Nursing profession is generally perceived as a stressful and demanding line of work which includes physical and psychological challenges [1]. Nurses are constantly exposed to ceaseless work schedules, frequent shift duties, increased workload and work pressure. A study among ICU nurses has reported the prevalence of high and moderate level of stress among nurses to be 83.9% and 10.7% [2]. Bhatia N et al., concluded that the prevalence of occupational stress among Indian nurses stated were as high as 87.4% [3]. The risk of developing stress related symptoms like fatigue, sleep impairment, drug abuse and psychotic morbidity was found to be more among women nurses [4]. Although stress has a psychological origin, it affects several physiological processes in the human body especially by altering the autonomic nervous system via Hypothalamo Pituitary Adrenal (HPA) axis and endocrine regulations, thereby altering the cognitive functions [5]. One of the consequences of prolonged psychosocial stress is alteration in autonomic function, evidenced by increased sympathetic and decreased parasympathetic tone and increased cortisol levels [6,7]. Disturbed feedback balance on HPA axis, might be the reason for increased secretion of cortisol [8]. Chronic stress reduces cognition and attenuate mental concentration and attentiveness as evidenced by prolongation of VRT and ART [9-12]. Also both acute and chronic exposure of stress increase anxiety and aggressive behaviour [13].
Stress could be effectively managed by various interventions like meditation, yoga, deep breathing, prayer, time management, planning and decision making, listening to music and chanting hymns. Chanting has been believed to have therapeutic effect [14]. It brings enormous positive effects on our body and mind. Chanting is a simple and inexpensive method of stress reduction without side-effects and promotes relaxation [15]. It has contributed to an increase in self-awareness and consciousness, well-being and health. Introducing Mahamantra chanting to promote healthy behaviour may enhance coping mechanisms to counter the ill effects of stress. Mantra: ‘Man’ means ‘mind’ and ‘tra’ means ‘deliver’ [16, 17]. Chanting “Hare Krishna” mahamantra, a mantra emphasised in the literature from ancient India relieves stress, depression and other mental health disturbances [18]. It also calms our emotions and has enormous positive effects on our body and mind. “Hare Rama Hare Rama, Rama Rama Hare Hare; Hare Krishna Hare Krishna, Krishna Krishna Hare Hare” is the mahamantra chosen for chanting in this study. Very few studies have been dedicated to investigate the beneficial effects of Mahamantra chanting in reducing stress [18]. Hence, this exploratory study was designed to assess the effect of Mahamantra chanting on autonomic, cognitive and hormonal parameters by analysing short term Heart Rate Variability (HRV), ART, VRT and stress marker like serum cortisol levels among moderate to severe stress nursing professionals.
Materials and Methods
Participants
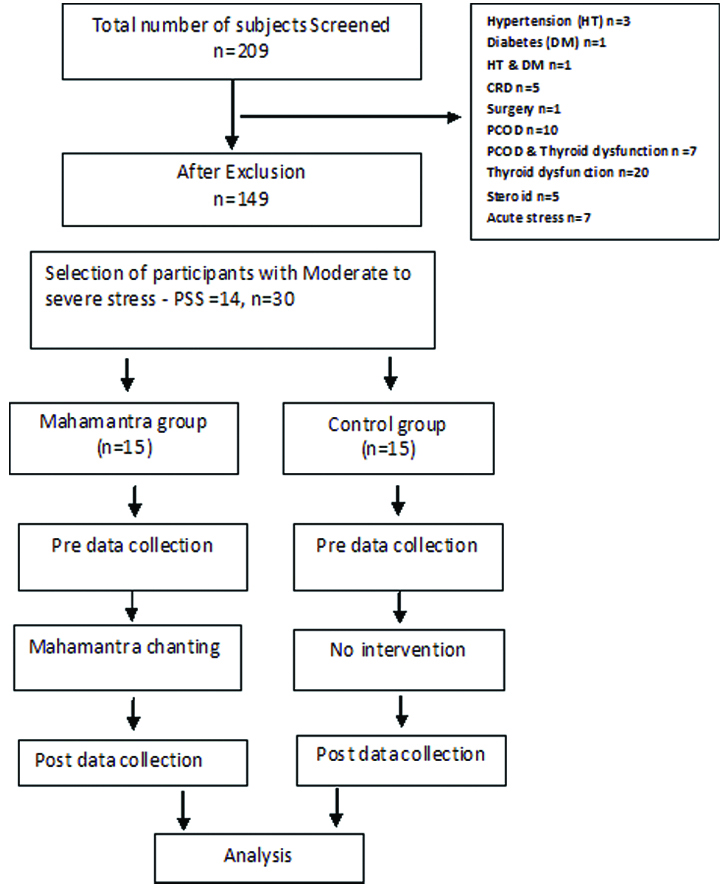
This study had an experimental design with randomisation of 30 participants into Mahamantra chanting (n=15) and control group (n=15). After selecting 30 volunteers we requested them to take chits numbered from 1-30; subjects with odd numbers were kept in intervention group and the subjects with even numbers were in control group. The sample size for this study was calculated based on the anticipatory mean difference of 0.75 with standard deviation 1.5, alpha of 0.05 and power of 0.9, which makes up 13 subjects in each group. Data was collected from women nursing professionals of various departments of a tertiary care hospital at Chennai, India between March to August in the year 2017. Ethical clearance was obtained from Sri Ramachandra Institute of Higher Education and Research at Chennai (ethical clearance registration No: CSP/17/MAR/55/79) and written informed consent was obtained from the study participants after explaining the protocol of the study.
A total of 209 female nurses between the age group 25-45 years (Mean Age-30.01±4.31 years) were screened. After procuring anthropometric details and health status of the individuals, subjects with hypertension, diabetes mellitus, thyroid dysfunction, Polycystic Ovarian Disease (PCOD), cardiorespiratory disorders, subjects who were under steroid therapy, oral contraceptive pills, psychoactive medications or any medications that may affect the HPA axis function, pregnant, nursing mother, postmenopausal women [19] and those who have experienced any major stressful event in the past six months were excluded from this study.
Allocation and Grouping
After screening, 149 subjects were selected [Table/Fig-1] for the assessment of stress using 10 item Perceived Stress Scale (PSS) [20], which showed that nearly 50%(n=75) of the female nurses were having moderate stress levels (PSS≥14) and 3%(n=4) were having severe stress (PSS>26) and the rest had low stress levels (PSS≤13). The subjects those who had PSS score ≥14 (moderate and severe stress level nurses) and who volunteered for further investigations were included for the study (n=30) and were allocated into the Mahamantra intervention group (n=15) and control group (n=15).
Screening, recruitment and grouping of study participants.
Volunteers in the mahamantra intervention group were instructed to chant mahamantra for 20 minutes during the convenient time of the day for a minimum period of 45 days. Mahamantra chanting audio was provided to them in their mobile phones both to hear and to learn chanting. Intervention was started on the proliferative phase of the menstrual cycle of the subjects (5th-7th day of menstruation) after taking pre-intervention sample and post-intervention samples were collected after 2 menstrual cycles. Subjects were requested to chant for 2 menstrual cycles. The idea was that the subject should chant for 20 minutes per day for minimum of 45 days [21]. Each of the Mahamantra intervention group participants were followed-up by our research team members in person after 3 days of chanting and on the 7th or the 8th day, later after second, fourth, eighth week consecutively to ensure that they adhere to the guidelines of the intervention. We also formed a social media web group comprising of Mahamantra intervention nurses to check if the chanters were having any difficulties in following the procedures and were also motivated. A log book was maintained to note the timing and duration of chanting per day to ensure that the entire Mahamantra chanting group were chanting consistently. All the key parameters like HRV, ART, VRT and serum cortisol levels were assessed before and after intervention in both the groups and during the proliferative phase (5th-7th day of menstruation) of the subjects to ensure that there is not much hormonal influence on the stress markers.
Physiological Parameters Measured
For shortterm HRV analysis, 5 minutes electrocardiogram (ECG) recording in sitting posture was recorded in lead II, using a simple analog amplifier. For the recording of short term HRV, the recommendation of the task force on HRV was followed [22]. RR interval data from the ECG recording were imported into Kubios software for HRV analysis. ART and VRT were recorded using PC 1000 Hertz reaction timer with audacity software [23]. The examiner was given visual/auditory stimulus by pressing the START button in first component of the reaction timer which was out of the view of the subject. Subject was instructed to press the STOP button in second component of the reaction timer as soon as he/she sees the red light / sound in the instrument. Reaction time was estimated in audacity software in msec. Minimum of five recordings were done for VRT and ART and lowest value was taken for the final analysis. Early morning (8 am-10 am) 12 hours fasting blood sample of about 2 mL was collected from the study participants in a plain red vacutainer and the serum was separated after 30 minutes by centrifugation at the rate of 3000 rpm for 10 minutes. The serum was stored in -80°C for further investigation. Later Cortisol was assessed using Enzyme Linked Immuno Sorbent Assay (ELISA).
Statistical Analysis
Categorical data were represented as frequency and percentage; Continuous data were represented as Mean, Median (standard deviation/Standard Error of Mean (SEM) and range). Parametric (Paired and unpaired t-test) and non parametric (Mann-Whitney and wilcoxon sign test) was used to compare the mean intra-group and inter-group difference. The level of significance was taken at 5% level. For the parameters in which normality was maintained, parametric tests were used and the parameters where normality was not maintained, non parametric tests were used. SPSS licensed Statistical software version 20 was used for the analysis.
Results
The present study included 30 nurses who had PSS score ≥14. They were grouped into the Mahamantra group (n=15) and control group (n=15). Demographic characteristics were similar between the two groups [Table/Fig-2].
Demographic characteristics of the study participants of Mahamantra group and control group.
| Study variables | Control group (n=15) | Mahamantra group (n=15) | p-value |
|---|
| Age (years) | 27.80±2.210 | 29.20±4.601 | 0.34$ |
| BMI (kg/m2) | 23.64±4.217 | 22.08±3.662 | 0.87$ |
| PSS score | 21.00±2.204 | 21.47±3.204 | 0.56$ |
| Years of work experience | 5.67±4.48 | 6.73±4.480 | 0.85$ |
| Marital status (Married/Unmarried) | 8 (53%)/7(47%) | 7 (47%)/8 (53%) | 0.43# |
| Residential status (Hostel/Day Scholar) | 6 (40%)/9 (60%) | 8 (53%)/7 (47%) | 0.67# |
$Unpaired t-test; #Chi-square test
Short Term Heart Rate Variability
The time domain short term HRV parameters in baseline [Table/Fig-3] showed similar values (Mean R-R-735(730.9) vs. 733.6 (694.1), resp., p=0.45, SDNN- 52 (32.81) vs. 62.6 (37.43), resp., p=0.08, pNN50- 18.4 (13.10) vs. 11.93 (8), resp., p=0.09) in between the groups. Frequency domain parameters also showed similar values in baseline (LF n.u-45.33 (46.42) vs. 49.33 (51.93), resp., p=0.48, HF n.u-53.4 (45.61) vs. 50.6 (48.03), resp., p=0.92 and LF/HF ratio-1.13(0.86) vs. 1.2 (1.08), resp., p=0.76).
Short Term HRV parameters before and after mahamantra intervention.
| HRV variables | Mahamantra groupMean (Median) (Interquartile Q1-Q3) | p-value/difference | Control groupMean (Median) (Interquartile Q1-Q3) | p-value/difference |
|---|
| Before intervention Day 1 | After intervention Day 45 | Day 1 | Day 45 |
|---|
| Mean RR (ms) | 735 (730.9) (660.6-771.1) | 769 (747.5) (713.4-819.6) | 0.73/34 | 733.6 (694.1) (670.5-772.1) | 713.4(682) (661.4-765.5) | 0.4/-20.2 |
| SDNN (ms) | 52 (32.81) (22.75-81.16) | 64.5 (59.98)$ (49.11-79.76) | 0.38/12.5 | 62.6 (37.43) (31.50-93.69) | 47.93(36.85) (33.26-62.69) | 0.28/-14.67 |
| PNN50 (ms) | 18.4 (13.10) (9.26-27.68) | 18 (12.99) (10.26-25.71) | 0.95/-0.4 | 11.93 (8) (4.55-9.28) | 9.8(8.90) (4.17-15.34) | 0.51/-2.13 |
| LF n.u | 45.33 (46.42) (37.78-53.11) | 38.47 (39.89)$ (31.97-45.09) | 0.66/-6.86 | 49.33 (51.93) (38.43-60.39) | 53.067(51.33) (42.67-3.36) | 0.58/3.73 |
| HF n.u | 53.4 (45.61) (45.61-60.94) | 60.33 (59.10)# (53.94-66.83) | 0.091/6.93 | 50.6 (48.03) 39.51-61.45) | 46.8 (48.15) (36.48-57.11) | 0.58/-3.8 |
| LF/HF Ratio | 1.13(0.86) (0.69-1.2) | 0.73 (0.67)$ (0.50-0.89) | 0.028#/-0.4 | 1.2 (1.08) (0.76-1.9) | 1.933 (1.06) (0.64-2.97) | 0.21/0.7 |
#Mann Whitney U test and $Wilcoxon test; Mean RR: Mean RR interval (msecs); SDNN: Standard deviation of all normal RR intervals (msecs); pNN50: The proportion derived by dividing NN50 by the total number of NN intervals (msecs); LF: Low frequency; HF: High frequency; LF/HF ratio, nu-normalised units
After mahamantra intervention, the nurses in the mahamantra group showed a significant increase in SDNN (64.5 (59.98) vs. 47.93 (36.85), resp., p=0.04), and HF (60.33 (59.10) vs. 46.8 (48.15), resp., p=0.05) and significant reduction in LF (38.47 (39.89) vs. 53.067 (51.33), resp., p=0.03) and LF/HF ratio (0.73 (0.67) vs. 1.933 (1.06), resp., p=0.03). The intra-group comparison after intervention also showed significant (p=0.028) decrease of LF/HF ratio {1.13 (0.86) vs. 0.73 (0.67)} among the mahamantra group nurses. Though other parameters showed variation after mahamantra chanting these were not statistically significant (p>0.05).
Cognitive Function (ART and VRT)
The baseline VRT and ART between Mahamantra and control group participants were in normal range. After the study period control group ART remained unchanged, while the ART (p=0.01) and VRT (p=0.001) significantly reduced in mahamantra group participants [Table/Fig-4].
Effects of Mahamantra on Visual and Auditory Reaction time.
| RT variables | Mahamantra group | p-value | Control group | p-value |
|---|
| Before intervention Day 1 | After intervention Day 45 | Day 1 | Day 45 |
|---|
| ART | 200±16.725 | 160±8.72* | 0.01 | 153.6±6.16 | 154.46±13.74 | 0.949 |
| VRT | 262.13±13.17 | 214.8±9.88** | 0.001 | 240.67±16.38 | 201.67±8.21 | 0.027 |
*Intergroup comparison between mahamantra and control group after intervention (unpaired t test). *p<0.05, **p<0.01, ART: Auditory Reaction Time (msecs); VRT: Visual Reaction Time (msecs).
Stress Biomarker (Serum Cortisol)
Prior to intervention the serum cortisol levels showed no significant difference between mahamantra and control group [Table/Fig-5]. After intervention participants in the mahamantra intervention group had significant (268.33±33.15 vs. 180.6±7.60 p=0.01) reduction in serum cortisol level. Inter-group comparison after intervention showed cortisol levels in the participants of mahamantra intervention group were significantly lower when compared with the levels observed in the participants of control group (180.6±7.60 vs. 255.93±26.31, p=0.001).
Effects of Mahamantra on Serum Cortisol Levels.
| Variables | Mahamantra group | p-value | Control group | p-value |
|---|
| Before intervention Day 1 | After intervention Day 45 | Day 1 | Day 45 |
|---|
| Cortisol (nmol/L) | 268.33±33.15 | 180.6±7.60* | 0.012 | 239.86±20.02 | 255.93±26.31 | 0.215 |
*p<0.05 - Intergroup comparison between mahamantra and control group after intervention (Unpaired t-test)
Discussion
This exploratory mahamantra chanting intervention study among nursing professionals has highlighted the beneficial effects of mahamantra chanting as evidenced by assessment of autonomic and cognitive functions. It examined the effect of Mahamantra chanting on autonomic, cognitive and endocrine functions among the working women nursing professionals with moderate to severe stress level (PSS≥14). Chanting Mahamantra which is considered as one form of bakthi yoga has substantiated an increase in parasympathetic tone, demonstrated a marked improvement in sympathovagal balance (LF/HF ratio), potentiated the psychomotor speed, thereby increasing the receptiveness and cognition as evidenced by shortening of Auditory and visual reaction time and reduced the stress hormone levels (cortisol) among the nursing professionals.
HRV has been recognised as a tool to evaluate the cardiac parasympathetic activity and therefore, an indicator of a relaxation response and a sensitive indicator of autonomic dysfunction in alcoholics, diabetic or cardiopathic patients [24,25]. Previous studies, supported by a recent meta-analysis, revealed that increase in LF and decrease in HF power in psychosomatic disorders, can lead to alteration in the ANS [26]. In short term HRV, the time domain measures like the mean R-R interval, NN50 and pNN50 are recognised to be strongly dependent on the vagal modulation [22]. The sympathovagal balance is assessed by LF/HF ratio. Increased LF/HF ratio reflects increased sympathetic activity and decreased LF/HF ratio indicates decreased sympathetic activity. In this study, LF and HF power expressed in normalised unit has been applied in an attempt to quantify modulation of the parasympathetic and sympathetic branches of the ANS [8]. We have found that after mahamantra chanting, significant reduction of LF/HF ratio occurs among the mahamantra group nurses. Lower LF/HF ratio indicates that the cardiac ANS has better autonomic tone and autonomic modulation. Study done by Nagarajan et al., found that carnatic music intervention in Buphali raga had significant improvement in the HRV [27]. Our results are in line with Berad A et al., who explained parasympathetic dominance after ‘OM’ chanting meditation [28]. The results of this study showed reversal in the autonomic functions in moderately/severely stressed nurses with intervention. This indicates that these nursing professionals with moderate to severe stress are prone for autonomic dysfunction at a later date and are also at an increased risk of developing lifestyle disorders such as diabetes, obesity, sleep disturbances and other cardiovascular and neurological disorders. They can reduce their risk with the mahamantra intervention. The findings of this study supports the hypothesis that disturbances of the autonomic nervous system and a reduction in the vagal control of the heart rate in particular, can play an important role in the mechanisms linking work stress and cardiovascular disorders and are reversible if addressed early with simple, suitable and sustainable interventions.
Reaction Time (RT) testing is used in the field of neurophysiology and psychology as a simple and sensitive cognitive assessment which mainly assess the psychomotor speed. It is the time period taken for the appearance of rapid voluntary reaction by an individual following a stimulus either auditory or visual. ART and VRT significantly shortened after mahamantra chanting among the nurses. Many known factors influence reaction time, arousal or states of attention, age, mental and physical fatigue. Prolonged ART and VRT during chronic stress can be because of enhanced release of epinephrine and glucocorticoid [29]. Under stressful conditions, the cognitive system is overloaded, thereby it reduces a person’s attentional resources, reduces the decision making capability, concentration and the psychomotor speed [30, 31]. Profession like nursing should be very vigilant and nimble, especially while handling emergencies during patient care. Shortening of VRT and ART after mahamantra intervention signifies better awakening, enhanced attention and faster responsiveness among the nurses. It may enhance the sensory-motor transmission velocity and faster information processing in the central nervous system. There is an improvement of ART and VRT with background music due to facilitation of processing of stimuli in somatosensory cortex. Studies done by Amin A et al., are consistent with our study showing the effectiveness of ‘OM’ chanting in mind relaxation and it has also enhanced the cognition [32].
Serum cortisol levels were higher among the nursing professionals in both the groups at the starting of the study. After mahamantra intervention, there was a significant reduction in the cortisol levels among the participants who underwent the mahamantra intervention. Elevated serum cortisol levels significantly correlate with the symptoms of metabolic syndrome [33]. There is a significant positive relationship between blood glucose, HbA1c and serum Cortisol levels [7]. Our study is in line with another study that provided music intervention and found promising outcomes after music therapy in reducing metabolic syndrome [15]. Listening to music improves the parasympathetic tone and to a lesser extent has a positive impact on endocrine and psychological stress response. These findings also help us with better understanding of the beneficial effects of music and other similar interventions like mantra chanting on the human body.
Limitation
Sample size of the study was small as it was an exploratory study, future studies with large number of participants can help in reinforcing the evidence regarding the effectiveness of the intervention. In this study, the mahamantra chanting intervention was given for a minimum period of 45 days, research on beneficial effects of chanting for longer period of time is required. Further chanting in groups under direct supervision will provide better outcomes. Autonomic functions can be further assessed by measuring catecholamine levels which can explain the mechanistic pathway for the beneficial effects observed with mahamantra chanting.
Conclusion
This exploratory study demonstrates that simple techniques like chanting has beneficial effect in relieving stress of an individual evidenced by increased parasympathetic tone, cognitive function and lowered stress hormone (serum cortisol) level among moderate to severe stressed nursing professional women.
$Unpaired t-test; #Chi-square test