and a broader mandibular arch and macroglossia with lateral tongue thrusting habit.
Treatment Objectives
To improve maxillomandibular skeletal and dental relationship in order to correct the complex open bite such that patient’s masticatory ability is enhanced thereby providing improved oral health quality of life.
Correction of occlusal canting
To coordinate upper and lower arches
To establish ideal overjet and overbite
Treatment Progress
The treatment plan was discussed with the patient and an informed consent was obtained. Maxillary arch was bonded using .022”×.028” pre-adjusted edgewise MBT appliance prescription. (Di MIM Mini Twin Bracket system, Ortho organisers, A Henry Schein Company). The arch wire sequence proceeded as .014” NiTi, .016” NiTi, .016” Australian and 0.016×0.022” NiTi, for initial leveling and alignment. NiTi expander was placed to expand the maxilla. The upper right lateral incisor was extracted to create space for erupting upper right canine. Lower premolars were bonded and short vertical elastics were given for 3 months from lower premolars and molar to their antagonists in upper arch. Progressively more rigid stainless-steel wires were placed in the maxillary arch.
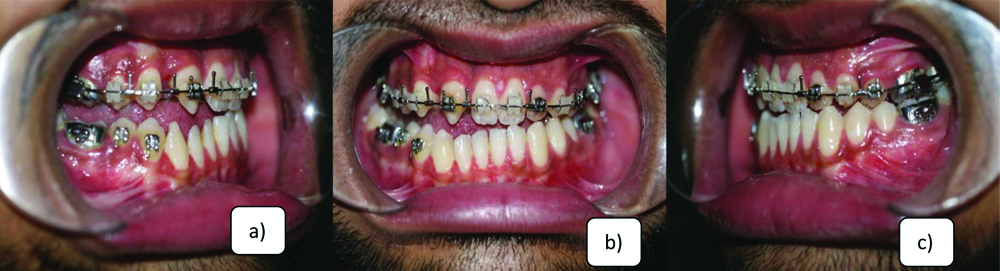
After 14 months of presurgical orthodontics, patient was prepared for surgery and upper 0.019”×0.025” stainless steel wire with crimpable hooks was placed [Table/Fig-6]. Mock surgery was planned using Hanau semi-adjustable articulator. Unilateral Sagittal Split Osteotomy was done on right side to close the open bite surgically. In this procedure, on the right lateral aspect of mandible, a vertical cut was made downwards from external oblique ridge through outer cortex to lower border where the lower border was sectioned and the split outer segment was lifted upwards in occlusion to close the open bite surgically [2]. Paramedian mandibular ostectomy was done to constrict the expanded mandibular arch. In this procedure right lower lateral incisor was extracted to facilitate the placement of surgical cut and two vertical osteotomy cuts were made followed by removal of a segment of bone from that area [3]. The middle dorsal part of tongue was resected by the method of Harada and Enomoto [Table/Fig-7] [4].
a) Presurgical Intraoral right lateral photograph; b) Presurgical Intraoral frontal photograph; c) Presurgical Intraoral left lateral photograph.
a) Tongue resection being done; b) Rigid internal fixation done on right side; c) Paramedian mandibular ostectomy.

After these surgical procedures, intermaxillary fixation was done to stabilise the osteotomised sections after surgery [Table/Fig-8]. Post-surgical orthodontics was started 1 week after surgery and Mandibular arch was leveled and aligned [Table/Fig-9]. Elastics were given for settling the occlusion. Postsurgical orthodontics continued for 7 month. Since gingival health of patient was compromised so thorough scaling was performed and chlorhexidine mouth rinse was prescribed to the patient. Before debonding, the upper right canine was reshaped into lateral incisor for aesthetics. Upper hawleys appliance with cribs lingual to canine, premolar and molars region was given. In lower arch fixed retention was used.
Intermaxillary fixation done after surgical procedure.

a) Postsurgical Intraoral right lateral photograph; b) Postsurgical Intraoral frontal photograph; c) Postsurgical Intraoral left lateral photograph.

After 22 months of treatment duration there was a dramatic improvement in severe anterior and posterior open bite providing functional occlusion to the patient [Table/Fig-10,11]. Normal overjet and overbite was achieved with Angle’s Class II molar relation [Table/Fig-12,13]. Thus, patient’s masticatory function was completely rehabilitated. CBCT derived post treatment OPG showed fully eruped upper right canine [Table/Fig-149]. CBCT derived frontal cephalogram tracing shows significant correction of mandibular asymmetry and improvement in occlusal cant [Table/Fig-15,16 and 17]. Thus, there was significant improvement in aesthetics and function. One year follow-up was done and there was slight relapse of open bite correction. This could be attributed to abnormal tongue position and functioning. To avoid this the patient was instructed to perform orofacial myofunctional therapy and was asked to wear the tongue crib retainer continuously [Table/Fig-18].

a) Post-treatment Extraoral frontal photograph; b) Post-treatment Extraoral photograph showing anterior teeth; c) Posttreatment Extraoral profile photograph.

a) Post-treatment Intraoral right lateral photograph; b) Post-treatment Intraoral frontal photograph; c) Post-treatment Intraoral left lateral photograph.

a) Post-treatment maxillary arch; b) Post-treatment mandibular arch.

CBCT derived Post-treatment OPG.

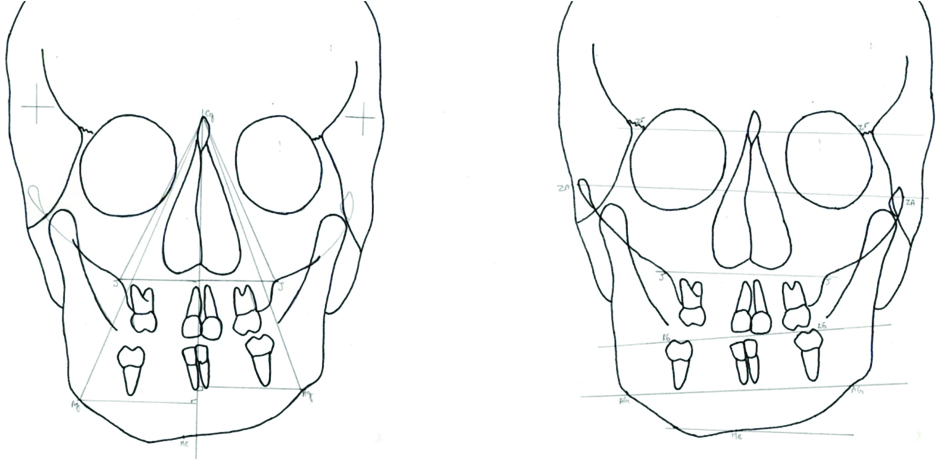
a) Pre-treatment marked mandibular asymmetry; b) Pre-treatment occlusal cant.
Post-treatment mandibular symmetry; b) Post-treatment occlusal cant correction.
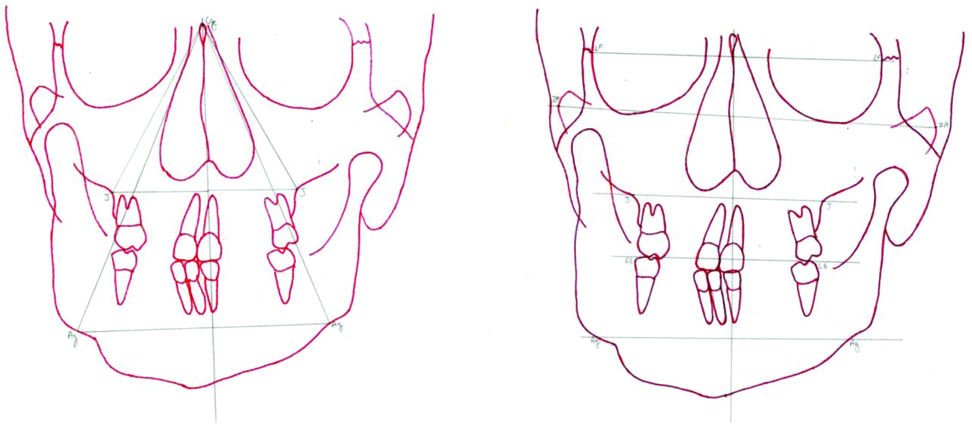
Grummons frontal asymmetry analysis.
| Parameter | Pre-treatment right | Pre-treatment left | Post-treatment right | Post-treatment left |
|---|
| Mandibular Morphology triangle |
| Co-Me | 86 | 90 | 97 | 91 |
| Co-Ag | 63 | 60 | 67 | 57 |
| Ag-Me | 37 | 42 | 46 | 44 |
| Me-Co-Ag | 230 | 240 | 25 | 22 |
| Co-Me-Ag | 430 | 350 | 38 | 30 |
| Co-Ag-Me | 1150 | 1220 | 1170 | 1290 |
| Maxilla-mandibular comparison of Asymmetry |
| Cg-J | 60 | 60 | 60 | 62 |
| Cg-MSR | 54 | 54 | 52 | 53 |
| MSR-J | 26 | 26 | 30 | 29 |
| Cg-Ag | 103 | 98 | 108 | 106 |
| Ag-MSR | 39 | 35 | 44 | 42 |
| Cg-MSR | 95 | 91 | 99 | 99 |
a) One year Post-treatment Intraoral right lateral photograph; b) One year Post-treatment Intraoral frontal photograph; c) One year Post-treatment Intraoral left lateral photograph.

Discussion
Skeletal open bite is a malocclusion in vertical plane which is most difficult to treat orthodontically [5,6]. This deformity not only compromises the aesthetics of the patient but also hampers mastication when posterior open bite is present. An enlarged tongue may create orthodontic and orthognathic instability, dento-muskulo-skeletal deformities as well as masticatory and speech problems [1]. In the literature, severe open bite cases have been treated with ortho-surgical approach. In a case reported by Nitin VM et al., adult Class III male patient with anterior open bite and facial asymmetry was treated orthosurgically with Lefort I advancement and asymmetrical bilateral sagittal split osteotomy [7]. Asymmetric osteotomy was done to correct mandibular asymmetry. In another case described by Vadgaonkar V et al., adult male patient with severe vertical dysplasia with a large open bite was treated with Le Fort 1 superior repositioning of maxilla and mandibular BSSO [8]. Buyukcavus MH also reported adult high angle, skeletal open bite case which was treated by maxillary posterior impaction and mandibular BSSO [9].
Recently, Park JH has described correction of anterior open bite in adult male with LeFort I osteotomy and down-fracture of anterior maxilla to correct open bite and BSSO for correcting mandibular asymmetry [10]. Thus, mostly anterior open-bite cases are corrected by posterior maxillary impaction and the consequent mandibular auto-rotation closes the open bite. In this patient, there was no skeletal deformity in maxilla; mandible however was skeletally asymmetrical with chin deviation to right side. Also, there was occlusal canting due to asymmetric open bite that was greater in magnitude on right side. Thus this complex case of skeletal deformity demanded customised treatment plan. Due to extreme severity of the case the treatment plan did not allow the compensatory treatment, surgical option being the only possible option. Thus, such a surgery was required which corrected mandibular deviation along with correction of severe open bite on right side. So, Depending upon patient requirement, Sagittal split osteotomy on one side, unlike conventionally performed Bilateral sagittal split osteotomy was done.
In the present case report, complete open bite with no occlusal contact anteriorly or posteriorly with mandibular asymmetry and macroglossia was treated by mandibular surgery and orthodontics. To maximise the treatment outcome and efficiency, atypical orthognathic surgery was carried out. Initially maxillary arch expansion was carried out to coordinate with the expanded mandibular arch. Due to insufficient space gain from expansion; upper right lateral incisor was extracted. Extrusion of posterior teeth was carried out as part of presurgical orthodontics. Trauner R et al., introduced Sagittal Split Ramus Osteotomy (SSO) for correcting mandibular prognathism, retrognathism, and asymmetry [11].
Unilateral sagittal split osteotomy has been recently introduced for correction of mandibular laterognathism. In a recent report, unilateral sagittal split osteotomy was used to correct lateral deviation of the mandible in 3 cases and yielded favorable outcomes. It was concluded that this technique could be considered a useful mandibular orthognathic surgical technique for reducing operation time and the incidence of postoperative complications [12]. Also, recently this surgical procedure has been successfully done on 31 cases of mandibular asymmetry and results showed long term occlusal stability with this procedure [13]. In our case there was need of surgical correction only on right side as the open bite was severe on that side only. Thus, USSO was preferred over Bilateral sagittal split osteotomy for this patient.
USSO was done only on right side of mandible and mandibular segment was lifted up to facilitate closure of bite on right side. Mandibular midline osteotomy/ostectomy associated with a BSSO is useful surgical technique when dealing with transverse maxillo-mandibular discrepancies [14,15]. This technique decreases the intercanine diameter and modulates the intermolar contraction according to the aesthetic and occlusal indications. Parasymphyseal mandibular ostectomy was also done to reduce size of expanded mandible and to achieve positive overjet [16]. Midline osteotomy was not done due to attachment of muscles on lingual tubercle of mandible. It is well known that the size and position of tongue can affect skeletal and dental components [17]. Open bite is many times caused by macroglossia and this macroglossia can be treated by partial glossectomy [18]. As the patient presented with macroglossia, partial glossectomy was done using Harada and Enomoto method [4].
Remarkable improvement was achieved in present severe open bite case which met patient’s expectations.
Conclusion
In this case, Treatment of mandibular asymmetry with severe open bite and occlusal canting was successfully accomplished with USSO, paramedian ostectomy and partial glossectomy procedure in combination with orthodontics. The treatment plan not only improved aesthetics of the patient significantly but also restored masticatory function.
[1]. Wolford LM, Cottrell DA, Diagnosis of macroglossia and indications for reduction glossectomyAm J Orthod Dentofacial Orthop 1996 110:170-77.10.1016/S0889-5406(96)70105-1 [Google Scholar] [CrossRef]
[2]. Epker BN, Modifications in the saggital split osteotomy of the mandibleJ Oral Surg 1977 35:157 [Google Scholar]
[3]. Fonseca RJ, Marciani RD, Oral and Maxillofacial Surgery: Orthognathic surgery, aesthetic surgery, cleft and craniofacial surgery. Turvey TA, editor 2009 Saunders [Google Scholar]
[4]. Harada K, Enomoto S, A new method of tongue reduction for macroglossiaJ Oral Maxillofac Surg 1995 53(1):91-92.10.1016/0278-2391(95)90513-8 [Google Scholar] [CrossRef]
[5]. Erverdi N, Usumez S, Solak A, New generation open-bite treatment with zygomatic anchorageAngle Orthod 2006 6:519-26.10.2319/101206-422.118004921 [Google Scholar] [CrossRef] [PubMed]
[6]. Tuncer C, Atac M, Tuncer B, Kaan E, Osteotomy assisted maxillary posterior impaction with miniplate anchorageAngle Orthod 2008 78:737-44.10.2319/0003-3219(2008)078[0737:OAMPIW]2.0.CO;2 [Google Scholar] [CrossRef]
[7]. Nitin VM, Ranjan A, Raghunath NM, Treatment of skeletal Class III Malocclusion with Anterior open bite using orthosurgical approach.: A case reportInt J Oral Health and Medical Res 2017 4(3):60-64. [Google Scholar]
[8]. Vadgaonkar V, Gangurde P, Deshmukh V, Shah A, Orthodontic and surgical perspectives in management of a severe skeletal open biteBMJ Case Rep 2014 :01-06.10.1136/bcr-2013-20006924835800 [Google Scholar] [CrossRef] [PubMed]
[9]. Buyukcavus MH, Orthognathic surgical treatment of patient with high angle growth pattern and skeletal open bite malocclusion: A case reportAdv Dent & Oral Health 2017 7(1):001-06.10.19080/ADOH.2017.07.555703 [Google Scholar] [CrossRef]
[10]. Park JH, Papademetriou M, Gardiner C, Grubb J, Anterior open bite correction with 2-jaw orthognathic surgeryAm J Orthod Dentofacial Orthop 2019 155(1):108-16.10.1016/j.ajodo.2017.07.02730591154 [Google Scholar] [CrossRef] [PubMed]
[11]. Trauner R, Obwegeser H, The surgical correction of mandibular prognathism and retrognathia with consideration of genioplasty. I. Surgical procedures to correct mandibular prognathism and reshaping of the chinOral Surg Oral Med Oral Pathol 1957 10:677-89.10.1016/S0030-4220(57)80063-2 [Google Scholar] [CrossRef]
[12]. Lee SG, Kang YH, Byun JH, Kim UK, Kim JR, Park BW, Stability of unilateral sagittal split ramus osteotomy for correction of facial asymmetry: long-term case series and literature reviewJ Korean Assoc Oral Maxillofac Surg 2015 41(3):156-64.10.5125/jkaoms.2015.41.3.15626131434 [Google Scholar] [CrossRef] [PubMed]
[13]. Fariña R, Mebus C, Mayer C, Torrealba R, Moreno E, Unilateral sagittal split ramus osteotomy: an alternative for some cases of asymmetric mandibularprognathismInt J Oral Maxillofac Surg 2018 47(5):630-37.10.1016/j.ijom.2017.11.01029223700 [Google Scholar] [CrossRef] [PubMed]
[14]. Brusati R, Sesenna E, Mannucci N, Gamoletti R, The midline mandibular osteotomy-ostectomy in the correction of dentofacial deformitiesInt J Adult Orthod Orthognath Surg 1987 2:37-50. [Google Scholar]
[15]. Anghinoni ML, Di Blasio A, Sesenna E, La gestione del diametro trasversale della mandibola. Implicazioni estetiche e occlusaliMondo Ortodontico 2006 4:247-62. [Google Scholar]
[16]. Joondeph DR, Bloomquist D, Mandibular midline osteotomy for constrictionAm J Orthod Dentofacial Orthop 2004 126(3):268-70.10.1016/j.ajodo.2004.06.027 [Google Scholar] [CrossRef]
[17]. Kawakami M, Yamamoto K, Noshi T, Miyawaki S, Kirita T, Effect of surgical reduction of the tongue on dentofacial structure following mandibular setbackJ Oral Maxillofac Surg 2004 62(10):1188-92.10.1016/j.joms.2004.06.03215452803 [Google Scholar] [CrossRef] [PubMed]
[18]. Miyawaki S, Oya S, Noguchi H, Takano-Yamamoto T, Long-term changes in dentoskeletal pattern in a case with Beckwith-Wiedemann syndrome following tongue reduction and ortodontic treatmentAngle Orthod 2000 70(4):326-31. [Google Scholar]