Comparison of Total and Ionic Calcium in Hypothyroidism
Vasanthan Mani1, Meenakshi Sundari Subramaniyan Natarajan2, Vinodhini Vellore Mohanakrishnan3
1 Assistant Professor, Department of Biochemistry, SRM MCH and RC, SRMIST, Kattankulathur, Tamil Nadu, India.
2 Associate Professor, Department of General Medicine, SRM MCH and RC, SRMIST, Kattankulathur, Tamil Nadu, India.
3 Professor, Department of Biochemistry, SRM MCH and RC, SRMIST, Kattankulathur, Tamil Nadu, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Meenakshi Sundari Subramaniyan Natarajan, Department of Medicine, SRM MCH and RC, SRMIST, Kattankulathur, Kanchipuram-603203, Tamil Nadu, India.
E-mail: dr.meenakshisundari@gmail.com
Introduction
Thyroid hormones are involved in various functions of human body such as metabolic activities, homeostasis of electrolytes and minerals like calcium and potassium. The blood calcium level is believed to increase glucose uptake of cells by acting as a messenger under the influence of thyroid hormone. Some studies report alteration in calcium levels with respect to the thyroid status, while other studies report alteration in ionic calcium and normal levels of total calcium levels in hypothyroidism.
Aim
To estimate and find the correlation between total and ionic calcium levels in hypothyroidism.
Materials and Methods
The study was conducted on 35 healthy controls (Groups A) and 35 hypothyroid subjects (Groups B) of age group 20-45 years. Blood samples were analysed for Thyroid Stimulating Hormone (TSH) and Free Thyroxine (FT4) by Chemiluminescence Immunoassay (CLIA), serum albumin by Bromocresol Green (BCG) method and calcium levels by the Arsenazo method. Independent student’s t-test and Pearson’s correlation were used to analyse the results. A p-value <0.05 was considered as statistically significant.
Results
The study confirmed the direct correlation between blood total (r-value 0.32, p-value <0.001) and an ionic (r-value 0.03, p-value <0.001) calcium levels in hypothyroid patients. Significant differences (p value <0.001) were observed in FT4 and TSH levels between hypothyroid and control group. However, no significant (p-value=0.498) difference was found between the albumin levels between the groups, which indirectly reflects the values of total and ionic calcium.
Conclusion
This study concluded that both total calcium and ionised calcium were decreased in patients with hypothyroidism when compared to those with euthyroid status. Thus the study highlights the need for hypothyroid patients to be screened for serum calcium levels to prevent hypocalcemia and its related complications.
Free thyroxine, Thyroid stimulating hormone, Total and ionic calcium
Introduction
Thyroid stimulating hormone (TSH) secreted by pituitary gland regulates the synthesis of two vital hormones Thyroxine (T4) and Triiodothyronine (T3). Both T4 and T3 exert negative feedback control over the hypothalamus as well as anterior pituitary, thus controlling the release of both Thyroid Releasing Hormone (TRH) from hypothalamus and TSH from anterior pituitary gland. To assess thyroid status, Free Thyroxine (FT4) and TSH are considered to be of more clinical significance [1]. These hormones are crucial in various functions such as thermoregulation, metabolic functions, and water, electrolyte and mineral homeostasis. Thyroid hormones act directly on the bones, thereby maintain the calcium homeostasis. In euthyroid state, the TSH range is 0.5-5.0 mIU/L and the FT4 range is 0.75-1.54 ng/dL. In hypothyroidism, FT4 drops below the normal reference range and TSH exceeds the upper limit of reference range along with prominent signs and symptoms such as weight gain, tiredness, hoarseness of voice, menorrhagia and dry coarse skin. Improper diagnosis of hypothyroidism or irregular follow-up of the patients on levothyroxine often can lead to overcorrection with symptoms of hyperthyroidism like palpitation, insomnia, hunger and anxiety [2]. Therefore, thyroid profile should be routinely done to determine the efficacy of treatment and management of associated symptoms.
Calcium is an important mineral which plays a major role in the formation of teeth and bones, muscle contraction, blood coagulation, normal functioning of many enzymes and normal rhythmic contraction of the heart. In hypocalcemia, ionised serum calcium levels in plasma are less than 8.5 mg/dL. The symptoms and signs of hypocalcemia include rickets in children, osteomalacia in adults, perioral paresthesias and spontaneous muscle cramps. In severe hypocalcemia, electrocardiogram shows QT interval prolongation which indicates the risk of developing ventricular tachycardia [3].
Various studies have reported normal calcium levels in hypothyroidism and both increased and decreased calcium levels in hyperthyroid patients [4-8]. Based on these conclusion, the present study was designed to evaluate the alterations in total and ionic calcium levels in hypothyroid patients and euthyroid controls and thereby emphasise on the importance of calcium estimation and the need to maintain calcium homeostasis in hypothyroid patients.
Materials and Methods
The cross-sectional study was conducted with 70 participants (35 male and 35 female) attending the Outpatient department and participants of Master Health Checkup at SRM Medical College Hospital and Research Centre, SRM IST (study conducted in year 2017).
The participants were selected by convenient sampling from the general population (aged 20-45 years), were divided into two groups, A and B with 35 hypothyroid patients and 35 euthyroid controls respectively. Individuals with normal TSH (0.5-5 mIU/L) and normal FT4 (0.75-1.54 ng/dL) levels were classified as euthyroid controls. Recently diagnosed hypothyroid patients TSH >5 mIU/L and FT4 <0.75 ng/dL were taken as subjects.
Patients with a history of alcoholism, kidney, liver and bone disorders or patients on calcium or mineral supplements or any other medication that might affect serum calcium levels were excluded from the study. Procedures performed in the present study involving human participants were conferring with the ethical standards (IEC Number: 1243/IEC/2017) of the Institution. The blood samples were collected after obtaining written consent from all the individuals under study.
Blood collection and analysis: Overnight fasting blood samples of 2-3 mL were collected in plain vials. The samples were analysed on the day of collection to avoid misinterpretations. Measurement of TSH and FT4 was based on the principle of enhanced Chemiluminescence Immunoassay (e-CLIA) in VITROS fully automated hormone analyzer [9]. Serum albumin was estimated by BCG method and total calcium by the Arsenazo method in Beckman Coulter fully automated chemistry analyzer [10]. Ionic calcium was calculated by the formula [11]:
0.25 × [0.9 + (0.55×total calcium)-(0.3×albumin)]Statistical Analysis
Statistical analysis was performed by Independent students’ t-test, and Pearson’s correlation was used to determine the correlation between total and ionic calcium levels and hypothyroidism. The results were analysed using Statistical Package for Social Sciences (SPSS). p-value <0.05 was considered as statistically significant.
Results
The study included 70 individuals divided into two Groups as A and B, normal thyroid functions as controls and hypothyroidism subjects respectively. Statistically significant (p-values <0.001) difference was observed in FT4, TSH, total and ionic calcium levels between euthyroid and hypothyroid patients [Table/Fig-1,2].
Levels of FT4, TSH and serum albumin of normal thyroid function (Group A) and hypothyroidism (Group B) participants.
| Parameters | Control Euthyroid (Group A) (n=35) | Hypothyroid Patients (Group B) (n=35) | p-values |
|---|
| Mean±SD | Mean±S.D | |
|---|
| FT4 (g/dL) | 1.34±0.45 | 0.41±0.12 | <0.001* |
| TSH (g/dL) | 3.61±1.13 | 6.28±1.01 | <0.001* |
| Albumin (g/dL) | 4.97±0.60 | 5.04±0.10 | 0.498 |
*FT4: Free thyroxine, TSH:Thyroid stimulating hormone, *Student’s t-test *p value <0.001 is highly significant
Total and ionic calcium in euthyroid (Group A) and hypothyroid (Group B) participants.
| Dependent Variable | Euthyroid (Group A) Mean±SD | Patients (Group B) Mean±SD | Mean Difference±S.E. | Significance (p) | 95% Confidence Interval |
|---|
| Lower bound | Upper bound |
|---|
| Total calcium (mg/dL) | 10.28±1.03 | 8.33±0.30 | -1.950±0.181 | <0.001* | -2.3119 | -1.5881 |
| Ionic calcium (mg/dL) | 1.24±0.11 | 0.99±0.16 | -0.250±0.033 | <0.001* | -0.3155 | -0.1845 |
S.E.: Standard error, Student’s t-test *p value <0.001 is highly significant
The calcium (total and ionic) levels of the patients with hypothyroidism were lower than that of control individuals with normal thyroid function (p-value <0.001, r-value 0.32 and 0.03 for total and ionic calcium respectively) [Table/Fig-3,4].
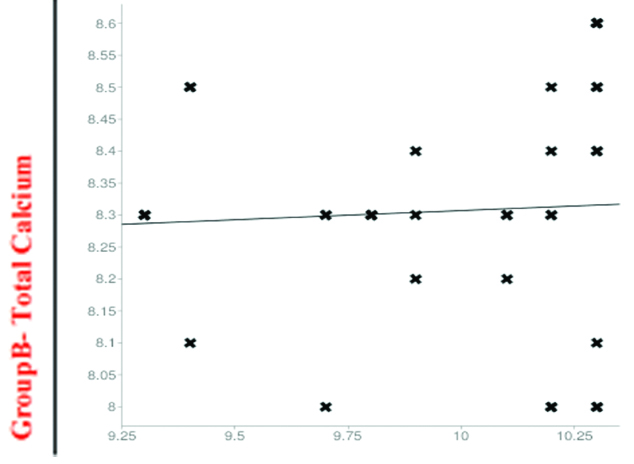
Linear regression for total calciumin hypothyroid patients.
*Group A- Total calcium
p-value <0.001, r-value is 0.32 for total calcium
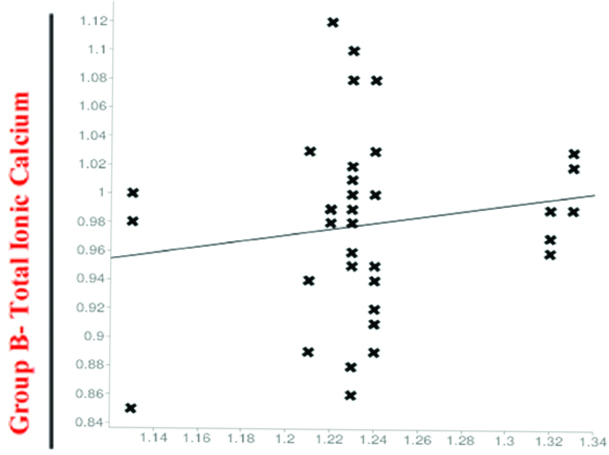
Linear regression for Ionic calcium in hypothyroid patients.
Group A- Total ionic calcium
p-value <0.001, r-value is 0.03 for ionic calcium
Discussion
The main function of FT3 and FT4 is the stimulation of osteoblastic differentiation in the bones that promotes bone resorption and increases the calcium levels in blood. The reduction in FT4 and FT3 levels in hypothyroidism leads to impairment in the mobilisation of calcium into the bone and decreased blood calcium levels [12]. In the present study, the FT4 and TSH levels were significantly decreased in the hypothyroid group as compared to the euthyroid participants. Our findings are in accordance with the study done by Murgod B and Soans G [13].
The present study showed decreased concentrations of total calcium and ionic calcium in hypothyroid patients when compared to the group of controls with normal thyroid function with a highly significant p value of <0.001. Similar results were also observed by the studies conducted by Shivaleela MB et al and Gohel MG et al and Abdel-Gayoum AA [14-16]. The study was conducted by Abdel-Gayoum AA showed decrease in blood calcium concentration in overt hypothyroid patients. Our findings were in accordance with the study conducted by Ashmaik AS et al in the year 2013 which showed decreased calcium levels in Sudanese patients with hypothyroidism [17].
While some studies delineate the association of decreased total and ionic calcium in hypothyroid patients, other studies contradict these findings. Serum calcium was found to be normal in patients with hyperthyroidism in a study conducted by Begic-Karup S et al., [4]. According to another study conducted by Sabuncu T et al, serum calcium levels were normal in hypothyroidism [5]. Susanna TY et al., concluded that there was no correlation between T3, T4, and TSH with the serum calcium levels in patients with hypothyroidism [6]. These results were in contrast to our findings. Supplementary studies are required to determine the in-detail mechanism and causes of alteration of calcium levels in thyroid disorder.
Limitation
Since we have excluded the patients with liver diseases, serum albumin was normal in all the patients in study and control group, making the ionic calcium comparison less significant in this study. The method of choice for estimating ionic calcium was traditional ion selective electrode. The sample size is relatively small, further studies with larger sample size and diverse participants are required to validate our findings. Dietary pattern of the individual should also be monitored to avoid misinterpretations.
Conclusion
Even though calcium is one of the most important mineral in our body with varied essential functions, many physicians are still unaware of the fact of abnormal low calcium levels occurring in hypothyroid patients. The present study will help them to understand the importance of screening of serum calcium in hypothyroidism patients for determining the course of treatment and prevention of the complications of hypocalcemia.
*FT4: Free thyroxine, TSH:Thyroid stimulating hormone, *Student’s t-test *p value <0.001 is highly significant
S.E.: Standard error, Student’s t-test *p value <0.001 is highly significant
[1]. Li H, Yuan X, Liu L, Zhou J, Li C, Yang P, Bu L, Zhang M, Qu S, Clinical evaluation of various thyroid hormones on thyroid functionInt J Endocrinol 2014 2014:61857210.1155/2014/61857225548564 [Google Scholar] [CrossRef] [PubMed]
[2]. HAARBURGER, David. Thyroid disease: thyroid function tests and interpretation. Continuing Medical Education, [S.l.], v. 30, n. 7, p. 241-243, jun. 2012. ISSN 2078-5143. Available at: <http://www.cmej.org.za/index.php/cmej/article/view/2515/2432>. Date accessed: 18 Mar. 2019 [Google Scholar]
[3]. Goltzman D. Clinical manifestations of hypocalcemia. Available at: https://somepomed.org/articulos/contents/mobipreview.htm?39/49/40734?source=see_link [Google Scholar]
[4]. Begic-Karup S, Wagner B, Raber W, Schneider B, Hamwi A, Waldhäusl W, Serum calcium in thyroid diseaseWein Klin Wochenschr 2001 113(1-2):65-8. [Google Scholar]
[5]. Sabuncu T, Aksoy N, Arikan E, Ugur B, Tasan E, Hatemi H, Early changes in the parameters of bone and mineral metabolism during therapy for hyperthyroidism and hypothyroidismEndocrine Research 2001 27(1-2):201-13.10.1081/ERC-10010718111428712 [Google Scholar] [CrossRef] [PubMed]
[6]. Susanna TY, Sagayaraj A, Shashidhar KN, Gomathi M, Mahesh V, A correlative study of thyroid profile and mineral status in patients with hypothyroidism-A hospital-based case control studyAsian J Pharm Clin Res 2016 9(3):292-4. [Google Scholar]
[7]. Orluwene CG, Mommoh MO, Serum phosphorus, estimated ionized and total serum calcium in industrial females with thyroid dysfunction in Port HarcourtInt J Res Med Health Sci 2013 3(4):20-24. [Google Scholar]
[8]. Dhanwal DK, Kochupillai N, Gupta N, Cooper C, Dennison EM, Hypovitaminosis D and bone mineral metabolism and bone density in hyperthyroidismJ Clin Densitom 2010 13(4):462-66.10.1016/j.jocd.2010.05.00820663698 [Google Scholar] [CrossRef] [PubMed]
[9]. Sharon Saw, Sunil Sethi, Tar-Choon Aw, Technical Evaluation of Thyroid Assays on the Vitros ECiClinical Chemistry 1999 45(4):578-80. [Google Scholar]
[10]. Goswami K, Mookherjee S, Mazumdar I, Calibration verification for olympus au 480 and meril autoquant aq 400i automatic biochemistry auto analyser using seven analytesEuropean Journal of Biomedical and Pharmaceutical Sciences 2017 4(11):682-86. [Google Scholar]
[11]. Dickerson RN, Alexander KH, Minard G, Croce MA, Brown RO, Accuracy of methods to estimate ionized and “corrected” serum calcium concentrations in critically ill multiple trauma patients receiving specialized nutrition supportJPEN J Parenter Enteral Nutr 2004 28(3):133-41.10.1177/014860710402800313315141404 [Google Scholar] [CrossRef] [PubMed]
[12]. Tuchendler D, Bolanowski M, The influence of thyroid dysfunction on bone metabolismThyroid Res 2014 7:1210.1186/s13044-014-0012-025648501 [Google Scholar] [CrossRef] [PubMed]
[13]. Murgod R, Soans G, Changes in Electrolyte and Lipid profile in HypothyroidismInternational Journal of Life science and Pharma research 2012 2(3):185-194. [Google Scholar]
[14]. Shivaleela MB, Poornima RT, Jayaprakash Murthy DS, Serum calcium and phosphorous levels in thyroid dysfunctionIndian Journal of Fundamental and Applied Life Science 2012 2(2):179-83. [Google Scholar]
[15]. Gohel MG, Shah AM, Shah AM, Makadia JS, A study of serum calcium, magnesium and phosphorus level in hypothyroidism patientsInt J Med Health Sci 2014 3(4):308-12. [Google Scholar]
[16]. Abdel-Gayoum AA, Dyslipidemia and serum mineral profiles in patients with thyroid disordersSaudi Med J 2014 35(12):1469-76. [Google Scholar]
[17]. Ashmaik AS, Gabra HM, Elzein AO, Nassr Eldin MA, Hassan EE, Assessment of Serum Levels of Calcium and Phosphorous in Sudanese Patients with HypothyroidismAsian Journal of Biomedical and Pharmaceutical Sciences 2013 3(25):21-26. [Google Scholar]