Evaluation of Impedance and Reactance in the Intensive Treatment of Lymphoedema
Jose Maria Pereira De Godoy1, Henrique Jose Pereira De Godoy2, Maria De Fatima Guerreiro Godoy3
1 Department of Cardiology and Cardiovascular Surgery, Medicine School in São José do Rio Preto (FAMERP), CNPq (National Council for Research and Development), Sao Jose do Rio Preto, São Paulo, Brazil.
2 Student, Medicine School of Universidade Federal do Mato Grosso-Cuiabá-UFMT and Research Group in the Clínica, São José do Rio Preto, SP, Brazil.
3 Department of Rehabilitation, Medicine School of Sao Jose do Rio Preto and Clinica Godoy-Brazil, Sao Paulo, Brazil.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Jose Maria Pereira de Godoy, Avenida Constituição 1306, Sao Jose do Rio Preto, Sao Paulo, Brazil.
E-mail: godoyjmp@gmail.com
Introduction
Lymphoedema is a progressive, chronic, clinical sign of an abnormal accumulation of macromolecules in the interstitial space that causes a buildup of fluids.
Aim
To evaluate specific data of bioimpedance such as impedance and reactance in the evolution of lymphoedema treatment.
Materials and Methods
A prospective quantitative study was enrolled in the Clinica Godoy-Brazil in May 2013, on 24 patients with bilateral lower limb lymphoedema (48 legs). Bioimpedance variables (impedance and reactance) were evaluated before and after five days of intensive treatment (mechanical lymphatic therapy, cervical stimulation, manual lymphatic therapy and grosgrain compression stockings) of the legs with the results being compared with a control group. The patients of the control group had arm lymphoedema without clinical evidence of swelling of the legs. All patients were weighed and underwent volumetry by the water displacement technique or perimetry (elephantiasis), and multi-frequency bioelectrical impedance before treatment and at the beginning and at the end of each day of treatment. The results are reported as descriptive statistics and Kruskal-Wallis test (Conover-Inman).
Results
Statistically significant differences were found between the study and control groups for impedance (p-value <0.0001). The ages of the 17 female and seven male patients ranged from 22 to 75-year-old (mean: 43.7 years) and ages of control group ranged from 42 to 71-year-old (mean: 51.8 years).
Conclusion
Impedance and reactance evaluations contribute to the diagnostic evaluation in the follow-up of lymphoedema treatment.
Interstitial space, Lower limb, Lymphoedema treatment
Introduction
Lymphoedema is a progressive, chronic, clinical sign of an abnormal accumulation of macromolecules in the interstitial space that causes a buildup of fluids. This is the result of a failure to form and drain lymph due to congenital or acquired changes in the lymphatic system [1]. Clinical history and physical examination are required to diagnose lymphoedema with complementary tests confirming the diagnosis. These tests directly assess the lymphatic vessels, such as the lymphography and lymphoscintigraphy, while others evaluate the severity of oedema, such as water displacement volumetry, perimetry or more recently bioimpedance [2]. Bioimpedance focuses on an evaluation of intra- and extra-cellular liquid, however, other important information such as an analysis of reactance; impedance and the phase angle have not been stressed in lymphology [3].
Bioimpedance is a non-invasive practical method based on an analysis of the resistance of the entire body to the passage of low amplitude, high-frequency electrical current by measuring the Resistance (R), Reactance (Xc) and the phase angle [4,5]. This technique is currently being used in the diagnosis and monitoring of lymphoedema and so the new knowledge gained is assisting in the evolution of this technology [4-8].
Reactance is related to the structure and function of cell membranes with respect to the extra- and intracellular fluid balance [9]. Thus, a better assessment of the elements that bioimpedance provides may contribute to widening its use. The objective of the present study was to evaluate specific data of bioimpedance such as impedance and reactance in the evolution of the treatment of lymphoedema.
Materials and Methods
A prospective quantitative study was enrolled in the Clinica Godoy-Brazil in May 2013, 24 patients with bilateral lower limb lymphoedema (48 legs), sample size was determined by using an unpublished pilot work. Bioimpedance variables (impedance and reactance) were evaluated before and after five days of intensive treatment of the legs with the results being compared with a control group. The age of the 17 female and seven male patients ranged from 22 to 75-year-old (mean: 43.7 years). The patients of the control group had arm lymphoedema without clinical evidence of swelling of the legs; their ages ranged from 42 to 71-year-old (mean: 51.8 years).
The inclusion criterion of the patients in the study group was Grade II or III leg lymphoedema of whatever origin [2]. The control Group could not have evidence of oedema of the legs. All patients who fulfilled the inclusion criterion and accepted to participate in the study were consecutively enrolled as they arrived in the clinic. Patients with lymphedema grade 1 was excluded from the study.
All patients were weighed and underwent volumetry by the water displacement technique or perimetry (elephantiasis), and multi-frequency bioelectrical impedance before treatment and at the beginning and end of each day of treatment. The In Body S10 Body Composition Analyzer (BioSpace, Seoul, Korea) was used to measure impedance and reactance. The control group had a single evaluation.
All patients underwent intensive treatment of between seven and eight hours per day which included mechanical lymphatic therapy (RAGodoy®) all day, one hour of manual lymphatic therapy (Godoy and Godoy) simultaneously to the mechanical lymphatic therapy and cervical stimulation (Godoy cervical therapy) for 15 minutes per day. A home-made compression stocking of grosgrain was used and adjusted two or three times per day depending on the reduction in volume. The study was approved by Ethical Committee in Medicine School of CAAE: 278223014.8.40.54.15.
Statistical Analysis
The results are reported as descriptive statistics including mean, median, standard deviation, and interquartile percentiles. The Friedman, Kruskal-Wallis (Conover-Inman) the Wilcoxon’s signed ranks tests were used for statistical analysis. Statistical significance was set for an alpha error of 5% (p-value <0.05).
Results
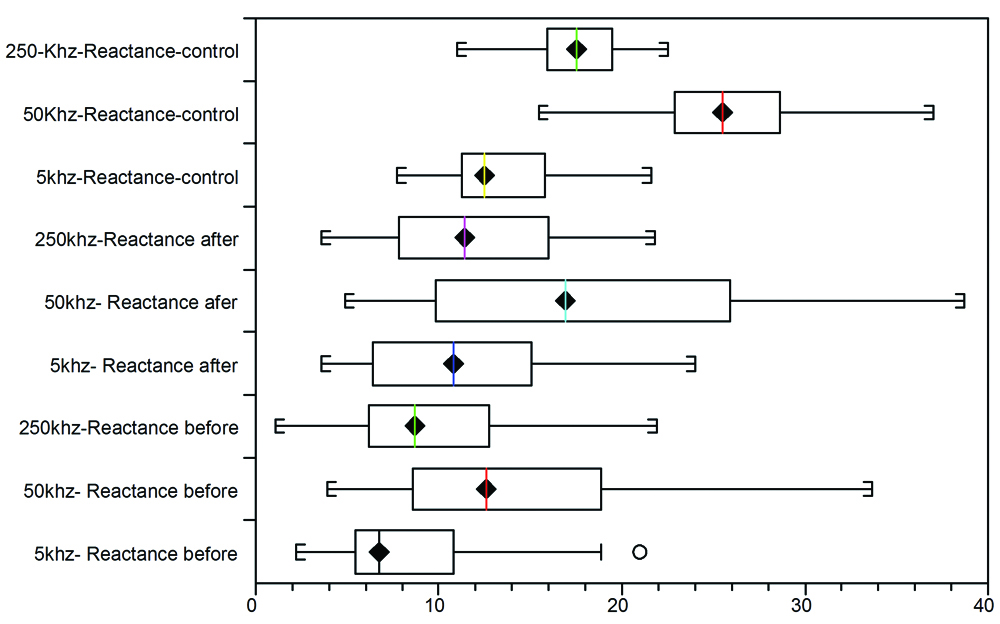
All patients had volumetric reductions at the end of the five-day treatment program. There was a statistically significant difference in respect to the impedance [Table/Fig-1,2]. The Friedman test identified a significant difference as did all the multiple comparisons using the Conover-Inman test comparing before and after treatment and with the Control Group [Table/Fig-3]. There were significant differences in respect to the reactance between the Control group and the Study group both before and after treatment [Table/Fig-4,5 and 6].
Descriptive statistics of the impedance comparing normal legs and lymphoedematous legs before and after five days of intensive treatment.
| Valid data | Mean | Standard deviation | Variance coefficient | Upper quartile | Median | Lower quartile | Minimum |
|---|
| 1 kHz before | 48 | 178.94 | 67.58 | 0.37 | 224.85 | 180.4 | 124.05 | 62 |
| 1 kHz after | 48 | 209.53 | 76.96 | 0.36 | 167.55 | 212.7 | 141.4 | 74.3 |
| 1 kHz normal | 48 | 275.27 | 31.76 | 0.11 | 302.2 | 276.5 | 252.2 | 195.6 |
| 5 kHz before | 48 | 173.15 | 65.38 | 0.37 | 214.25 | 175.4 | 121.15 | 53.3 |
| 5 kHz after | 48 | 202.54 | 74.27 | 0.36 | 256.55 | 203.4 | 137.75 | 69.1 |
| 5 kHz Normal | 48 | 267.24 | 30.57 | 0.11 | 293 | 269.1 | 243.7 | 191.1 |
| 50 kHz before | 48 | 153.12 | 55.64 | 0.36 | 192.55 | 152.95 | 109.65 | 46.8 |
| 50 kHz after | 48 | 175.86 | 62.7 | 0.35 | 223.7 | 176.25 | 120.7 | 55.9 |
| 50 kHz Normal | 48 | 231.23 | 25.38 | 0.10 | 249.85 | 230.15 | 210.3 | 170.8 |
| 250 kHz before | 48 | 138.26 | 48.72 | 0.35 | 177.3 | 137.55 | 99.65 | 40 |
| 250 kHz after | 48 | 157.29 | 55.25 | 0.35 | 198.95 | 155.7 | 111.8 | 47.4 |
| 250 kHz normal | 48 | 205.36 | 22.84 | 0.11 | 219.9 | 201.3 | 190.65 | 154.7 |
| 500 kHz before | 48 | 134.33 | 47.28 | 0.35 | 172.85 | 133.45 | 96.35 | 38 |
| 500 kHz after | 48 | 152.64 | 53.28 | 0.35 | 193.65 | 152.4 | 108.65 | 45 |
| 500 kHz normal | 48 | 198.77 | 22.37 | 0.11 | 212.7 | 194.4 | 185 | 150.1 |
| 1 MHz RL before | 48 | 130.21 | 46.15 | 0.35 | 167.55 | 129.2 | 94 | 35.9 |
| 1 MHz RL after | 48 | 147.75 | 52.34 | 0.35 | 188.85 | 146.65 | 104.6 | 41.9 |
| 1 MHz normal | 48 | 192.47 | 21.52 | 0.11 | 206.25 | 188.5 | 179.6 | 145.5 |
Box and whisker plot comparing interquartile ranges of impedance at different frequencies between the control Group and the Treatment Group both before and after five days of treatment.
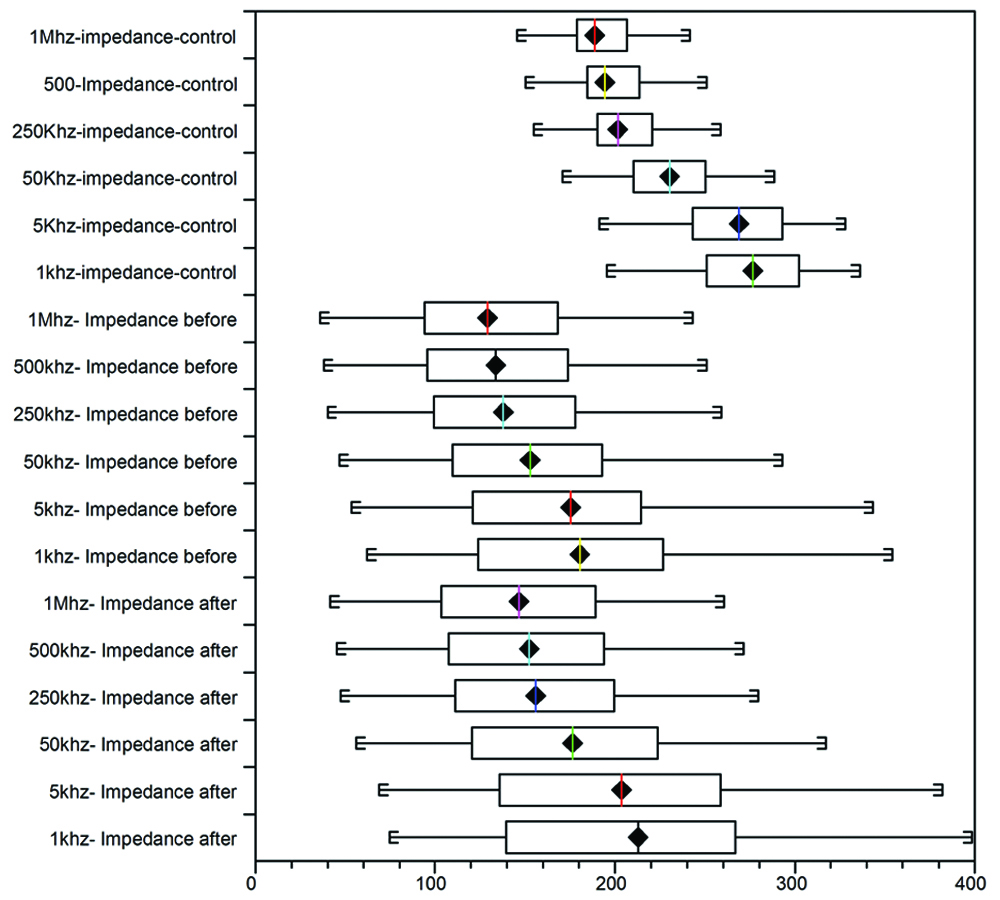
Statistical analysis of impedance at frequencies of 1 kHz, 5 kHz, 250 kHz, 500 kHz, and 1 MHz, using the Kruskal-Wallis test: all pairwise comparisons (Conover-Inman) between the Control Group and the Treatment Group, before and after five days of intensive treatment.
| 1 kHz Impedance after | 1 kHz Impedance before | p-value =0.0148 |
| 1 kHz Impedance after | 1 kHz impedance normal | p-value <0.0001 |
| 1 kHz Impedance before | 1 kHz impedance normal | p-value <0.0001 |
| 5 kHz Impedance after | 5 kHz Impedance before | p-value =0.0199 |
| 5 kHz Impedance after | 5 kHz impedance normal | p-value <0.0001 |
| 5 kHz Impedance before | 5 kHz impedance normal | p-value <0.0001 |
| 50 kHz Impedance after | 50 kHz Impedance before | p-value =0.0274 |
| 50 kHz Impedance after | 50 kHz impedance normal | p-value <0.0001 |
| 50 kHz Impedance before | 50 kHz impedance normal | p-value <0.0001 |
| 250 kHz Impedance after | 250 kHz Impedance before | p-value =0.031 |
| 250 kHz Impedance after | 250 kHz impedance normal | p-value <0.0001 |
| 250 kHz Impedance before | 250 kHz impedance normal | p-value <0.0001 |
| 500 kHz Impedance after | 500 kHz Impedance before | p-value =0.0354 |
| 500 kHz Impedance after | 500 kHz Impedance normal | p-value <0.0001 |
| 500 kHz Impedance before | 500 kHz Impedance normal | p-value =0.0001 |
| 1 MHz Impedance after | 1 MHz Impedance before | p-value =0.035 |
| 1 MHz Impedance after | 1 MHz impedance normal | p-value <0.0001 |
| 1 MHz Impedance before | 1 MHz impedance normal | p-value <0.0001 |
Descriptive statistics of the reactance between the Control Group and the Treatment Group both before and after five days of intensive treatment.
| Variables | 5 kHz before | 5 kHz after | 5 kHz control | 50 kHz before | 50 kHz after | 50 kHz control | 250 kHz before | 250 kHz after | 250 kHz control |
|---|
| Valid data | 48 | 48 | 48 | 48 | 48 | 48 | 48 | 48 | 48 |
| Mean | 8.30 | 10.80 | 13.21 | 14.57 | 18.51 | 25.85 | 9.72 | 11.85 | 17.49 |
| Standard deviation | 4.18 | 4.97 | 3.48 | 7.95 | 9.08 | 3.48 | 4.95 | 4.82 | 2.65 |
| Variance coefficient | 0.50 | 0.46 | 0.26 | 0.54 | 0.49 | 0.19 | 0.50 | 0.40 | 0.15 |
| Upper quartile | 10.7 | 15.5 | 15.8 | 18.65 | 25.75 | 28.45 | 12.7 | 15.8 | 19.5 |
| median | 6.75 | 10.80 | 12.5 | 12.6 | 16.9 | 25.5 | 8.7 | 15.8 | 17.55 |
| Lower quartile | 5.45 | 6.4 | 11.3 | 8.85 | 9.85 | 22.9 | 6.25 | 7.8 | 15.95 |
Statistical analysis of reactance using the Kruskal-Wallis test: all pairwise comparisons (Conover-Inman) between the Control Group and the Treatment Group, before and after five days of treatment.
| 5 kHz Reactance before | 5 kHz Reactance after | p=0.0077 |
| 5 kHz Reactance before | 5 kHz Reactance-control | p<0.0001 |
| 5 kHz Reactance after | 5 kHz Reactance-control | p=0.0043 |
| 50 kHz Reactance before | 50 kHz Reactance after | p=0.0027 |
| 50 kHz Reactance before | 50 kHz Reactance control | p<0.0001 |
| 50 kHz Reactance after | 50 kHz Reactance control | p<0.0001 |
| 250 kHz Reactance before | 250 kHz Reactance after | p=0.022 |
| 250 kHz Reactance before | 250 kHz Reactance control | p<0.0001 |
| 250 kHz Reactance after | 250 kHz Reactance control | p<0.0001 |
Box and whisker comparing interquartile ranges of reactance at different frequencies between the Control group and the Treatment group both before and after five days of treatment.
Discussion
The present study shows that an analysis of the impedance, reactance can assist in the evolution of the treatment of lymphoedema. These parameters can improve significantly with clinical treatment, but this assessment has not been employed in the treatment of lymphoedema. In this study with the treatment, significant differences in the impedance were identified at every frequency from 1 kHz to 1 Mhz, but after treatment, there still was a significant difference compared to the Control group. This shows that the treatment improves the fluid balance. The reactance improved significantly at 5 kHz, 50 kHz and 250 kHz with treatment, however, there was still a significant difference compared to the Control group, but after five days of treatment it was still not normal. Clinically, there was a volumetric reduction in the Study group, however, the size of the legs were not normal at the end of the 5-day treatment program. A previous study shows that this reduction is around 50% of the volume per week [1]. Therefore, the oedema was not improved completely.
Another study with this group of patients showed a redistribution of fluid to other regions of the body including the arms and trunk [10]. Hence, besides the mobilisation of liquids which is normally evaluated by bioelectrical impedance, authors believe that the Impedance and reactance should also be evaluated during the evolution of these patients.
Limitation
Age of the control group could not be standardised with the study group.
Conclusion
Impedance and reactance evaluations contribute to the diagnostic evaluation in the follow-up of lymphoedema treatment. Bioimpedance is a diagnostic method of volume and compared to volumetry by water displacement technique, it is suggested as gold standard.
[1]. Pereira De Godoy JM, Franco Brigidio PA, Salles Cunha SX, Batigália F, De Fatima Guerreiro Godoy M, Mobilization of fluids in large volumetric reductions during intensive treatment of leg lymphoedemaInt Angiol 2013 32(5):479-82. [Google Scholar]
[2]. Lee BB, Andrade M, Antignani PL, Boccardo F, Bunke N, Campisi C, Damstra R, Diagnosis and treatment of primary lymphoedema. Consensus Document of the International Union of Phlebology (IUP)-2013Int Angiol 2013 32(6):541-74. [Google Scholar]
[3]. Godoy JMP, Fortuny EI, Godoy HJP, Godoy MFG, Phase angle in the assessment of intensive outpatient treatment of primary lower limb lymphoedemaJ Phlebol Lymphol 2017 10(1):12-15. [Google Scholar]
[4]. Cornish BH, Bunce IH, Ward LC, Jones LC, Thomas BJ, Bioelectrical impedance for monitoring the efficacy of lymphoedema treatment programmesBreast Cancer Res Treat 1996 38:169-76.10.1007/BF018066718861835 [Google Scholar] [CrossRef] [PubMed]
[5]. Cornish BH, Thomas BJ, Ward LC, Hirst C, Bunce IH, A new technique for the quantification of peripheral oedema with application in both unilateral and bilateral casesAngiology 2002 53:41-47.10.1177/00033197020530010611863308 [Google Scholar] [CrossRef] [PubMed]
[6]. Hayes S, Janda M, Cornish B, Battistutta D, Newman B, Lymphoedema secondary to breast cancer: how choice of measure influences diagnosis, prevalence, and identifiable risk factorsLmphology 2008 41:18-28. [Google Scholar]
[7]. Stanton A, Modi S, Mellor R, Levick R, Mortimer P, Diagnosing breast cancer-related lymphoedema in the armJournal of Lymphoedema 2006 1:12-15. [Google Scholar]
[8]. Ward LC, Bioelectrical impedance analysis: proven utility in lymphoedema risk assessment and therapeutic monitoringLymphatic Res Biol 2006 4:51-56.10.1089/lrb.2006.4.5116569209 [Google Scholar] [CrossRef] [PubMed]
[9]. Baumgartner RN, Chumlea WC, Roche AF, Bioelectric impedance phase angle and body compositionAmerican Journal of Clinical Nutrition 1988 48(1):16-23.10.1093/ajcn/48.1.163389323 [Google Scholar] [CrossRef] [PubMed]
[10]. Godoy JMP, Godoy HJP, Godoy MFG, Subclinical systemic lymphoedema manifesting early in patients with clinical lymphoedemaInternational Journal of Development Research 2018 8(9):23041-44. [Google Scholar]