Mott Cells: The Herculean Plasma cell
SV Sreelatha1, Vimal Kumar Karnaker2, Sanjana Nair3
1 Additional Professor, Department of Oral Pathology, A.B. Shetty Memorial Institute of Dental Sciences, NITTE (Deemed to be University), Mangalore, Karnataka, India.
2 Professor, Department of Microbiology, K.S. Hegde Medical Academy, NITTE (Deemed to be University), Mangalore, Karnataka, India.
3 Student, Srinivas Institute of Medical Sciences and Research Centre, Mangalore, Karnataka, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Vimal Kumar Karnaker, Professor, Department of Microbiology, K.S. Hegde Medical Academy, NITTE (Deemed to be University), Deralakatte, Mangalore-18, Karnataka, India.
E-mail: vimalkarnaker@yahoo.co.in
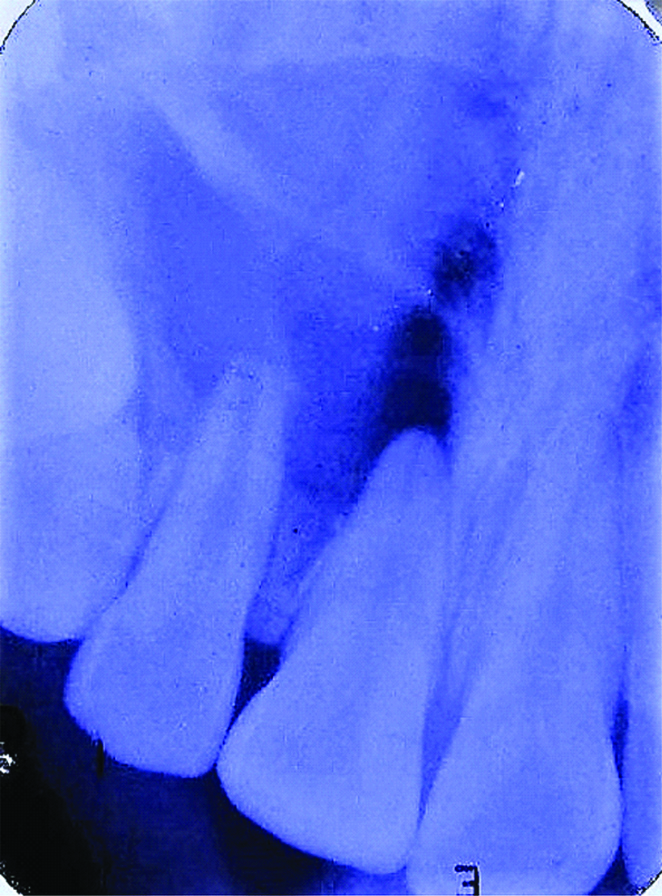
A 19-year-old female patient presented with a non-tender swelling in the right anterior maxillary region of one month duration. A history of trauma 10 years ago was reported in the same site which was uneventful. On intraoral examination the swelling was diffuse, well defined in relation to 11 and 12 region. On palpation the swelling was soft to firm in consistency, adherent to the overlying mucosa. Electric pulp testing of 11 and 12 showed no response. This indicated non-vital teeth. The lesion was provisionally diagnosed as Periapical cyst. Differential diagnosis of Periapical granuloma was given. Radiographic examination revealed an ovoid radiolucency in relation to the periapical region of 11 and 12. The lesion was well defined and extending from mesial of 11 to mesial of 13, measuring 1×1 cm [Table/Fig-1].
Periapical radiograph showing radiolucency in relation to the apical region of 11 and 12.
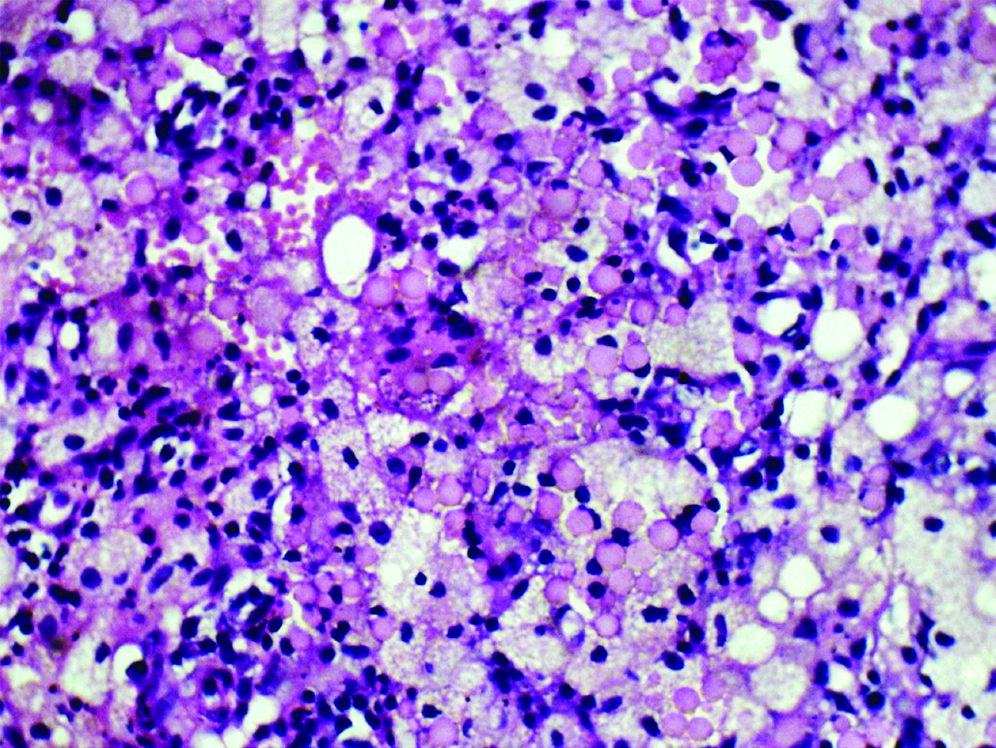
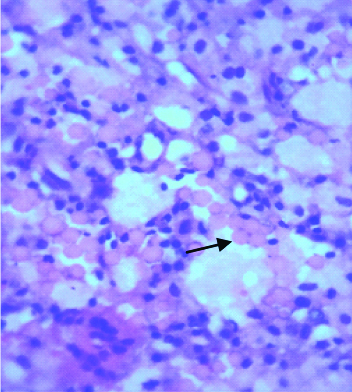
An excisional biopsy was performed after obtaining the patients written consent. Gross examination of the submitted soft tissue was of multiple bits, brownish black in colour with no lumen. Histopathological examination of Haematoxylin and eosin stained sections revealed dense chronic inflammatory infiltrate in the connective tissue stroma. The inflammatory cells were predominantly composed of foamy macrophages, multiple round to ovoid refractile bodies which were homogenous and eosinophilic resembling fused Russell bodies of varying sizes and number [Table/Fig-2], plasma cells and lymphocytes. In higher magnification 400X using H&E stain showed Russell bodies of varying number [Table/Fig-3], with eccentrically placed nucleus where seen arranged in clusters. On literature search, these cells were confirmed as “Mott cells.” On the basis of clinical, radiological and microscopic findings this case was diagnosed as Periapical granuloma of the immune type. On follow-up the healing was uneventful. The presence of these unique cells called Mott cells made us report this case.
Photomicrograph of H&E stained slide shows numerous Mott cells (fused Russell bodies) interspersed between plasma cells, foamy histiocytes and lymphocytes with extravasated RBCs in connective tissue stroma. (Original magnifications, 200X).
Photomicrograph of H&E stained section shows presence of Mott cells (clustered Russell bodies 3-5 in number) with eccentrically placed nucleus (Original magnification 400X).
Discussion
Periapical granulomas are of two types immune and non-immune granuloma. Immune granuloma consists of numerous plasma cells, lymphocytes and macrophages. Mott cells are Atypical Plasma cells with multiple aggregates of Russell bodies containing immunoglobulins. Mott cells were initially identified in the brains of monkeys with Trypanosomiasis by a surgeon, FW Mott. However, he called it as ‘Morular cell’ as ‘Morus’ means mulberry in Latin and is also believed to be of plasma cell origin, which are seen in chronic inflammation [1]. William Russell in 1890 was the first to describe these cells in the peripheral areas of malignant lesions, and thought that it was a fungus. However, he was unaware of its exact origin and nature. Thus, these cells were named after the surgeon FW Mott in 1901 [1,2].
Mott cell are accumulation of multiple Russell bodies containing immunoglobulins. One theory proposed for its formation is linked to the atypical plasma cells which are seen at the end stage of B-lymphocyte development which leads to increased synthesis of mutated immunoglobulin. The immunoglobulins synthesized are accumulated in the distorted endoplasmic reticulum which form large vesicles, which is neither secreted nor degraded resulting in grape-like appearance of these bizarre cells called Mott cell [3]. Another theory proposed for the Mott cell development is linked to the genetic locus-microsatellite marker D4 Mit70 and D4 Mit 48, which is in close proximity to the locus lmh-1 associated with hypergammaglobulinemia [4]. Mott cell formation has been observed in mice and rabbits as a result of antigenic stimulus and the nature of which is unexplainable. A study conducted by Cotter PF on peripheral blood examination obtained from poultry reported the presence of Mott cells and related their production to incompetent or an abnormal immune response or thought to be an indicator of stress [5]. Mott cell on H&E stained section is seen as multiple eosinophilic, homogeneous spherical inclusions of varying sizes which are accumulated Russell bodies within a single plasma cell having an eccentrically placed clock faced nucleus. Special stains like Periodic acid Schiff stain and May-Grunwald Giemsa (MGG) stain show positive reactions [1]. Immunohistochemistry markers (IHC) markers like B 220, CD 5, CD 43, CD 11b are found to be positive for Mott cells [6].
Mott cells have been reported in various conditions such as reactive lesions, neoplasm, and in some syndromes. Reactive lesions like Reactive Plasmacytosis and neoplasms like Large B-cell lymphoma, Burkitt’s lymphoma, Plasmablastic lymphoma, Multiple myeloma, and also in syndromes like Wiskott-Aldrich syndrome and Von-Recklinghausen neurofibromatosis [7]. Russell bodies were first reported in dental literature by Giardino L et al., in case of pulpitis [8]. Other cases like neurofibroma [6], periapical granuloma, osteomyelitis, lichen planus and radicular cyst [9] also showed the occurrence of these interesting cells. Its association with such lesions suggest its relationship to chronicity, aberrant immune response and also may indicate stress [9]. The presence of Mott cells in our case may be related to stress caused due to trauma or may suggest abnormal immune response which was the reason to call it as immune type of periapical granuloma. To unveil the significance of Mott cells in pathology more number of cases needs to be reported to demystify the facts behind these unique cells.
[1]. Bain BJ, Russell bodies and Mott cellsAm J Hematol 2009 84:51610.1002/ajh.2139719384941 [Google Scholar] [CrossRef] [PubMed]
[2]. Manasa Ravath CJ, Kulkarni N, Vinod R, Mott cells- at a glanceInternational Journal of Contemporary Medical Research 2017 4(1):43-44. [Google Scholar]
[3]. Valetti C, Grossi CE, Milstein C, Sitia R, Russell bodies: A general response of secretory cells to synthesis of a mutant immunoglobulin which can neither exit from, nor be degraded in, the endoplasmic reticulumJ Cell Biol 1991 115:983-94.10.1083/jcb.115.4.9831955467 [Google Scholar] [CrossRef] [PubMed]
[4]. Jiang Y, Hirose S, Hamano Y, Kodera S, Tsurui H, Abe M, Mapping of a gene for the increased susceptibility of B1 cells to Mott cell formation in murine autoimmune diseaseJ Immunol 1997 158:992-97. [Google Scholar]
[5]. Cotter PF, Are peripheral Mott cells an indication of tress or inefficient immunity?Poult Sci 2015 94:1433-38.10.3382/ps/pev05325725075 [Google Scholar] [CrossRef] [PubMed]
[6]. Bavle RM, Bizzare plasma cell- Mott cellJ Oral Maxillofac Pathol 2013 17:2-3.10.4103/0973-029X.11068223798821 [Google Scholar] [CrossRef] [PubMed]
[7]. Rampisela D, Donner LR, An unusual self-limited clonal Mott cell proliferation with lymphoplasmablastic lymphoma like features in child with Wiskott- Aldrich syndrome and von Recklinghausen’s neurofibromatosisPathol Res Pract 2010 206:467-71.10.1016/j.prp.2009.07.00319713050 [Google Scholar] [CrossRef] [PubMed]
[8]. Giardino L, Savoldi E, Pontieri F, Berutti E, Russell bodies in dental pulp of permanent human teethOral Surg Oral Med Oral Pathol Oral Radiol Endod 2004 98:760-64.10.1016/j.tripleo.2004.06.07315583553 [Google Scholar] [CrossRef] [PubMed]
[9]. Arora M, Desai K, Mane D, Multiple mott cells in periapical lesion of the oral cavityJ Coll Physicians Surg Pak 2017 27(6):373-75. [Google Scholar]