Given that women account for the majority of medical visits, they have a special position in the field of medicine [5]. Gynaecology is a branch of specialised medicine, which involves diagnosis and treatment of women diseases, childbirth, infertility, and gynaecological operations. Regarding the strong dependence of physical and mental health on each other, the internal power is a factor of psychological health and well-being [6]. The combination of gynaecology with psychology is essential for both patients and healthcare providers [5].
In some psychosomatic therapies, such as yoga and coping strategies, a combination of psychological and physiological methods has been used. Yoga is a mindfulness sport that causes mental and physical relaxation [7]. It is a combination of many activities including concentration, balance, stretching and respiratory exercises [8]. Moreover, coping strategy is a technique to deal with stress, which has three parts including distraction [9].
The distraction techniques are a cognitive-behavioural approach in the field of psychology [10]. The cognitive-behavioural counseling methods is a branch of counseling methods that include 20 counseling protocols [9,10]. The distraction technique is one of these protocols and a sub-branch of a series of coping strategy [10]. The distraction technique has been effective in controlling emotions such as fear, stress, anxiety, and anger by means of mental distraction [11]. In addition, the distraction techniques can be effective in pain control by affecting the central nervous system and free nervous transmitters [12]. In recent years, the distraction technique arose interest in researchers [13]. Among distraction techniques are counting numbers, remembering a poetry, reviving a pleasant memory or image, remembering a joke, avoiding thinking [11], using distraction cards [14] and virtual reality [15], and watching TV [16].
Many studies have been conducted based on this theory with a concentration on the distraction technique. The pain management should be considered as the first priority in meeting physiological needs [17], and distraction is the therapeutic method by which the patient is sensually stimulated for pain reduction [18]. Moreover, the distraction technique reduces psychological emotions, including fear and anxiety [11]. The signs of fear are an organism’s response to a stressful factor [19] and anxiety in an unpleasant emotional state characterised by the feeling of uneasiness, discomfort, excitement, stress and panic [20]. A review study reported the effectiveness of distraction technique in improving pain management in women receiving midwifery services (episiotomy, IUD placement, hysteroscopy, uterine aspiration, and endometrial biopsy) [15]. Another study proposed distraction technique; as a solution to patients with Persistent Genital Arousal Disorder (PGAD) [21].
Many studies have investigated the effect of distraction techniques on different areas of medicine. Following reasons encouraged the researchers to perform a systematic review into clinical trials in the field of obstetrics and gynaecology: (i) important role of mental health in promoting physical health; (ii) dependence of mental and physical health in the field of gynaecology and midwifery; and (iii) low-cost and accessibility of this technique for controlling the emotions and pain.
Materials and Methods
Search Strategy and Selection Procedures
This systematic review investigated clinical trials on the topic, the effectiveness of distraction techniques in obstetrics and gynaecological services. The search process was initiated on 23 October 2018 without time limit to find English and Farsi articles either published or unpublished. The Data bases of Cochrane Library, Web of Sciences, PubMed, Scopus, Google Scholar, CINHAL and Persian databases including SID, Magiran, and Barakat Knowledge Network System were systematically searched and then other articles and references of review studies were manually searched.
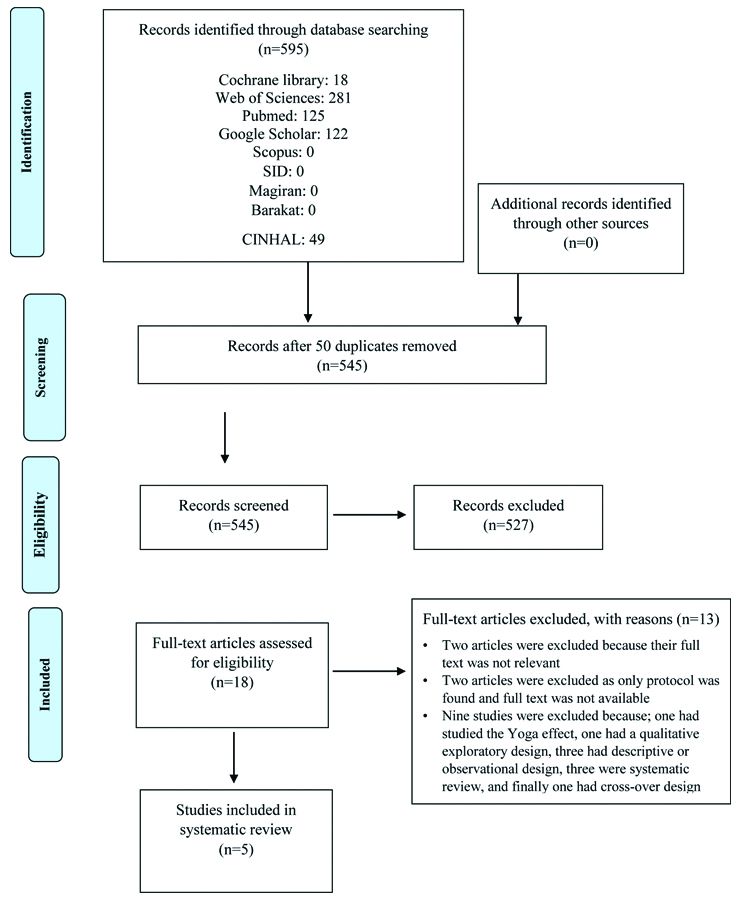
The search results are presented in a PRISMA chart [Table/Fig-1]. The keywords used to search the articles were in compliance with MeSH terminology. In addition to MeSH keywords, free keywords were also used for searching the articles. The distraction or distraction technique keywords, along with following keywords were used using + or AND with keywords of Midwife, Birth Attendants, Traditional Midwives, Traditional Birth Attendant, and Genital Diseases, Female, Gynaecologic Surgical Procedures, Reproductive Medicine, Obstetrics, Pregnancy Complications, Obstetric Surgical Procedures, Gynaecology and Gynaecological diseases. To ensure, the search process was conducted once again by using keywords of dysmenorrhea, vomiting, nausea, pregnancy, delivery and cesarean section. [Appendix 1] shows the electronic search strategy.
After validating the topic and content of the relevant studies, data was extracted by designing a table-like checklist to record specifications of the trials. To avoid bias, all extraction stages and study of references were done by two independent researchers.
Criteria for Study Entry
Types of studies: Clinical trial with parallel groups, as well as full text articles in English and Farsi in the field of obstetrics and gynaecology were included.
Types of participants: The participants were females visiting for gynaecologic examinations or women of any age group visiting for obstetrics-gynaecology services.
Types of interventions: The effect of different types of distraction techniques on outcome of patient, visiting obstetrics and gynaecology centres.
Exclusion Criteria
Studies into combination methods, such as yoga and coping strategies, were excluded.
Types of outcome measures: Severity of pain, anxiety and stress
Quality Assessment and Data Extraction
Two authors individually investigated the acceptability and quality of the articles. Any disagreement was resolved in a discussion session with a third author. Evaluation of the quality of articles was done using Cochrane Handbook for Systematic Reviews of Interventions version 5.2.0 (updated June 2017). This is a standard instrument used for investigating the quality of clinical trials. It can mark any types of bias in selection, performance, detection, attrition, reporting and other biases. Data extracted from trials included name of the author, year of the study, design of the study, site of the study, number of participants, inclusion criteria, characteristics of intervention, measured outcomes, ethical approval, and funding.
In the first stage, 595 articles were collected from data bases. Among them, 545 articles were excluded due to irrelevancy and repetition. Finally, 18 articles were found to be eligible, off which 13 were excluded from the final review and uitimately 5 articles were taken up the analysis. Specifications of the excluded studies are presented in [Appendix 2] [15,22,23-33]. Characteristics of the included studies and authors’ judgements about each study are presented in [Table/Fig-2].
Characteristics of included studies.
| Locsin RG [34] |
|---|
| Metdods | Study design: Controlled trialTrial location: Philippines |
| Participants | Number of participants: 24 female patients who admitted at the department of Obstetrics and GynaecologyEligibility criteria: Age 21 to 60-year-oldResidents of the Negros Island, Philippines |
| Intervention | Intervention: “Listen to favourite music 30 minutes before closing the surgical incision as distraction and repeat every two hours for 15 minutes”Control: “Routine care without favorite music” |
| Outcome | Primary outcome: “Musculoskeletal, verbal and physiologic-autonomic pain reactions among patients in the first and second 24 hours after surgery, which measured by Overt Pain Reaction Rating Scale”Secondary outcome: Blood pressure, pulse rate, and respirational rate |
| Notes | Ethics approval: “Ethics approval has not been reported” |
| Risk of bias |
| Bias | Authors’ judgement | Support for judgement |
| Random sequence generation (Selection bias) | High risk | Randomisation technique has not been reported, and respect to the phrase “selected post-operative patients”, it seems randomisation be at high risk. |
| Allocation concealment (Selection bias) | High risk | “Participants were paired according to age, type of surgery educational attainment and operative experience” |
| Blinding of participants and personnel (Performance bias) | High risk | Blinding has not been mentioned and there is no evidence for masking. |
| Blinding of outcome assessor (Detection bias) | High risk | Blinding has not been mentioned and there is no evidence for masking |
| Incomplete outcome data (Attrition bias) | Low risk | “None of the 24 enrolled women were withdrawn from the study for any reason” |
| Selective reporting (Reporting bias) | Low risk | “All the pre-specified outcomes in the method section were addressed adequately” |
| Other biases | High risk | Ethics approval, conflict of interest and the funding organisation have not been reported. |
| Berenson AB et al., [35] |
| Methods | Study design: Randomised trialTrial location: The University of Texas Medical Branch. Galveston, Texas, United States |
| Participants | “Number of participants: 89 children aged 3-8 years for genital examination”Eligibility criteria: not reported |
| Intervention | Intervention: “Passive play (being read to), active play (singing, blowing bubbles) and watch the movie with the help of the virtual reality device”Control: No control group |
| Outcome | Primary outcome: “PHYSDIS (reaction related to body movements), VERDIS (oral expressions caused by fear or discomfort), EMOS (demand for verbal or physical supports from parents) and child satisfaction” |
| Notes | Ethics approval: “Ethics approval has not been reported” |
| Risk of bias |
| Bias | Authors’ judgement | Support for judgement |
| Random sequence generation (Selection bias) | Unclear | Randomisation technique has not been reported |
| Allocation concealment (Selection bias) | Unclear | “Children were randomly assigned to one of three distraction techniques” but there is no evidence for random assignment |
| Blinding of participants and personnel (Performance bias) | High risk | “Children were encouraged by the research assistant” |
| Blinding of outcome assessment (Detection bias) | High risk | “Research assistant recorded the child’s behaviours” |
| Incomplete outcome data (Attrition bias) | Low risk | “None of the 89 enrolled children were withdrawn from the study for any reason” |
| Selective reporting (Reporting bias) | Low risk | “All the pre-specified outcomes in the method section were addressed adequately” |
| Other biases | High risk | Ethics approval, conflict of interest and the funding organisation have not been reported. |
| Urech C et al., [36] |
| Methods | Study design: Randomised controlled trialTrial location: University Women’s Hospital of Basel, Switzerland |
| Participants | Number of participants: 93 pregnant women Eligibility criteria: Gestational age 18-32 weeks, detection of preterm labour, familiarity and availability to the internet, being conversant with German language, low risk pregnancy, not taking progesterone, no substance abuse (except nicotine), low risk for mental disorders and suicide |
| Intervention | Intervention: “It consisted of six weekly sessions about (1) psych-education of stress during pregnancy, (2) relaxation training, (3) emotional training with main focus on pregnancy-related anxiety, (4) cognitive training, (5) problem solving and training of enjoyment, and (6) psych-education on and coping with difficulties in the upcoming motherhood”Control: Six stress management counseling sessions, writing short story, listen to radio plays, Quiz games |
| Outcome | Primary outcome: Gestational age at birth, birth weight, height, and birth rate before 37 weeksSecondary outcome: “Anxiety related to pregnancy, frequency of worries about the health of the woman and the physical issues related to pregnancy, baby’s health, childbirth and child care, examine the perceived stress level, depression, check the amount of cortisone saliva” |
| Notes | Ethics approval: The Ethics Committee approved the study and informed consent from have been received from all participants (Grant number: CR13I1_135,060).Funding: Supported by the National Science Foundation. |
| Risk of bias |
| Bias | Authors’ judgement | Support for judgement |
| Random sequence generation (Selection bias) | Low risk | “Random assignment was prepared with the help of the website random.org” |
| Allocation concealment (Selection bias) | Unclear | “Women were randomly assigned to either the six weeks IB-CBSM intervention or the CG”, this information is not sufficient for judgement. |
| Blinding of participants and personnel (performance bias) | High risk | Due to the type of intervention, there was no possibility of blindness |
| Blinding of outcome assessment (Detection bias) | Unclear | Not reported |
| Incomplete outcome data (Attrition bias) | High risk | Out of 212 screened pregnant women, a total of 93 women were included in the study and psychological measures were performed only for 52 women. Study flow chart has been reported, but we don’t know the 41 withdrawn mothers, dropped out from which group. |
| Selective reporting (Reporting bias) | Low risk | All outcomes in the method section were addressed adequately |
| Other bias | Low risk | Ethics approval has been obtained.There was no conflict of interest.The funding organisation has been reported. |
| Shourab NJ et al., [37] |
| Methods | Study design: Randomised controlled trialTrial location: Mashhad University of Medical Sciences, Mashhad, Iran |
| Participants | Number of participants: 32 primiparous women undergoing labourEligibility criteria: “Iranian females, low risk singleton pregnancy and labour without congenital anomaly with Apgar score 7-10, without any psychological disease or mother’s addiction, lacking motion sickness or headache, and having literacy” |
| Intervention | Intervention: “In addition to taking lidocaine, audiovisual glasses were given to the intervention group before the repair and they were asked to watch the 42-minute movie”Control: After the childbirth and five minutes before the start of repair, lidocaine was infiltrated. |
| Outcome | Primary outcome: “Anxiety in primiparous women during episiotomy repair” |
| Notes | Ethics approval: “The ethics committee of Mashhad University of Medical Sciences (code 89600) has approved this research”Funding: “This study has been funded by the Research Affairs of Mashhad Medical University”There was no conflict of interest. |
| Risk of bias |
| Bias | Authors’ judgement | Support for judgement |
| Random sequence generation (Selection bias) | Low risk | Random sequence generated by dropping a coin |
| Allocation concealment (Selection bias) | Low risk | “Allocation of the groups after childbirth into intervention and control groups was done by dropping a coin. Head showed the first person of the intervention group and then samples were distributed into the two groups” |
| Blinding of participants and personnel (Performance bias) | High risk | Participants and staff were not blinded. |
| Blinding of outcome assessor (Detection bias) | Unclear | Blinding of outcome assessor has not been reported. |
| Incomplete outcome data (Attrition bias) | Unclear | Two participants withdrawn of the study (The reason has not been mentioned), study flow chart not reported, we don’t know the two mothers when left the study, before or after allocation |
| Selective reporting (Reporting bias) | Low risk | All the pre-specified outcomes in the method section were addressed adequately |
| Other biases | Low risk | “Ethics approval has been obtained, there was no conflict of interest, the funding organisation has been reported” |
| Manesh MJ et al., [38] |
| Methods | Study design: Randomised controlled trialTrial location: Iran University of Medical Sciences, Tehran, Iran |
| Participants | Number of participants: 100 childbearing womenEligibility criteria: “1) 4-cm dilated cervix; 2) intact membrane; 3) no indication for cesarean section; 4) no history of allergy, and asthma; 5) no pulmonary or heart diseases, high blood pressure, diabetes, or infertility; and 6) no cervical cerclage in the current pregnancy” |
| Intervention | Intervention: “The experimental group entered into snoezelen room with comfort conditions combined with light, music, lavender essence, food and drink, in addition women could walk, sit, or lay down based on their wishes”Control: “The control group received all services that provided to the intervention group except room design” |
| Outcome | Primary outcome: “pain intensity, duration of labour, and perinea status in nulliparous women” |
| Notes | Ethics approval: “The Ethics Committee of the Iran University approved this research”.Declaration of interest: “There was no conflict of interest” |
| Risk of bias |
| Bias | Authors’ judgement | Support for judgement |
| Random sequence generation (Selection bias) | Low risk | “Random sequence generation was done by using block randomization with 4 and 6 blocks” |
| Allocation concealment (Selection bias) | Low risk | “The allocation sequence was generated by statistician, using sealed opaque envelopes to provide concealment allocation to the group” |
| Blinding of participants and personnel (Performance bias) | High risk | “Participants and staff were not blinded” |
| Blinding of outcome assessor (Detection bias) | Unclear | Blinding of outcome assessment has not been reported. |
| Incomplete outcome data (Attrition bias) | Low risk | “None of the 100 participants were withdrawn from the study for any reason” |
| Selective reporting (Reporting bias) | Low risk | All the pre-specified outcomes in the method section were addressed adequately. |
| Other biases | Low risk | “Ethics approval has been obtained, there was no conflict of interest, the funding organisation has been reported” |
Locsin RG used Overt Pain Reaction Rating Scale (OPRRS) to investigate the effect of music therapy on the severity of pain in patients after gynaecological operation [34]. Berenson AB et al., used Observation Scale of Behavioural Distress and the Faces Rating Scale to measure the behavioural distress in the girls visiting for gynaecological examination [35]. Urech C et al., in a study into stress management using distraction techniques in women diagnosed with preterm labour measured following outcomes: Stress in pregnant women using the Perceived Stress Scale (PSS), anxiety using the Anxiety Scale for Pregnancy (ASP), postpartum depression using Edinburgh Postnatal Depression (EPDS), and cortisol response using Cortisol Awakening Response (CAR) [36].
Shourab NJ et al., investigated the effect of virtual reality on women anxiety during episiotomy repair using Spielberger State-Trait Anxiety Inventory (STAI) [37]. Manesh MJ et al., investigated the effect of a distraction technique on the severity of delivery pain and postpartum perineal status using Visual Analogue Scale (VAS) [38].
Methodological Quality
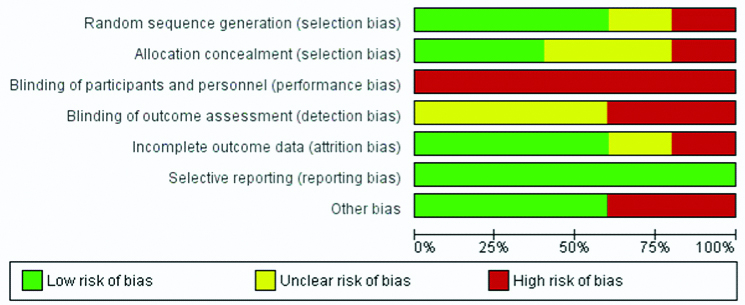
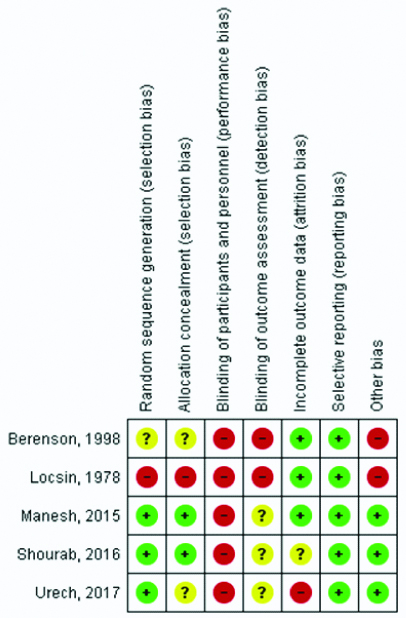
All included articles were with a clinical trial design. Given the selection bias, only two studies were at low-risk of selection bias [36,37], one study had uncertain status and there was not enough data for the judgsment [35]. In addition, two studies published before 2000 had high risk of bias and none of the studies were blinded [37,38]. As a result, they had high [28,34] or unclear risk of bias [35,37]. Detection bias was high or unclear in all included trials, and attrition bias was low in three studies [28,34,37] and high in two studies [36,37]. All trials were low risk for reporting bias [31-38]. Among the five reviewed trials, ethics approval, conflict of interest andfunding hadn’t been mentioned in two studies [34,35] and the riskof other bias was low risk in three studies [35-37]. Risk of Bias Graph and Summary are reported in [Table/Fig-3,4].
Results
Locsin RG conducted a study to determine the effect of music therapy on the severity of pain in patients after gynaecological operation. In this study, 24 women visiting medical centre of the university between 25 January and 10 April were included. They were equally divided into the intervention and control groups. The inclusion criteria were women aged 21-60 years, living in Philippine island and receiving gynaecological operations. The intervention group received music therapy 30 minutes prior to the operation. They also listened to music for 15 minutes every two hours during the first 48 hours after the surgery. The researcher measured the intensity of pain using the OPRRS. Moreover, data related to blood pressure, heart rate, respiration rate, and amount of consumed analgesics were recorded. The control group received similar care except from music therapy. Provision of care services continued for 48 hours after the surgery. Results showed that the intensity of pain was significantly lower in the first and second 24 hours in the intervention group that listened to their favourite music compared to the control group (p<0.01) [34].
Berenson AB et al., conducted a study to investigate the effects of video on the severity of behavioural distress and satisfaction of prepubescent girls referring to gynaecology clinic for genital examination. In this study, the participating African-American and Spanish-American girls aged 3-8 years were with undamaged hymen and no history of sexually abused, visiting for gynaecological examinations. They were included after obtaining their parents’ consent. A total of 89 eligible girls were included after obtaining oral consent of their parents and divided into three groups receiving three different distraction techniques including passive play (being read to), active play (singing, blowing bubbles) and watch the movie with the help of the virtual reality device. Active play group, passive play group, and virtual reality group included 28, 26, and 35 participants, respectively. In this study, the child was placed in lithotomy position and the nurse, child, and mother implemented the intervention as they were trained. Then, the research assistant scored the patient behaviour and reaction in the first six minutes based on the behaviour coding system. This paediatric behaviour coding system, used for data collection, included three codes for three behaviours: PHYSDIS (reaction related to body movements), VERDIS (oral expressions caused by fear or discomfort), EMOS (demand for verbal or physical support from parents). The first researcher’s assistant was informed via a headphone when to observe the child’s behaviour and when to score his/her behaviour. During the study, the second researcher’s assistant asked the child to score satisfaction of examination, distraction technique, and the doctor. The mean age of participants was 6±0.9 years. Approximately, 41% of them were African-American, 34% were Mexican-American, and 25% were white. According to the result, 53 participants (60%) had a history of genital examination by the first author. The multivariate ANCOVA showed that in the paediatric behaviour coding system, the physical distress or reactions related to body movements were the most common behaviours during genital examination of children. According to the paediatric behaviour coding system, all three forms of behavioural distress in the passive play group was greater than the active play group, and in this group, more than the watch the movie with the help of the virtual reality device {F=2.13, df=8, p<0.04}. The three distraction techniques had similar effects on children with different ethnicity and race {F=1.49, df=8, p>0.16} and they were satisfied of all three techniques {χ2=6.84, df=2, p=0.03}. The level of satisfaction of examination was higher in the virtual group than passive group (p=0.03), and also higher in the virtual group than active group (p=0.01). The participating girls were equally satisfied by the examiner [35].
Urech C et al., in a randomised controlled intervention study conducted in a hospital in Switzerland, entitled “Efficacy of an Internet-Based Cognitive Behavioural Stress Management (IB-CBSM) training in women with idiopathic preterm labour,” examined 212 pregnant women at the gestational age of 18-32 weeks. Among them, 93 eligible women were enrolled and assigned into the intervention (n=43) and control (n=50) groups. The inclusion criteria were women at gestational age of 18-32 weeks with a diagnosis of preterm labour, who were familiar with German language and had knowledge of internet and access to it. Women at high risk of complication (placenta previa, abnormalities of the uterus and cervix, premature rupture of membranes, etc.,), women receiving progesterone, women positive to psychotherapy and suicide screening, and women with substance abuse (except nicotine) were excluded. In this study, the intervention was implemented with minimum face-to-face contact, that the participants received counseling services online. Each participant was in an online contact with one out of four psychologists in this study. These four psychologists received six weekly counseling training sessions: stress psychology during pregnancy, relaxation, emotional training with a concentration on pregnancy anxiety, cognitive training, problem solving, enjoying from training and psychology training, coping with maternal problems in future. Conditions for the control group were similar to the intervention group, except that they controlled their stress using distraction techniques, namely listening to radio narrations, playing online games, and writing short stories. The participants emailed their weekly feedback to one of the four psychologists specified to them earlier. Study results showed no statistically significant difference between the two study groups and both methods, namely distraction and IB-CBSM, were effective in reducing psychological and social depression. Moreover, there was no significant effect on labour outcomes and cortisol parameters [36].
Shourab NJ et al., conducted a controlled clinical trial in Mashahd-Iran to determine the effect of virtual reality on anxiety during and after episiotomy repair in primiparous women. The inclusion criteria were: Iranian nationality, low risk pregnancy, labour without congenital abnormality with Apgar score of 7-10, no psychological disorder or addiction, no motor disease or headache, and should be literate. The exclusion criteria were: disease or auditory disorder, taking sedatives (except normal dose of lidocaine), and obstetrics complications or bleeding requiring emergency care. In this study, 32 primiparous women were randomised into the control and intervention groups. In addition to taking lidocaine, the intervention group was asked to watch a 42-minute virtual reality movie. The control group only received lidocaine. Results showed no significant between-group difference in the second stage of delivery, laceration of other parts of the birth canal, frequency of oxytocin infusion, amniotic sac rupture time, spontaneous delivery, contractions, fatigue, and degree of fasting. The mean episiotomy depth in the intervention and control groups was 2.5±0.6 and 2.1±0.5 respectively. The Mann-Whitney U test showed a statistically significant difference between groups in episiotomy depth (U=69.0, p=0.042). In addition, mothers in both groups were satisfied of their pregnancy and newborn sex. There was also no significant difference between group in the weight and height of the newborns. In addition, there was a significant difference between group in the mean score of anxiety before, during, and after the repair (p=0.000) [37].
Manesh MJ et al., executed a study to assess the effect of the Snoezelen room condition on the first and second stages of delivery, intensity of pain, perineum status, and frequency of C-section. This clinical trial was conducted in Tehran-Iran. The inclusion criteria were 4 cm dilatation, undamaged amniotic sac, no need for emergency C-section, no medical history of asthma and allergy, mothers without pulmonary, cardiac, hypertension, or infertility problems, and no cerclage in the current pregnancy. A total of 100 pregnant women were equally assigned to the control and intervention groups, using randomised block design in two blocks of sizes 4 and 6. Participants in need of emergency C-section after randomisation were excluded. At the time of delivery, the participants in the intervention group were transferred to special snoezelen rooms characterised by pleasant light, music, lavender smell, foods, and drinks, and they could freely walk or sit. On the other hand, the control group received only the routine care. A Visual Analogue Scale (VAS) was used to measure the intensity of pain in the first stage in the delivery room (first three hours) once per hour. Then, the severity of pain was measured once in the second delivery stage (from complete cervical dilatation to crowning). Results showed that only 2 out of 100 parturient women had undamaged perineum, both from the intervention group. The frequency of episiotomy (by a midwife or obstetrician) was 4% in the intervention group; whereas, it was reported 34% in the control group (p=0.02). This significant difference was due to higher prevalence of spontaneous perineal laceration in the intervention group {92% versus 66% (p=0.04)}. There was no significant difference in the mean severity of pain at the time of entrance to the snoezelen room and the first and second hours; whereas, this difference was significant in the third hour (p=0.01). The mean length of the first stage (in hour) was significantly lower in the intervention than control group (8.4±0.7 versus 5.0±1.0, p=0.04). Moreover, there was no difference in the Apgar score of newborns (p=0.89) [38].
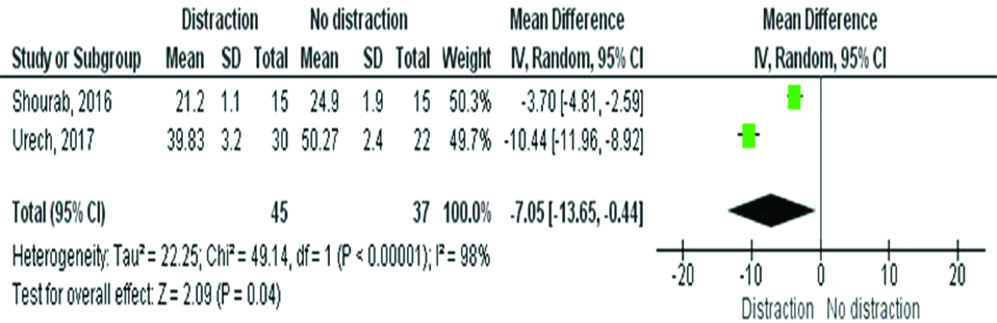
Moreover, the meta-analysis results showed that the mean score of anxiety in pregnant women and women in labour, who received distraction interventions, was significantly lower than the control{mean difference: -7.0; 95% Confidence Interval: -13.7 to -0.4; p=0.04} [Table/Fig-5].
Meta-analysis of the effect of distraction technique vs no distraction technique on maternal anxiety.
Discussion
The childbirth outcomes in clinical trials conducted by Shourab NJ et al., and Manesh MJ et al., were investigated as the outcome of distraction techniques [37,38]. Results showed that the distraction techniques had positive effect in reducing anxiety before, during, and after episiotomy repair, severity of delivery pain, length of labour, and frequency of episiotomy. Therefore, using these simple and low-cost techniques during pregnancy improves delivery outcomes and pregnancy experience of mothers.
In the studies by Locsin RG et al., and Manesh et al., the severity of pain was reported as an outcome [34,38]. Results showed that the distraction techniques can be used to reduce the intensity of pain during delivery and after the operation. These findings are consistent with results from McCarthy C study on the effect of distraction on severity of pain and anxiety during IUD placement [39]. Results of these two mentioned studies are consistent with the study of Aydin D et al., and Sadeghi T et al., [14,40].
The Berenson AB et al., study measured behavioural distress and anxiety in children as the outcome of intervention with distraction technique [35]. Results manifested the effectiveness of this technique in reducing anxiety caused from genital examination of prepubescent girls. This finding is consistent with Aydin D et al.’s and Lee J et al., studies [14,16]. Lee J et al., reported the effectiveness of distraction technique in reducing anxiety in children visiting for surgical operations. In a clinical trial, Salzmann S et al., showed that the distraction techniques reduced serum level of stress indicators, namely cortisol and alpha-amylase [41].
Anxiety of women with the risk of premature birth and women at labour has been investigated as the outcome of intervention in studies conducted by Urech C et al., and Shourab NJ et al., through distraction techniques [36,37]. Results showed that online games, as a distraction technique, did not significantly reduce anxiety in pregnant women, which is consistent with the results of McCarthy C’s study [39] and inconsistent with the findings of Shourab NJ et al.,’s study [37]. Although different distraction techniques have been used by these three studies, the participants in all of them were at childbearing age. These women are vulnerable sector of every society and thus the application of non-pharmacological and alternative medicine can guarantee the safety of mother and fetus. This contradiction in results highlights the need for further similar studies with more precise designs.
Although the five included studies in this systematic review are not homogeneous in terms of participants and distraction technique, they can be used at least for developing hypothesis and more homogeneous studies. To enrich the evidences, studies aiming at determining the effect of distraction techniques on severity of pain in women and men at different age groups should be designed and the results of consistent studies should be compared to obtain reliable results.
Limitation
Among the research limitations was that the study was limited to Farsi and English articles. Another limitation was low quality and high risk of bias of the included trials.
Conclusion
According to the results, distraction is a simple, low-cost, and accessible technique for reducing pain, anxiety, and stress in the field of gynaecology and midwifery. Moreover, given that there are scant studies into this field and their high risk of bias, it is recommended to use distraction techniques in different areas of clinical trials with higher quality.