Unilateral Breast Abscess by an Extremely Drug Resistant Salmonella enterica serovar Typhi: First Case Report from Pakistan
Nadia Midhat Zehra1, Luqman Satti2, Faisal Hanif3, Saman Nadeem4
1 Resident, Department of Microbiology, Pakistan Navy Ship Shifa Hospital, Karachi, Pakistan.
2 Consultant, Department of Microbiology, Pakistan Navy Ship Shifa Hospital, Karachi, Pakistan.
3 Consultant, Department of Microbiology, Pakistan Navy Ship Shifa Hospital, Karachi, Pakistan.
4 Resident, Department of Microbiology, Pakistan Navy Ship Shifa Hospital, Karachi, Pakistan.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Luqman Satti, Consultant, Department of Microbiology, Pakistan Navy Ship Shifa Hospital, Karachi, Pakistan.
E-mail: luqmansatti@hotmail.com
Invasive salmonellosis caused by Salmonella typhi and Salmonella paratyphi is a serious life-threatening complication in immunocompromised patients. Since blood cultures have only 40-80% sensitivity, very limited diagnostic modalities are left. Here, authors present a case of a 24-year-old pregnant lady who develops a unilateral breast abscess harbouring Salmonella typhi. The isolate was Extremely Drug Resistant (XDR), that is resistant to first line drugs, ciprofloxacin and ceftriaxone. She was successfully treated with combination of injection meropenem and tablet azithromycin and continued for 14 days. To the best of authors knowledge, this was the first reported case of Salmonella enterica serovar Typhi in a pregnant lady from Pakistan.
Immunocompromised, Invasive salmonellosis, Typhoid fever
Case Report
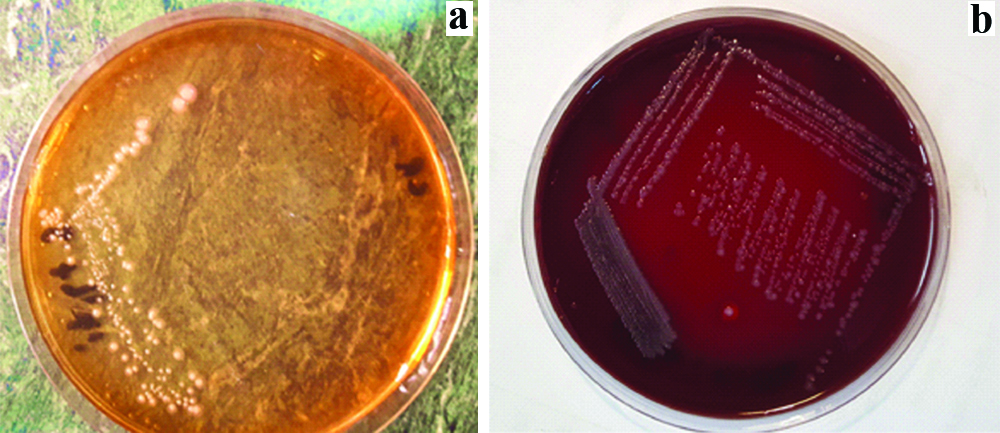
A 24-year-old female, 35th week of gestation, primigravida, presented in emergency department with two weeks history of fever off and on and malaise. She noticed left side breast pain and swelling for last two days. She remained admitted for few days at some local hospital and was given injection ceftriaxone but the symptoms did not improve. She was a housewife by profession and there was no past history of any admission and prolonged illness. At the time of presentation, her temperature was 102°F and blood pressure of 100/70 mmHg. Baseline investigations are mentioned in [Table/Fig-1]. Blood slide for malarial parasite and dengue NS1 serology was negative. Paired blood cultures were drawn and sent to microbiology laboratory. She was admitted in gynaecology ward and started with intravenous injection tazobactam-piperacillin 4.5 gram thrice daily. Ultrasound left breast swelling revealed localised abscess of around 5 mL. Abscess was drained and pus was sent for culture and sensitivity. Gram stain of the pus specimen showed numerous gram-negative bacilli. Specimen was inoculated on blood and MacConkey agar. Next day, growth of non-lactose fermenting, catalase positive and oxidase negative colonies were obtained on both the agars as shown in [Table/Fig-2]. Isolate was confirmed as Salmonella typhi on biochemical analysis and agglutination with specific antisera. The isolate was only sensitive to meropenem and azithromycin by disc diffusion antimicrobial susceptibility method. All the sensitivity results were confirmed by VITEK 2 (bioMerieux) system [Table/Fig-3]. The results were immediately informed to the primary physician.
Important blood chemistry parameters.
| Parameter | Result | Reference range |
|---|
| Total leucocyte count | 25.1×109/L | 4-10×109/L |
| Haemoglobin | 9.7 gm/L | 12-16 g/dL |
| Platelets | 229×109/L | 150-400×109/L |
| Neutrophils | 85% | 40-80% |
| Blood sugar random | 96 mg/dL | 80-160 mg/dL |
| C-reactive protein | 70 mg/L | Less than 6 mg/L |
| Urea | 4.6 μmol/L | 2.9-8.2 μmol/L |
| Creatinine | 41 μmol/L | 62-124 μmol/L |
| Serum bilirubin | 16 μmol/L | 1.7-20 μmol/L |
| Serum albumin | 44 g/dL | 35-50 g/dL |
Colonies of Salmonella typhi on: a). MacConkey agar and b). blood agar plate
MICs of Salmonella typhi on Vitec 2 system.
| Antibiotic | MIC | Interpretation |
|---|
| Ampicillin | ≥32 | R |
| Trimethoprim/ sulfamethoxazole | ≥320 | R |
| Ciprofloxacin | ≥4 | R |
| Ceftriaxone | ≥64 | R |
| Cefipime | ≥64 | R |
| Meropenem | ≤0.25 | S |
MIC=Minimum inhibitory concentration, R=Resistant, S=Sensitive
On the evening of admission, patient experienced decreased fetal movements. An urgent Cardiotocography (CTG) confirmed fetal distress. Patient underwent an urgent lower abdominal caesarian section. She developed respiratory distress post-operative and shifted to intensive care unit. X-ray chest showed bilateral patchy consolidation in lower lobes. A Computed Tomography (CT) pulmonary angiogram of lungs showed bilateral pleural effusion with basal atelectasis. Pleural tap was done and 10 mL of straw coloured fluid was sent for routine examination and culture. Initial antibiotic therapy was changed from Injection tazobactam-piperacillin to intravenous injection meropenem one gram thrice daily and tablet azithromycin 500 mg twice daily. Patient showed clinical and radiological improvement with this regimen and became afebrile on the 3rd day of treatment. She was shifted toward on 4th day of new regimen and later on discharged on 7th day. She was advised to continue the treatment for 14 days with regular follow-up. Her blood cultures and pleural fluid cultures did not show any growth after recommended period of incubation.
Discussion
Salmonella species belong to group Enterobacteriaceae and can cause gastroenteritis, septicaemia, focal diseases and enteric fever in humans. The pathogenesis of extra-intestinal complications of typhoid fever depends on the bacterial load, the virulence of the strain, host’s immunity, treatment failure and previous exposure [1]. Extremes of age, immunosuppression, underlying malignancy, intravenous drug abuse and previous trauma have been identified as risk factors for focal Salmonella infections [2].
Most common sites of focal salmonella infections are intra-abdominal, osteoarticular and urinary tract. Isolated soft tissue Salmonellosis is a rare finding and is reported in only 6-10% of cases [3]. After an episode of acute gastrointestinal illness, organism can persist in distal sites as gall bladder, bones and urinary tract. Remote abscesses are the result of haematogenous or lymphatic dissemination of primary gastrointestinal infections [4]. Focal abscess as the complication of invasive salmonellosis in different body parts is mostly reported in immunocompromised patients [5].
The incidence of breast abscess in typhoid fever is <30 cases as reported in literature [6]. The first report of Salmonella typhi in breast abscess was by Thayer WS and Hazen HH in 1907 [7]. In a study by Kataria K et al., salmonella infections causing an abscess in lactating breast has been stated as one of major causes of breast abscess in areas where typhoid fever is endemic [8]. Gali JH et al., has reported breast abscess in a young, non-lactating diabetic female [9]. Murugesan N et al., reports a 60-year diabetic female with unilateral breast abscess [10]. In the present case, the patient had symptoms of typhoid fever but the blood cultures were negative. In all reported cases patients developed a pattern of fever and other symptoms consistent with typhoid and blood cultures were negative for Salmonella. Most likely possibility could be that the isolate got settled in breast in the bacteremic phase of the disease. Due to weak immune response in pregnancy, the organisms got activated and initiated an infection leading to abscess. Salmonella breast abscess can occur in diabetic patients due to poor immune response [11,12].
Most of the cases of breast abscesses are due to Salmonella typhi strain. Disseminated focal abscess has been a complication of Salmonella enterica serovars Paratyphi and S. typhimurium. All the reported patients were immunocompetent females. Siddesh G and Sumana MN reports breast abscess by Salmonella paratyphi in a febrile young female [13]. Baran I et al., reports a unilateral breast abscess by Salmonella typhimurium in a middle-aged female with rheumatoid arthritis [14]. All these affected females were non-lactating and non-pregnant. In the present case, the patient was in 35th week of gestation.
In recent years, the incidence of Extensively Drug-Resistant (XDR) Salmonellatyphi is on the rise especially in Sindh province of Pakistan. Since 2016, more than 300 XDR cases of typhoid cases have been reported in this province [15]. By definition, the XDR Salmonellatyphi is resistant to ampicillin, trimethoprim-sulfamethoxazole, fluoroquinolones, and third generation cephalosporin [15]. Recent research has shown that these XDR isolates carry a plasmid, which encodes additional resistance including extended-spectrum β-lactamase, qnrS fluoroquinolone resistance gene and the blaCTX-M-15 [15]. In the present case, patient was given injection ceftriaxone at some local hospital but she did not show improvement. The present case report is unique as Salmonella strain was XDR and was only sensitive to meropenem and azithromycin. Meropenem and azithromycin are the last line of therapy for such cases.
Conclusion
The present case report concludes that breast abscess in a non-lactating pregnant female with history of prolonging fever must be evaluated, keeping the possibility of a Salmonella breast abscess in mind. Since typhoid is endemic in Pakistan and cases of XDR typhoid is increasingly being reported from Karachi and Hyderabad, there should be a high suspicion of XDR Salmonella in such areas. Despite limited treatment options, a combination of medical and surgical management helps in such a case when supported by a microbiological culture and sensitivity report.
MIC=Minimum inhibitory concentration, R=Resistant, S=Sensitive
[1]. Chen PL, Chang CM, Wu CJ, Ko NY, Lee NY, Lee HC, Extra intestinal focal infections in adults with nontyphoid Salmonella bacteremia: predisposing factors and clinical outcomeJ Intern Med 2007 261(1):91-100.10.1111/j.1365-2796.2006.01748.x17222172 [Google Scholar] [CrossRef] [PubMed]
[2]. Brncic N, Grorup L, Breast Abscess in a Man Due to Salmonella enterica Serotype EnteritidisJ Clin Microbiol 2012 50(1):192-93.10.1128/JCM.05361-1122031702 [Google Scholar] [CrossRef] [PubMed]
[3]. Hsu CC, Chen WJ, Chen SY, Chiang WC, Hsueh PR, Fatal septicemia and pyomyositis caused by Salmonella typhiClin Infect Dis 2004 39(10):1547-49.10.1086/42513815546098 [Google Scholar] [CrossRef] [PubMed]
[4]. Sudhaharan S, Padmaja K, Solanki R, Lakshmi V, Umabala P, Aparna B, Extra intestinal Salmonellosis in a tertiary care center in South IndiaJ Infect Dev Ctries 2014 8(7):831-7.10.3855/jidc.373125022292 [Google Scholar] [CrossRef] [PubMed]
[5]. Chiao HY, Wang CY, Wang CH, Salmonella abscess of the anterior chest wall in a patient with type 2 diabetes and poor glycemic control: a case reportOstomy Wound Manage 2016 62(3):46-9. [Google Scholar]
[6]. Smita S, Breast Abscess by Salmonellaparatyphi: a case report and literature reviewJ Clin Diagn Res 2015 9(9):03-04. [Google Scholar]
[7]. Thayer WS, Hazen HH, Calcification of the breast following a typhoid abscessExp Med 1907 9(1):1-17.10.1084/jem.9.1.119867070 [Google Scholar] [CrossRef] [PubMed]
[8]. Kataria K, Srivastava A, Dhar A, Management of lactational mastitis and breast abscesses: review of current knowledge and practiceIndian J Surg 2013 75(6):430-5.10.1007/s12262-012-0776-124465097 [Google Scholar] [CrossRef] [PubMed]
[9]. Gali JH, Firdous S, Narreddy S, Rao R, Recurrent Salmonella typhi chest wall abscesses in a diabetic ladyJ of Evolution of Medical and Dental Sciences 2014 3(46):11279-82. [Google Scholar]
[10]. Murugesan N, Alagar SR, Viswanathan MS, Anbazhagan A, A rare case of breast abscess due to Salmonella typhiIJCRR 2016 8(5):10-12. [Google Scholar]
[11]. Singh S, Pandya Y, Rathod J, Trivedi S, Bilateral breast abscess: a rare complication of enteric feverInd J Med Microbiol 2009 27:69-70. [Google Scholar]
[12]. Kumar ES, Selvam EM, Ramesh SS, Salmonella enterica serovar typhi in breast abscess: A case reportInd J Pathol Microbiol 2012 55(4):608-9.10.4103/0377-4929.10785723455830 [Google Scholar] [CrossRef] [PubMed]
[13]. Siddesh G, Sumana M N, A case of breast abscess due to Salmonella paratyphi AInt J Health Allied Sci 2012 1:109-11.10.4103/2278-344X.101712 [Google Scholar] [CrossRef]
[14]. Baran I, Aksu N, Aksoy A, Breast abscess due to Salmonella typhimurium in a patient with rheumatoid arthritis: a case reportBMC Infect Dis 2016 16:348-9.10.1186/s12879-016-1659-z27448659 [Google Scholar] [CrossRef] [PubMed]
[15]. Klemm EJ, Shakoor S, Page AJ, Qamar FN, Judge K, Saeed DK, Wong VK, Emergence of an extensively drug-resistant Salmonella enterica serovar typhi clone harboring a promiscuous plasmid encoding resistance to fluoroquinolones and third-generation cephalosporinsMbio 2018 9(1):pii:e00105-18.10.1128/mBio.00105-1829463654 [Google Scholar] [CrossRef] [PubMed]