Hereditary Gingival Fibromatosis: Report of Family Pedigree of Three Generations
Jaideep Mahendra1, Vijayalakshmi Rajaram2, Sujeetha Muthukumar3, Sathish Rajendran4
1 Professor, Department of Periodontics, Meenakshi Ammal Dental College, Chennai, Tamil Nadu, India.
2 Reader, Department of Periodontics, Meenakshi Ammal Dental College, Chennai, Tamil Nadu, India.
3 Postgraduate Student, Department of Periodontics, Meenakshi Ammal Dental College, Chennai, Tamil Nadu, India.
4 Senior Lecturer, Department of Periodontics, Meenakshi Ammal Dental College, Chennai, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jaideep Mahendra, Faculty of Dentistry, Meenakshi Academy of Higher Education and Research, Meenakshi Ammal Dental College and Hospital, Chennai-600095, Tamil Nadu, India.
E-mail: jaideep_m_23@yahoo.co.in
Gingival enlargement or gingival overgrowth can be defined as increase in the size of gingiva, caused due to a variety of etiological factors. One of the causes of gingival enlargement is hereditary gingival fibromatosis, which is a genetic disorder characterised by progressive enlargement of the free and attached gingiva. It may have a nodular enlargement, having stippled surfaces with no inflammation or may show inflamed surface. Clinically, gingiva may present dense or firm surface on palpation. It is commonly associated with mutation of Son of Sevenless-1 (SOS-1) gene, which is responsible for this disease. This case report focuses on a family, diagnosed with hereditary gingival fibromatosis in three consecutive generations. This report also discusses the diagnosis, treatment, histopathological features and the pattern of inheritance associated, which is emphasised through pedigree analysis.
Electrocoagulation, Gingival overgrowth, Gingivectomy, Pedigree
Case Report
Case-1
A 22-year-old male presented with the chief complaint of swelling of the gums in the right upper and lower front and back tooth region for the past six months. Patient’s medical history was non-contributory and the patient was not on medication. On interviewing the patient about family history, he revealed that the patient’s sister and mother had a similar history of gingival enlargement. Patient’s sister underwent gingivectomy two years ago.
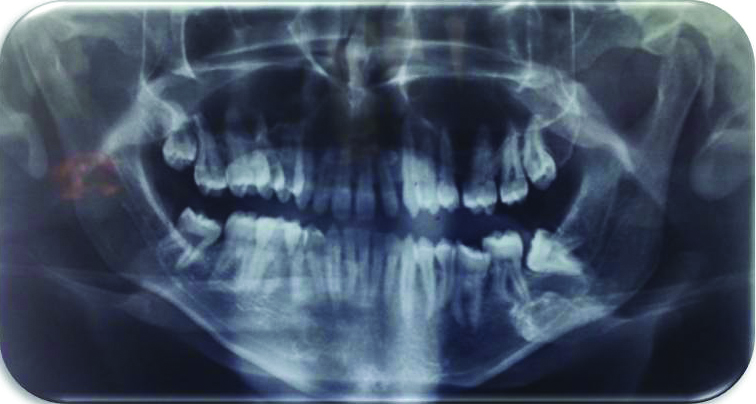
Intraoral examination revealed generalised severe gingival enlargement on the buccal and lingual/palatal aspect of first and fourth quadrant. The gingival surface was pink in colour. The enlargement extended to the incisal edge of teeth in the first quadrant [Table/Fig-1]. On palpation, the gingival overgrowth was firm, dense, fibrous and painless. Generalised pseudopockets were observed along with bleeding on probing. Panaromic radiograph showed normal bone height and impacted right upper and left lower third molars [Table/Fig-2]. On the basis of the clinical presentation and family history, a provisional diagnosis of hereditary gingival fibromatosis was made. Routine blood investigations were done, which showed values within normal range.
Pre-operative image of the patient (son) showing gingival enlargement. a) Right lateral view, b) occlusal view, c) Lingual view, d) Buccal view.

Orthopantomograph showing no bone loss in relation to all the quadrants.
Considering the severity of the enlargement, functional and aesthetic requirements, treatment was discussed with the patient and informed consent was obtained. Under local anaesthesia, biologic width calculation was done by the transgingival probing method. Once the amount of gingival tissue to be excised was demarcated, gingivectomy was performed by giving an external bevel incision using a no.15 scalpel blade and the gingival tissue was excised in both the quadrants [Table/Fig-3]. Gingivoplasty was done using electrocautery. Using a loop electrode, planing motion was given and the region was irrigated with saline frequently to dissipate the heat generated by the electrode. Postoperatively, the patient was prescribed Antibiotics (Amoxicillin, 500 mg 8 hourly for 5 days) and analgesics (Aceclofenac+Paracetamol, 12 hourly for 3 days). Use of 0.12% chlorhexidine rinse was also advised. The patient was instructed to apply ice-pack and avoid any mechanical trauma to the surgical site. There were no post-operative complications and the patient tolerated the procedure well [Table/Fig-4]. After recovery, the instructions given to maintain the oral hygiene were reinforced and complete tissue healing was evident after three weeks.
Intra-operative view after the gingivectomy procedure. a) Buccal view of right upper quadrant b) occlusal view c) lower buccal view d) lingual view e) lower labial view.

Post-operative picture-six months after gingivectomy. a) buccal view b) occlusal view c) lower labial view d) lower buccal view e) lingual view.

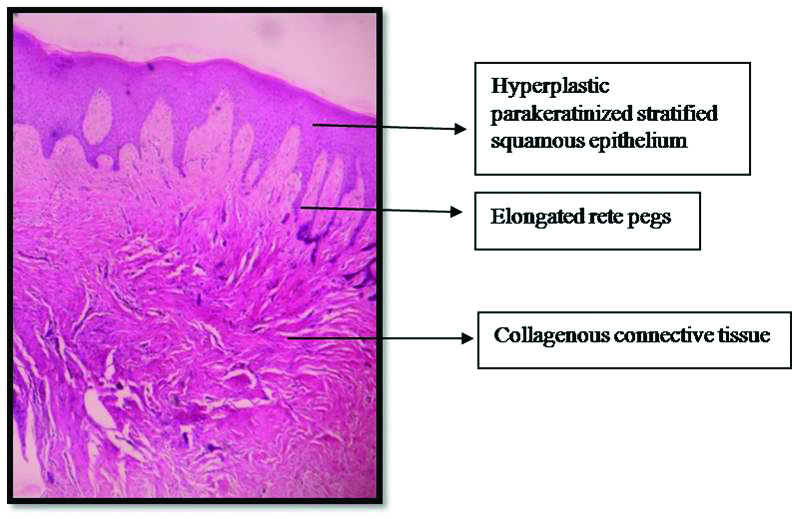
Excisional biopsy sample of the excised gingival tissue was sent for histologic evaluation. The fixed tissue specimens showed hyperplastic parakeratinized stratified squamous epithelium with elongated rete ridges. The underlying connective tissue presented fibrous hyperplasia with varying degree of cellularity [Table/Fig-5]. Chronic inflammatory cell infiltrate with a predominance of lymphocytes and plasma cells were also evident.
Histopathologic picture of the excised gingival tissue.
Hematoxylin and Eosin staining; 10X
Case-2
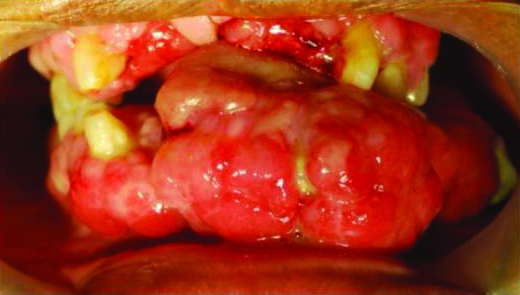
Patients’ mother also showed similar enlargement three years back. The mother while examination, revealed presence of similar enlargement seen in her family including her siblings, father and children. However the children never reported to the dental clinic at that time. Her clinical records revealed the presence of erythematous, firm and fibrotic gingiva with a pebble like appearance. It extended throughout the upper and lower arch [Table/Fig-6]. The position of the gingiva was above the CEJ and the teeth were submerged. Purulent yellow discharge was present in relation to lower anteriors. There were only 16 teeth and most of them grade III mobile. Based on patient’s history and clinical features, full mouth extraction along with excision of the hypertrophic lesion under general anaesthesia was planned [Table/Fig-7,8,9,10,11,12 and 13]. Full mouth rehabilitation was done by providing removable complete dentures [Table/Fig-14].
Pre-operative intraoral photograph of patient’s mother showing generalised gingival enlargement.
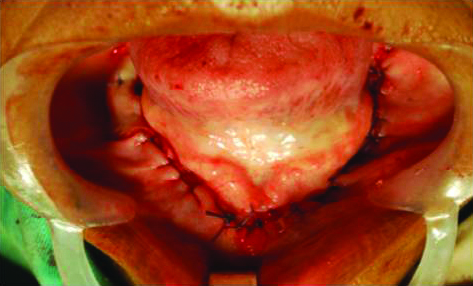
Excision of the gingival mass in maxillary arch (Case-2).
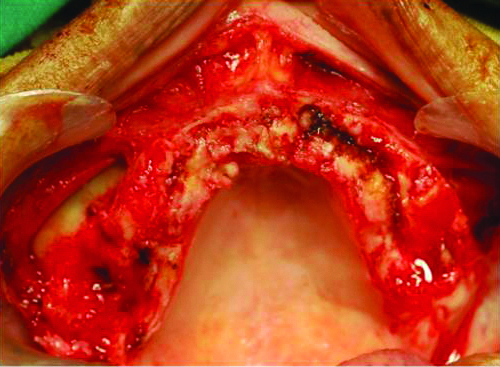
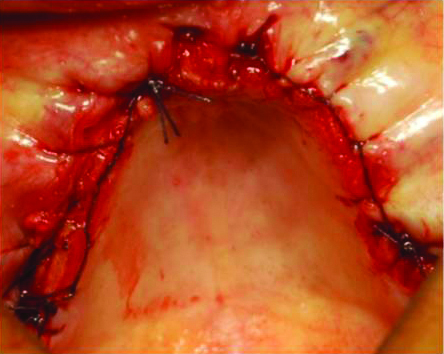
Flap sutured in maxillary arch (Case-2).
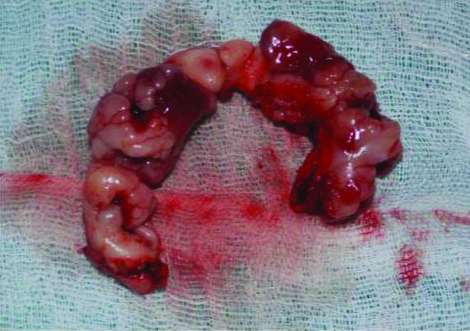
Excised gingival tissue from the maxillary arch (Case-2).
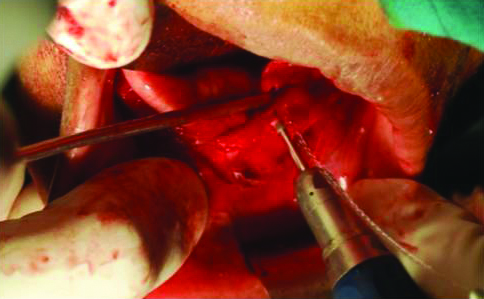
Alveoloplasty done in relation to mandibular arch (Case-2).
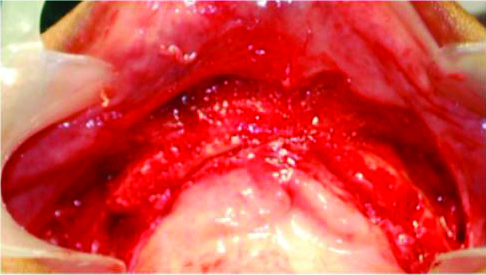
Post-operative view: after alveoloplasty in the mandibular arch (Case-2).
Excised gingival tissue from mandibular arch (Case-2).

Flap sututred in the mandibular arch (Case-2).
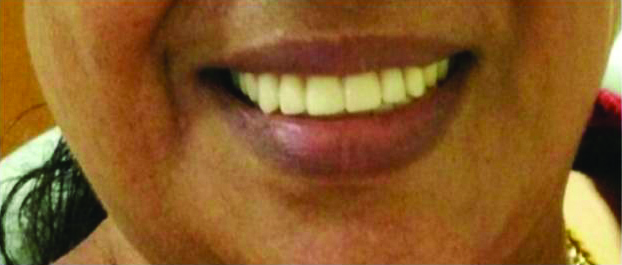
Full mouth rehabilitation with complete dentures (Case-2).
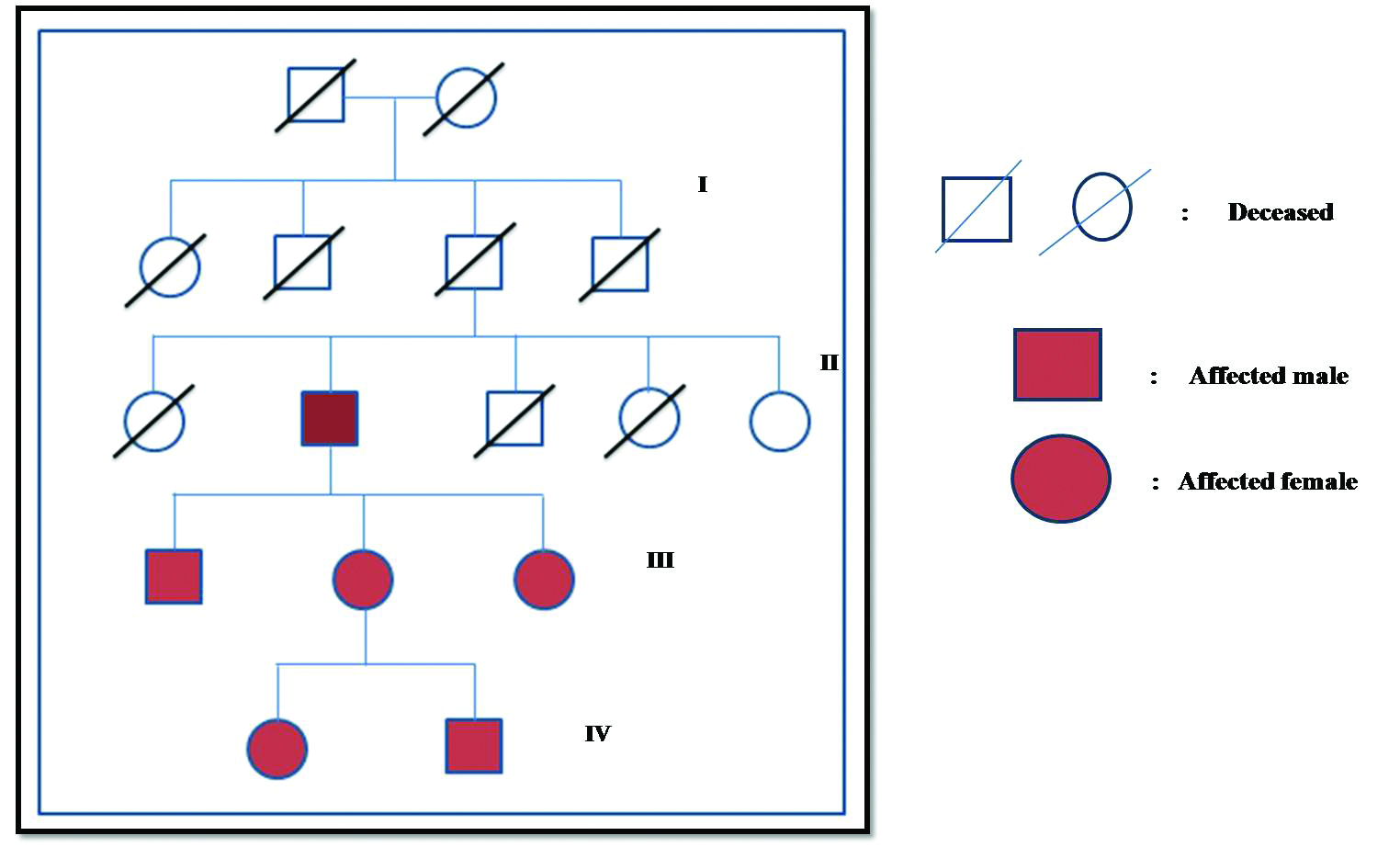
In both the cases of son and mother, on combining the clinical, histological findings and family history, a final diagnosis of hereditary gingival fibromatosis was made [Table/Fig-15].
PEDIGREE CHART representing three affected generations.
Discussion
Gingival fibromatosis is a slowly progressive gingival enlargement caused by collagenous overgrowth of the fibrous component of the gingival connective tissue. Hereditary Gingival Fibromatosis (HGF) is a rare, benign, non-haemorrhagic fibrous enlargement of gingival tissue. Differential diagnosis of such gingival enlargements includes enlargement associated with drugs, hormonal changes and genetic disorders. Inflammations, tumours and cysts can also present themselves as gingival enlargements [1]. It was first reported by Goddard and Gross in 1856 [2]. A mutation in the Son of Sevenless-1 (SOS-1) gene has been suggested as a possible cause of isolated gingival fibromatosis. Hart TC et al indicated that alteration of the carboxyl-terminal domain of the SOS-1 protein is responsible for HGF-1. They described the genomic structure of the SOS-1 gene and presented evidence that insertion of acytosine between nucleotides 126,142 and 126,143 in codon 1083 of the SOS-1 gene is responsible for HGF-1 [3]. This insertion mutation, which segregates in a dominant manner over four generations, introduces a frame shift and creates a premature stop codon, abolishing four functionally important proline-rich SH-3 binding domains, normally present in the carboxyl-terminal region of the SOS-1 protein. The resultant protein chimera has the wild-type SOS-1 protein for the N-terminal amino acids, 1-1083 fused to a novel 22-amino acid carboxyl terminus. Xiao S et al., identified a new locus (GINGF2) located on chromosome 5q13-q22 [4]. Chromosomal anomalies seen in syndromic forms include duplications, deletions, or other anomalies of chromosomes 2p13-16, 4q (MIM 252500), 8 (MIM 266270), 14q, 19p (MIM 246200), 19q (MIM 248500) and Xq. de Andrade CR et al., has stated that TGF-β 1 has an autocrine role as a stimulator of HGF fibroblast proliferation [5]. This case report deals with the hereditary gingival fibromatosis of three consecutive generations of a family. The report also describes the diagnosis, clinical and microscopic features along with the treatment of hereditary gingival fibromatosis, highlighting the importance of genetic condition by pedigree analysis.
This case report represents three generations of a family with HGF to characterise the pattern of inheritance. The pedigree was constructed including the five latest generations of the family [Table/Fig-15]. The clinical examination and history of this family revealed that six members presented a generalised gingival overgrowth. On histopathological examination, the biopsy showed well-structured epithelium with elongated papillae pushing into deep fibrous connective tissue. These findings were similar to those observed previously in other families [6].
Pego SP et al., has reported the ultrastructural feature of HGF. The gingival tissue showed collagen fibrils exhibiting a typically repeating banding pattern of which some fibrils displayed loops at their end. In few regions, an alignment was also observed [7]. There is excessive accumulation of ECM proteins, including collagen type I in HGF. During collagen biosynthesis, nascent single procollagen polypeptides undergo post-translational modification. Heat shock protein 47 (HSP47) binds to the nascent type I procollagen peptides to prevent premature folding and aggregation of procollagen chains. It participates in the translocation and secretion of procollagen I into the extracellular space. In fibroblast cultures derived from patients with HGF, Type I collagen and HSP47 mRNA and protein levels are increased significantly.
The activation of Sos-1-Ras-ERK1/2 pathway up-regulates the expression of type I collagen, CTGF, TGF-β, and TIMPs, while it down-regulates the expression of MMPs. Increased activation of the ERK1/2 pathway by constitutively active SOS-1 could drive the fibrosis in HGF. We have compiled similar cases of HGF and tabulated to show a comparative analysis [Table/Fig-16].
Case reports/series of hereditary gingival fibromatosis in the past 5 years obtained from PubMed search engine [8-26].
| Authors | Cases |
|---|
| Gandhi M et al., [8] | Case report of a eight-year-old child with HGF treated by gingivectomy under GA. |
| Ghartimagar D et al., [9] | Squamous cell carcinoma arising in familial gingival fibromatosis in a 21-year-old girl. |
| Ferreira Gonçalves C et al., [10] | 20-year-old Brazilian female patient with HGF followed-up for seven years without recurrence |
| Gawron K et al., [11] | Analysis of mutations in the SOS-1 gene in two Polish families with HGF. |
| Almiñana-Pastor PJ et al., [12] | Clinical aspects and treatment in two 8-year-old boys with HGF. |
| Aboujaoude S et al., [13] | Diode laser versus scalpel in the treatment of hereditary gingival fibromatosis in a 6-year old boy. |
| Karthikeyan BV et al., [14] | Family with three generations afflicted with a non-syndromic form of HGF with distinctive clinical and histological characteristics. |
| Gawron K et al., [15] | Gingival fibromatosis with significant de novo formation of fibrotic tissue and a high rate of recurrence in an 11-year-old female. |
| Michaud PL and Patel A [16] | HGF with extreme ridge thickness and insufficient interarch distance: A clinical report of surgical and prosthetic management. |
| Dani NH et al., [17] | A case report of HGF in 18-year-old male treated by gingivectomy. |
| Tripathi AK et al., [18] | Management of hereditary gingival fibromatosis in a 18-year-old female with a positive family history, where the mother was also affected. |
| Jadhav AS and Marathe SP [19] | Recurrent idiopathic gingival fibromatosis with generalised aggressive periodontitis in a 30-year-old female. |
| Pego SP et al., [20] | Clinical and ultrastructural features of HGF in a Brazilian family. |
| Zandinejad A et al., [21] | A case report on complete oral rehabilitation of a patient with HGF. |
| Tripathi AK et al., [22] | HGF in a 14-year-old male. |
| Ma Y et al., [23] | Non-syndromic HGF in three Chinese families which is not due to SOS-1 gene mutation. |
| Inagaki K et al., [24] | Case report on the management of traumatic dental injury after periodontal surgery in patient with HGF. |
| Gita B et al., [25] | Idiopathic gingival fibromatosis associated with progressive hearing loss: A nonfamilial variant of Jones syndrome in a 14-year-old male patient |
| Shetty A et al., [26] | Idiopathic gingival enlargement associated with generalised aggressive periodontitis in a 19-year-old female. |
The usual treatment of gingival fibromatosis includes external bevel gingivectomy using a scalpel [27]. If it is complicated by bony defects, a flap surgery is carried out. Removal of the hypertrophic tissue by electrosurgery or laser reduces the risk of bleeding, pain and post-operative discomfort of the patient [28]. In this case, the use of electrocautery helped us to give a clean incision with less bleeding and provided a clear view of the surgical site. The chair time of the surgical procedure as well as the operator fatigue was reduced. There was no discomfort during the healing period.
We evaluated four generations of a south Indian family with six individuals exhibiting hereditary gingival fibromatosis. Pedigree analysis was done to analyse the pattern of inheritance throughout the family. Gingival fibromatosis is not life threatening and is tolerated well by some patients without treatment, but the quality of life is compromised among the affected individuals. Therefore, to stabilise the long term outcomes and to alleviate suffering, non-surgical therapies are important. In this case, the propositon helped us to map the pedigree chart which included three generations. The case presented here was managed successfully with surgical intervention and electrocautery. The patient was educated about the chances of recurrence of the disease and occurrence in future generations. Importance of oral hygiene maintenance and recall visits were also emphasised.
[1]. Armitage GC, Development of a classification system for periodontal diseases and conditionsAnnals of Periodontology 1999 4(1):1-6.10.1902/annals.1999.4.1.110863370 [Google Scholar] [CrossRef] [PubMed]
[2]. Ramer M, Marrone J, Stahl B, Burakoff R, Hereditary gingival fibromatosis: Identification, treatment, controlJ Am Dent Assoc 1996 127:493-95.10.14219/jada.archive.1996.02428655871 [Google Scholar] [CrossRef] [PubMed]
[3]. Hart TC, Zhang Y, Gorry MC, Hart PS, Cooper M, Marazita ML, A mutation in the SOS1 gene causes hereditary gingival fibromatosis typeAm J Hum Genet 2002 70:943-54.10.1086/33968911868160 [Google Scholar] [CrossRef] [PubMed]
[4]. Xiao S, Bu L, Zhu L, A new locus for hereditary gingival fibromatosis (GINGF2) maps to 5q13-q22Genomics 2001 74(2):180-85.10.1006/geno.2001.654211386754 [Google Scholar] [CrossRef] [PubMed]
[5]. de Andrade CR, Cotrin P, Graner E, Almeida OP, Sauk JJ, Coletta RD, Transforming Growth Factor-β1 autocrine stimulation Regulates fibroblast proliferation in hereditary gingival fibromatosisJ Periodontol 2001 72:1726-33.10.1902/jop.2001.72.12.172611811509 [Google Scholar] [CrossRef] [PubMed]
[6]. Kantarci A, Nseir Z, Kim YS, Sume SS, Trackman PC, Loss of basement membrane integrity in human gingival overgrowthJ Dent Res 2011 90:887-93.10.1177/002203451140470321483030 [Google Scholar] [CrossRef] [PubMed]
[7]. Pêgo SP, de Faria PR, Santos LA, Coletta RD, de Aquino SN, Martelli-Júnior H, Ultrastructural evaluation of gingival connective tissue in hereditary gingival fibromatosisOral Surg Oral Med Oral Pathol Oral Radiol 2016 122(1):81-88.10.1016/j.oooo.2016.04.00227260277 [Google Scholar] [CrossRef] [PubMed]
[8]. Gandhi M, Tandon S, Sharma M, Vijay A, Nonsyndromic gingival fibromatosis: a rare case reportInt J Clin Pediatr Dent 2018 11(3):250-53.10.5005/jp-journals-10005-152130131651 [Google Scholar] [CrossRef] [PubMed]
[9]. Ghartimagar D, Koirala U, Ghosh A, Shrestha MK, Thapa S, Narasimhan R, Squamous cell carcinoma arising in familial gingival fibromatosis-a rare case reportJ Surg Case Rep 2017 9(10):rjx19710.1093/jscr/rjx197 [Google Scholar] [CrossRef]
[10]. Ferreira Gonçalves C, Mundim AP, Martins RFS, Gagliardi RM, Santos PSS, Hereditary gingival fibromatosis: a case report with seven-year follow-upActaStomatol Croat 2018 52(3):254-58.10.15644/asc52/3/930510301 [Google Scholar] [CrossRef] [PubMed]
[11]. Gawron K, Bereta G, Nowakowska Z, Łazarz-Bartyzel K, Potempa J, Chomyszyn-Gajewska M, Analysis of mutations in the SOS-1 gene in two Polish families with hereditary gingival fibromatosisOral Dis 2017 23(7):983-89.10.1111/odi.1268428425619 [Google Scholar] [CrossRef] [PubMed]
[12]. Almiñana-Pastor PJ, Buitrago-Vera PJ, Alpiste-Illueca FM, Catalá-Pizarro M, Hereditary gingival fibromatosis: Characteristics and treatment approachJ ClinExp Dent 2017 9(4):e599-e602.10.4317/jced.5364428469831 [Google Scholar] [CrossRef] [PubMed]
[13]. Aboujaoude S, Cassia A, Moukarzel C, Diode laser versus scalpel in the treatment of hereditary gingival fibromatosis in a six-year old boyClin Pract 2016 6(4):89510.4081/cp.2016.89527994842 [Google Scholar] [CrossRef] [PubMed]
[14]. Karthikeyan BV, Khanna D, Prabhuji MLV, The autosomal dominant inheritance of hereditary gingival fibromatosis: a case reportN Y State Dent J 2016 82(6):43-46. [Google Scholar]
[15]. Gawron K, Łazarz-Bartyzel K, Fertala A, Plakwicz P, Potempa J, Chomyszyn-Gajewska M, Gingival fibromatosis with significant de novo formation of fibrotic tissue and a high rate of recurrenceAm J Case Rep 2016 17:655-59.10.12659/AJCR.89999727609299 [Google Scholar] [CrossRef] [PubMed]
[16]. Michaud PL, Patel A, Hereditary gingival fibromatosis with extreme ridge thickness and insufficient interarch distance: A clinical report of surgical and prosthetic managementJ Prosthet Dent 2016 116(1):15-20.10.1016/j.prosdent.2016.01.00126873770 [Google Scholar] [CrossRef] [PubMed]
[17]. Dani NH, Khanna DP, Bhatt VH, Joshi CP, Idiopathic gingival fibromatosisJ Indian SocPeriodontol 2015 19(6):698-700.10.4103/0972-124X.16220626941525 [Google Scholar] [CrossRef] [PubMed]
[18]. Tripathi AK, Dete G, Saimbi CS, Kumar V, Management of hereditary gingival fibromatosis: A 2 years follow-up case reportJ Indian Soc Periodontol 2015 19(3):342-44.10.4103/0972-124X.14864326229281 [Google Scholar] [CrossRef] [PubMed]
[19]. Jadhav AS, Marathe SP, Recurrent idiopathic gingival fibromatosis with generalized aggressive periodontitis: A rare case reportJ Indian Soc Periodontol 2015 19(1):93-95.10.4103/0972-124X.14583325810601 [Google Scholar] [CrossRef] [PubMed]
[20]. Pego SP, Coletta RD, Mendes DC, de Faria PR, Melo-Filho MR, Alves LR, Hereditary gingival fibromatosis: clinical and ultrastructural features of a new familyMed Oral Patol Oral Cir Bucal 2015 20(2):e150-55.10.4317/medoral.2017025475776 [Google Scholar] [CrossRef] [PubMed]
[21]. Zandinejad A, Atarodi M, Abdel-Azim T, Leonhart RM, Morton D, Complete oral rehabilitation of a patient with hereditary gingival fibromatosis: a clinical reportJ Prosthet Dent 2015 113(1):1-7.10.1016/j.prosdent.2014.07.01325277031 [Google Scholar] [CrossRef] [PubMed]
[22]. Tripathi AK, Upadhaya V, Kumar V, Saimbi CS, Hereditary gingival fibromatosis and its management: 2-year follow-upContemp Clin Dent 2014 5(4):569-71.10.4103/0976-237X.14283525395783 [Google Scholar] [CrossRef] [PubMed]
[23]. Ma Y, Sun Z, Hu Y, Liu Y, Jin L, Zhang F, Non-syndromic hereditary gingival fibromatosis in three Chinese families is not due to SOS1 gene mutationsCell Biochem Biophys 2014 70(3):1869-73.10.1007/s12013-014-0144-925062969 [Google Scholar] [CrossRef] [PubMed]
[24]. Inagaki K, Kamei H, Mitani A, Noguchi T, Management of traumatic dental injury after periodontal surgery in patient with hereditary gingival fibromatosis: Case reportOral Health Dent Manag 2014 13(2):260-65. [Google Scholar]
[25]. Gita B, Chandrasekaran S, Manoharan P, Dembla G, Idiopathic gingival fibromatosis associated with progressive hearing loss: A nonfamilial variant of Jones syndromeContemp Clin Dent 2014 5(2):260-63.10.4103/0976-237X.13238724963260 [Google Scholar] [CrossRef] [PubMed]
[26]. Shetty A, Gupta N, Shetty D, Kadakia R, Idiopathic gingival enlargement associated with generalized aggressive periodontitis in a 19-year-old femaleJ Indian Soc Periodontol 2014 18(2):244-48.10.4103/0972-124X.13134424872638 [Google Scholar] [CrossRef] [PubMed]
[27]. Martelli-Junior H, Bonan PR, Dos Santos LA, Santos SM, Cavalcanti MG, Coletta RD, Case reports of a new syndrome associating gingival fibromatosis and dental abnormalities in a consanguineous familyJ Periodontol 2008 79:1287-96.10.1902/jop.2008.07052018597613 [Google Scholar] [CrossRef] [PubMed]
[28]. Gontiya G, Bhatnagar S, Mohandas U, Galgali SR, Laser-assisted gingivectomy in pediatric patients: a novel alternative treatmentJ Indian SocPedoPrev Dent 2011 29:264-69.10.4103/0970-4388.8583921985887 [Google Scholar] [CrossRef] [PubMed]