CA-19-9 as an Emerging Marker of Ovarian Tumour: A Rare Entity
Alpana Singh1, Astha Srivastava2, Divya Chauhan3, Rajeshwari Gautam4, Gita Radhakrishnan5
1 Assistant Professor, Department of Obstetrics and Gynaecology, UCMS and GTB Hospital, Delhi, India.
2 Assistant Professor, Department of Obstetrics and Gynaecology, LHMC and SSK Hospital, New Delhi, India.
3 Senior Resident, Department of Obstetrics and Gynaecology, UCMS and GTB Hospital, Delhi, India.
4 Senior Resident, Department of Obstetrics and Gynaecology, UCMS and GTB Hospital, Delhi, India.
5 Director Professor, Department of Obstetrics and Gynaecology, UCMS and GTB Hospital, Delhi, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Astha Srivastava, Assistant Professor, Department of Obstetrics and Gynaecology, LHMC and SSK Hospital, New Delhi-110001, India.
E-mail: astha1402@gmail.com
Tumour markers are widely used in clinical practice for diagnosis; follow-up, prognosis and to predict recurrence of certain malignancies. Markers for ovarian cancer include CA-125 antigen, CA-15-3 antigen, and Carcino-Embryonic Antigen (CEA). CA-19-9 antigen is usually elevated in malignancies including colorectal carcinoma, pancreatic adenocarcinoma but significantly raised levels of <10,000 U/mL were seen in advanced stage of gastrointestinal malignancy. A reported case of 60-year-old female who had abnormally high levels of CA19-9 in the blood associated with mucinous carcinoma right ovary invasive endocervical type. At one month post surgery CA 19-9 dropped significantly. There are few case reports which have shown an association of raised CA19-9 with benign pathology but the present case is first case showing such high levels of CA19-9 associated with mucinous carcinoma of ovary. This highlights the fact that although CA19-9 is a marker of gastrointestinal malignancy; thorough evaluation to rule out ovarian malignancy in suspected cases should be done.
Cancer antigen 125 (CA-125), Cancer antigen 15-3 (CA 15-3), Mucinous carcinoma
Case Report
A 60-year-old P2L2 postmenopausal woman since 15 years presented with complaint of abdominal distension since 4 months. She also had complaint of constipation since 10-15 days. She was a known case of hypothyroidism and Type 2 diabetes mellitus and was on treatment for both since five years. Family history was not significant. On examination, abdominal distension, ascites and shifting dullness were present. There was an 18 cm×18 cm abdominopelvic mass which was with firm to cystic in consistency and was non tender. On per vaginum examination, same mass was felt and on per rectal examination rectal mucosa was free.
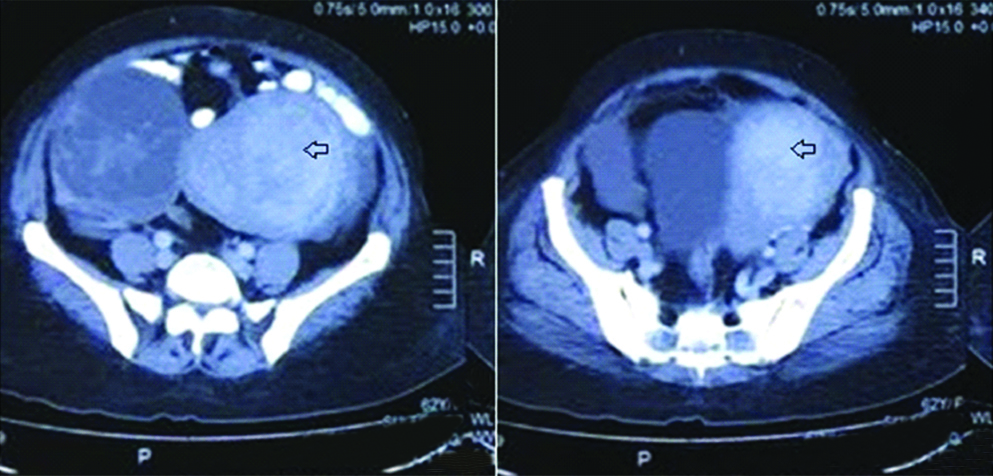
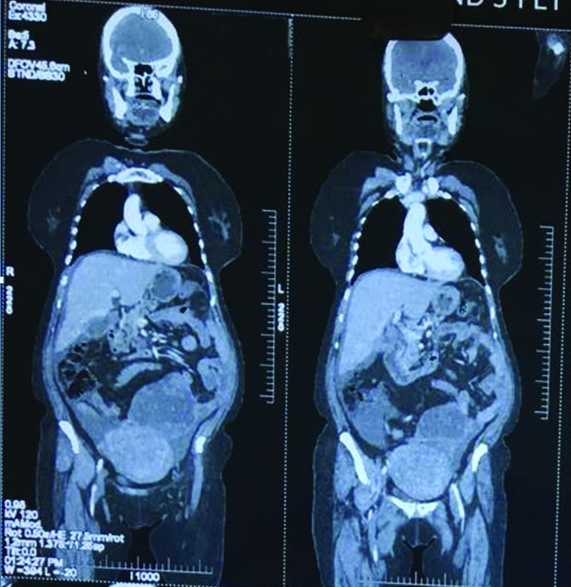
Haematological and biochemical profile of the patient was normal. Ultrasonography (USG) was done which showed evidence of large multiloculated/septated cystic mass in right adnexal region measuring 10.8 cm×15 cm having a marginal nodular shadow of 3.2 cm×4.5 cm s/o right ovarian mass/cyst possibly pseudomucinous cystadenocarcinoma. Left adnexal region was normal. Computed tomography scan of the abdomen showed a large, complex mixed density solid cystic right adnexal space occupying lesion extending from right adnexal region in pelvis [Table/Fig-1]. Lesion showed multiple thick walled enhancing septa with associated solid component in its inferior part. There was a gall bladder neck calculus with gall bladder wall oedema. There was also a large amount of ascites. The findings were suspicious for malignant epithelial tumour of the left ovary. The pancreas, spleen, both kidneys and both adrenal glands appeared normal. CA-19-9 level was increased to 21,507 U/mL (normal range, 0 to 27 U/mL), CA-125 antigen was 99.94 U/mL (normal range, 0 to 35 U/mL), CEA was 23 ng/mL (normal range, 0 to 4.7 ng/mL) and serum lipase was 34. The patient’s white blood cell count was 8,800/μL (normal range, 4,000 to 10,000/μL) and haemoglobin was 13.6 g/dL. Stool for occult blood was negative. Other laboratory tests were within normal range. In view of abnormally high levels of CA 19-9 upper GI and lower GI endoscopy were done; reports of which were normal. PET CT was done to further support the diagnosis and also to rule out any gastrointestinal tumour [Table/Fig-2]. It showed evidence of mildly metabolically active large predominantly multiseptate cystic lesion in left adnexa likely primary ovarian. It also showed presence of ascites and there was no evidence of metabolically active lesion anywhere else.
Computed tomography scan showing a large, complex mixed density solid cystic right adnexal space occupying lesion extending from right adnexal region in pelvis.
PET CT showing right ovarian mass.
Considering the clinical presentation, ultrasound and CT findings, most probable diagnosis of ovarian malignancy was kept in mind. Other differentials were GI malignancy because of raised levels of CA19-9. Patient was taken up for exploratory laparotomy. Per operatively 300 cc of straw coloured mucinous ascitic fluid was present. Around 10 cm×15 cm multicystic ovarian mass was seen [Table/Fig-3]. Capsule had a small 0.5 cm rent and mucinous fluid was seen oozing through the rent [Table/Fig-4]. Right tube was stretched over the mass. Uterus was enlarged to12-14 week size. Left tube and ovary were normal. Infra colic omentum had multiple areas of thickening and nodularity. Rest of the abdominal organs-caecum, appendix, ascending colon, liver, spleen, stomach, pancreas and descending colon was normal. Total abdominal hysterectomy with bilateral salpingo oopherectomy plus pelvic lymphadenectomy and infracolic omentectomy was done.
Intraoperative image showing multicystic ovarian mass.
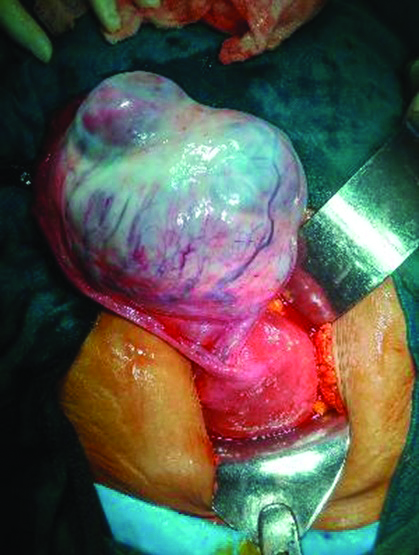
Intraoperative image showing rent through which mucinous fluid was oozing.

Postoperative period was uneventful. The final histopathlogical report came out to be mucinous carcinoma right ovary invasive endocervical type [Table/Fig-5,6]. At one month postsurgery CA 19-9 came to 66 U/mL and chemotherapy was started.
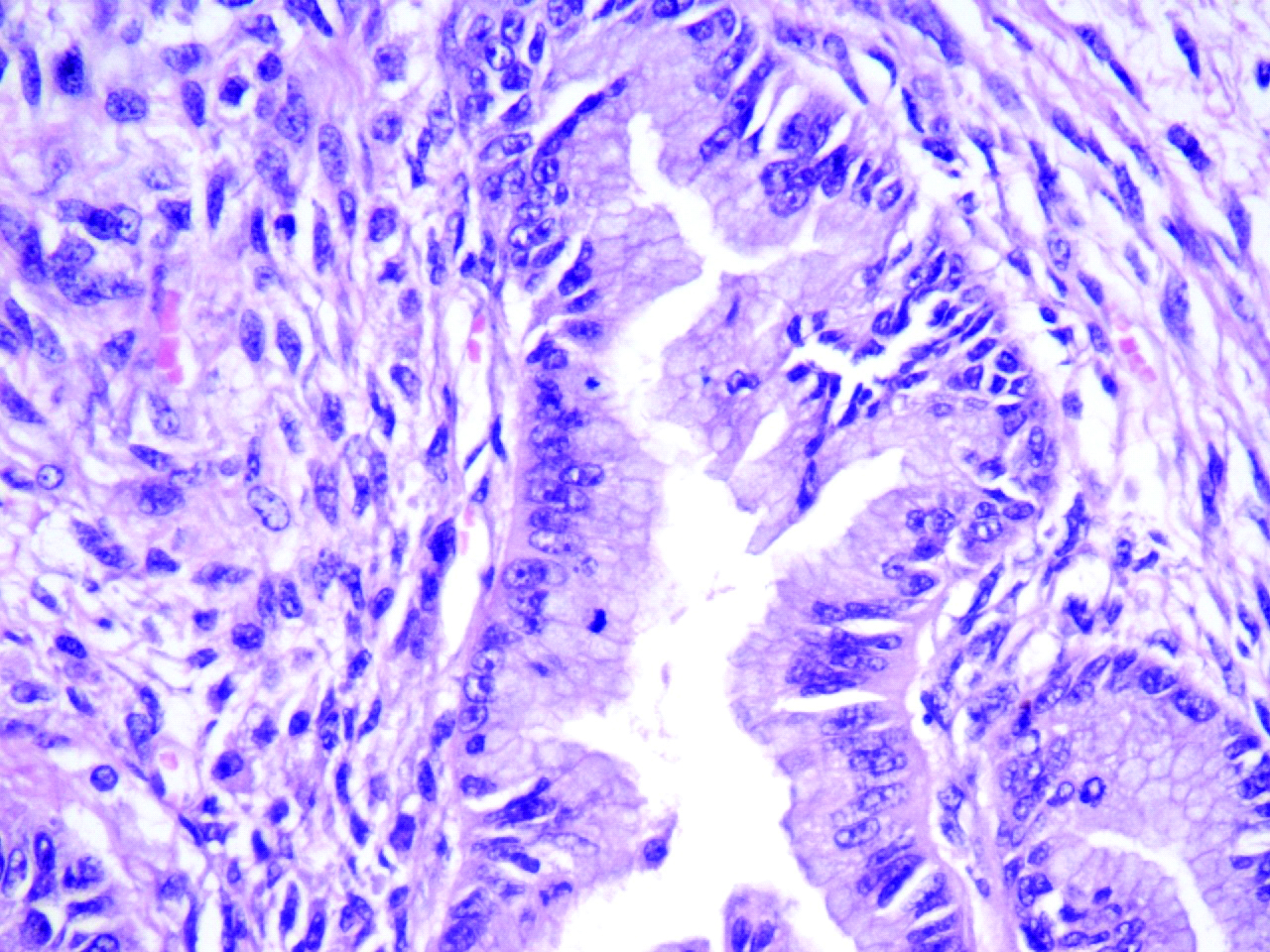
Low power view histopathological slide showing mucinous adenocarcinoma with tumour cells arranged in complex glandular pattern.
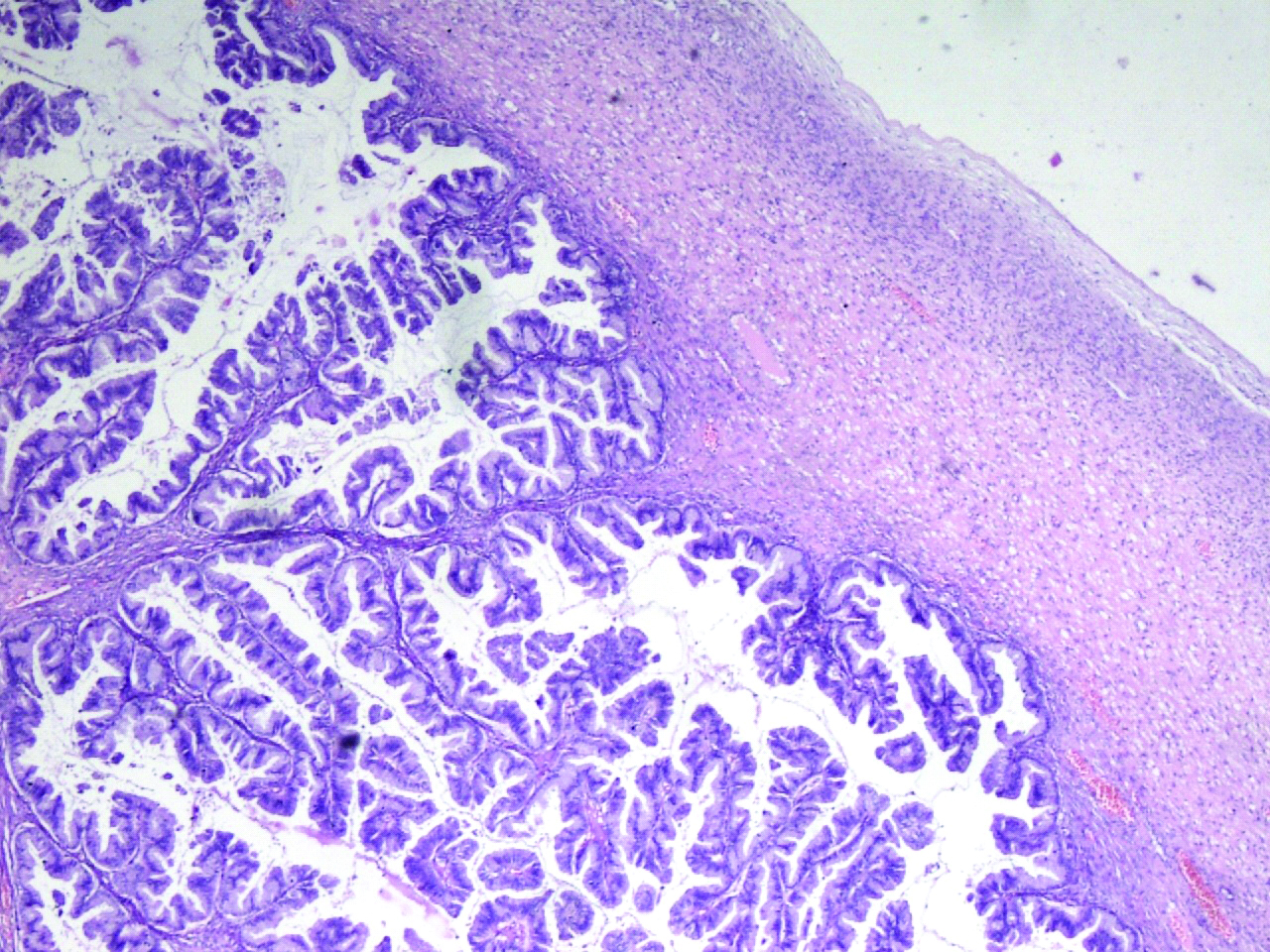
High power view histopathological slide showing intestinal type of mucinous epithelium.
Discussion
Tumour markers are widely used in clinical practice for diagnosis; follow-up, prognosis and to predict recurrence of certain malignancies. Markers for ovarian cancer include CA-125 antigen, CA-15-3 antigen, and CEA.
CA-19-9 antigen is a monosialoganglioside. It is secreted by mucinous tumours of the gastrointestinal tract [1]. It is a sialylated lewis blood group antigen which is primarily used for diagnosis, follow-up, and prognosis of pancreatic carcinoma. Its normal value is <35 U/mL. It is considered as the most sensitive and specific marker of pancreatic carcinoma. Its level is elevated in benign and malignant conditions of hepatobiliary system and pancreas [1]. Numerous studies have been published which suggest that serum CA19-9 level can be a useful marker in diagnosis of benign dermoid cyst but in those studies, significant large tumour size, bilateral tumour involvement, and tumour torsion were associated with serum CA19-9 elevation [2,3].
In a case reported by Pandey D et al., CA19-9 was found to be elevated in a postmenopausal woman with benign mucinous cystadenoma [4]. Similarly Brain O et al., and Pyeon SY et al., have reported raised level of CA19-9 in a case with ruptured ovarian mucinous cystadenoma [5,6]. There are very few case reports showing raised levels of CA19-9 in borderline mucinous tumours and malignant mucinous carcinoma [7]. The present case is an addition to the literature which shows markedly elevated CA19-9 as a diagnostic marker in ovarian mucinous carcinoma.
In study by Cho HY and Kyung MS, serum CA19-9 was found to be elevated in primary ovarian mucinous tumours [8]. In their study it was seen that only borderline and malignant mucinous tumours were considerably related with serum CA 19-9 elevation but benign mucinous tumours are not. In their results, clinical characteristics associated with serum CA19-9 were larger tumour size, serum CA125 elevation, and tumour pathology (borderline or malignant). They found that the elevation of serum CA19-9 in ovarian mucinous tumours was significantly correlated with larger tumour size, with leakage as a likely mechanism. They also concluded that tumour pathology (borderline or malignant) was the only independent risk factor for serum CA19-9 elevation in primary ovarian mucinous tumours.
This also explains very high levels found in the present case as the size of the tumour was quite large and per operatively capsule was found to be ruptured and mucinous fluid was seen oozing through the capsule and the histopathology confirmed it to be mucinous carcinoma right ovary invasive endocervical type In a case reported by Madaan M et al., there was high level of CA 19-9 associated with ovarian cyst [9]. Laparotomy revealed presence of ovarian mature cystic teratoma of size 15 cm × 12 cm. Cystectomy was done. On follow-up CA 19-9 returned to normal in two months postsurgery. Studies have shown that CA19-9 could be increased in up to 50% of cases of immature cystic teratoma [10]. There are few case reports which have shown association of raised CA19-9 with benign pathology but the present is first case showing such high levels of CA19-9 associated mucinous carcinoma of ovary.
Conclusion
Marked increase in serum levels of CA 19-9 is seen mostly in pancreatic and hepatobiliary conditions. Thorough evaluation of patients with raised level of CA 19-9 should be done as these patients may have benign or malignant ovarian mucinous tumour.
[1]. Steinberg WM, Gelfand R, Anderson KK, Glenn J, Kurtzman SH, Sindelar WF, Comparison of the sensitivity and specificity of the CA19-9 and carcino-embryonic antigen assays in detecting cancer of the pancreasGastroenterology 1986 90(2):343-49.10.1016/0016-5085(86)90930-3 [Google Scholar] [CrossRef]
[2]. Dede M, Gungor S, Yenen MC, Alanbay I, Duru NK, Haşimi A, CA19-9 may have clinical significance in mature cystic teratomas of the ovaryInt J Gynecol Cancer 2006 16(1):189-93.10.1111/j.1525-1438.2006.00284.x16445632 [Google Scholar] [CrossRef] [PubMed]
[3]. Kyung MS, Choi JS, Hong SH, Kim HS, Elevated CA 19-9 levels in mature cystic teratoma of the ovaryInt J Biol Markers 2009 24(1):52-56.10.1177/17246008090240010819404923 [Google Scholar] [CrossRef] [PubMed]
[4]. Pandey D, Sharma R, Sharma S, Salhan S, Unusually high serum levels of CA 19-9 in an ovarian tumour: malignant or benign?J Clin Diagn Res 2017 11(3):QD08-QD10.10.7860/JCDR/2017/21017.950628511463 [Google Scholar] [CrossRef] [PubMed]
[5]. Brain O, Brown LHW, Suvarna S, Chapman R, Markedly elevated CA19-9 associated with benign ovarian cyst and ascitesBMJ Case Rep 2009 2009:pii: bcr11.2008.121910.1136/bcr.11.2008.121921686409 [Google Scholar] [CrossRef] [PubMed]
[6]. Pyeon SY, Park JY, Ki KD, Lee JM, Abnormally high level of CA-19-9 in a benign ovarian cystObstet Gynecol Sci 2015 58(6):530-32.10.5468/ogs.2015.58.6.53026623421 [Google Scholar] [CrossRef] [PubMed]
[7]. Kelly PJ, Archbold P, Price JH, Cardwell C, McCluggage WG, Serum CA19.9 levels are commonly elevated in primary ovarian mucinous tumours but cannot be used to predict the histological subtypeJ Clin Pathol 2010 63(2):169-73.10.1136/jcp.2009.07235520154039 [Google Scholar] [CrossRef] [PubMed]
[8]. Cho HY, Kyung MS, Serum CA19-9 as a predictor of malignancy in primary ovarian mucinous tumours: a matched case-control studyMed Sci Monit 2014 20:1334-39.10.12659/MSM.89095425073801 [Google Scholar] [CrossRef] [PubMed]
[9]. Madaan M, Puri M, Sharma R, Kaur H, Trivedi SS, Unusually high levels of CA19-9 associated with mature cystic teratoma of the ovaryCase Rep Obstet Gynecol 2014 2014:18791010.1155/2014/18791025276448 [Google Scholar] [CrossRef] [PubMed]
[10]. Novakovic S, Tumour markers in clinical oncologyRadiol Oncol 2004 38(2):73-83. [Google Scholar]