Among the abdominal organs, the spleen and the liver are the most commonly injured abdominal organs. The kidneys are protected by the lower thoracic cage and the strong back muscles, and are less prone to external physical trauma [1,2]. Common modes of injury for renal trauma include Road Traffic Accidents (RTA), railway accidents, fall from a height or stab injuries [3,4]. Renal injury is seen in about 1-5% of all trauma cases. Most of these (80-95%) are a result of blunt trauma [2,4-6], whereas penetrating trauma accounts for 20% of the cases [7,8].
The application of conservative management for trauma to other solid organs like the liver and spleen has shown success and this has been applied to renal trauma much more than it was earlier. With the current advances in intensive care protocols, conservative management is successful in a large proportion of renal trauma patients who are haemodynamically stable [9]. Patients who continue to remain haemodynamically unstable need operative management and this usually leads to a nephrectomy, unless the patient is being managed in a specialised trauma centre where a renal preservation procedure like a renorraphy or renal vascular repair may be performed [9-11]. A specialised centre may also offer facilities of angioembolisation to control renal bleeding following trauma [12].
Watchful conservative management in high grade renal trauma can lower the rate of nephrectomy with no increased morbidity or mortality [4]. Consequently, there is consensus that conservative non operative management of renal trauma is safe in most patients who have a severe grade of renal injury but are haemodynamically stable [13-15].
In spite of the current trends towards conservative management of renal trauma, there still remains a dilemma in patients with grade IV renal trauma (as per the grading of renal trauma on computed tomography by the American Association of Surgery for Trauma, AAST) [16].
There are many scoring systems to assess the severity of trauma like anatomical, physiological and mixed scoring system. Anatomical trauma scoring systems are the ISS and Mangled Extremity Severity Score (MESS); physiological trauma scoring system includes the Glasgow Coma Scale (GCS) and Revised Trauma Score (RTS). Out of these, ISS is the only anatomical scoring system, is easy to calculate and it has been proven as an excellent predictor for mortality in trauma patients [17-21].
The ISS was first described in 1974 as a method of classifying patients with multiple injuries and stratifying them into severity grades [22]. It has been validated to correlate with mortality and morbidity following trauma [23]. The ISS is based on the Abbreviated Injury Scale (AIS) which is an anatomic scale and describes severity of individual injuries The ISS in turn, combines the three most severe AIS scores in a patient with polytrauma and gives a score which provides a complete picture of the severity of polytrauma and can then be used clinically to prognosticate patients. The aim of this retrospective study was to find correlation between Injury Severity Score and the decision regarding the management in patients with severe renal trauma.
Materials and Methods
We conducted a retrospective study evaluating the medical records of all renal trauma patients admitted in Lokmanya Tilak Municipal General Hospital, Mumbai, India, a tertiary trauma care setup, from January 2013 to December 2016. Patients with polytrauma including renal trauma but without any other visceral organ injury were included. These patients could have injuries to other body regions like head, face, neck, thorax, spine and extremities. Patients with other abdominal visceral injury (liver, spleen, mesenteric tear) were excluded. This was done so that the renal injury would be the sole contributing factor in calculating the AIS for the abdomen. All patients were managed by resuscitation according to ATLS (Advanced Trauma Life Support) guidelines for trauma [24]. Haemodynamic parameters of the patients were noted. Blood investigations were performed including complete haemogram, liver and renal function tests, serum electrolytes, prothrombin time and blood grouping. All patients were catheterised and observed for gross or microscopic haematuria in the first catheterised sample of urine.
After primary resuscitation, the AIS for each component injury of the polytrauma, and the ISS were calculated [22,25].
Subsequently, a bedside Focused Assessment with Ultrasonography for Trauma (FAST) was carried out in all patients. All patients with suspected renal injuries, as a component of their polytrauma, were investigated by a Contrast Enhanced Computed Tomography (CECT) after confirming a normal serum creatinine report. Haemodynamic parameters, blood investigations and the CECT findings were considered together guiding patient management.
All renal traumas were graded as per their American Association for Surgery of Trauma (AAST) renal injury scale [16]. Grades 1, 2 and 3 renal injuries were managed conservatively. It included strict bed rest, strict monitoring of patient parameters like pulse rate, blood pressure, respiratory rate, abdominal girth, fluid intake, urine output and central venous pressure. Serial haemoglobin and haematocrit monitoring (every 12 hours) were done.
Haemodynamically stable patients with grade 4 renal injuries underwent minimally interventional management in the form of Double J (DJ) stenting when contrast extravasation was seen on CT urography while unstable patients required invasive treatment in the form of exploratory laparotomy followed by renorraphy or nephrectomy. Pig tailing was done along with DJ stenting in patients presenting with grade 4 renal injury with a large perinephric collection. Grade 5 renal injury patients were managed with emergency exploratory laparotomy.
Patients with a DJ stent were followed up after 6 weeks. A retrograde pyelography was performed at the time of stent removal to check for any extravasation from the pelvicalyceal system. Patients who required pigtail catheter for perinephric collection were reviewed with a local ultrasonography after 10 days to confirm complete drainage of the collection following which the pigtail catheter was removed.
For patients who required exploratory laparotomy, an abdominal drain was removed once the drain output was less than 50 mL over 24 hours. For patients who had undergone renorraphy, the Foley’s catheter was removed after 3 days and the drain was observed for any increase in output for 24 hours and then removed.
We grouped the patients as follows: Group A-Conservative Management; Group B Minimally invasive management; and Group C-Surgical management. We also correlated the ISS of the patients with their type of management, especially those with high grade renal trauma. Patients were followed up at 6 weeks with an ultrasound of the abdomen, serum creatinine and blood pressure measurement and then at 3 months with serum creatinine and measurement of blood pressure.
Statistical Analysis
Data was analysed using the XLSTAT software (Addinsoft, New York, USA) in Microsoft Excel. Mann-Whitney U test was used in univariate analysis. p<0.05 was considered statistically significant.
Results
A total of 38 patients were studied of which 30 were males and 8 females (ratio 3.75:1). The mean age was 29 years (range 10 to 55 years). Six (15.78%) were paediatric patients (Age <12 years). Thirty four patients (89.4%) had blunt trauma (25 from a RTA and 9 following fall from a height) while 4 (10.6%) patients had stab injuries. Mean time to present to the emergency room was 4.6 hours.
Mean systolic blood pressure was 108.6±20.16 mm Hg and the mean heart rate was 98.7±13.03 beats per minute. Seven (18.42%) patients presented with hypotension (systolic BP <100 mm Hg). Twenty eight (73.6%) of the patients had gross haematuria. Four out of remaining 10 patients had microscopic haematuria. Mean haemoglobin among the patients was 10.49±1.74 gm% with 44.7% patients having haemoglobin less than 10 gm/dL. All patients had normal serum creatinine at presentation. Sensitivity of FAST in detecting renal injury was 84.2%. While 58% of the patients had renal injury on the right side, 40% had it on the left. One patient had bilateral renal arterial thrombus. Severity of renal trauma as graded by CECT is shown in [Table/Fig-1] while [Table/Fig-2] summarises the AAST grade and ISS in the three management groups.
AAST grade of patients with their management and mean ISS.
| AAST grade | Number of patients | Management | ISS (mean±2 SD)* |
|---|
| 1 | 9 | Conservative | 13.77±11.10 |
| 2 | 11 | Conservative | 10.72±12.18 |
| 3 | 3 | Conservative | 14±7.2 |
| 4 | 75 | Minimally InvasiveSurgical Exploration | 9.85±3.26**17.80±5.54 |
| 5 | 3 | Surgical Exploration | 21±6.42 |
*ISS: Injury severity score, **(p=0.007), Mann-Whitney U test
ISS and AAST grades of renal injury in different management Groups.
| Management group | Number of patients (percentage) | Mean ISS | AAST grades of renal Injury (percentage out of total patients in specific management group) |
|---|
| A- Conservative | 23 (60.5%) | 12.3 | 1 (39.1%)2 (47.8%)3 (13%) |
| B- Minimally interventional management | 7 (18.4%) | 11 | 4 (100%) |
| C- Surgical Exploration (total)NephrectomyRenorrhaphy | 8 (21.8%)5 (13.5%)3 (7.89%) | 19.371920 | 4 (60%), 5 (40%)4 (66.6%), 5 (33.3%) |
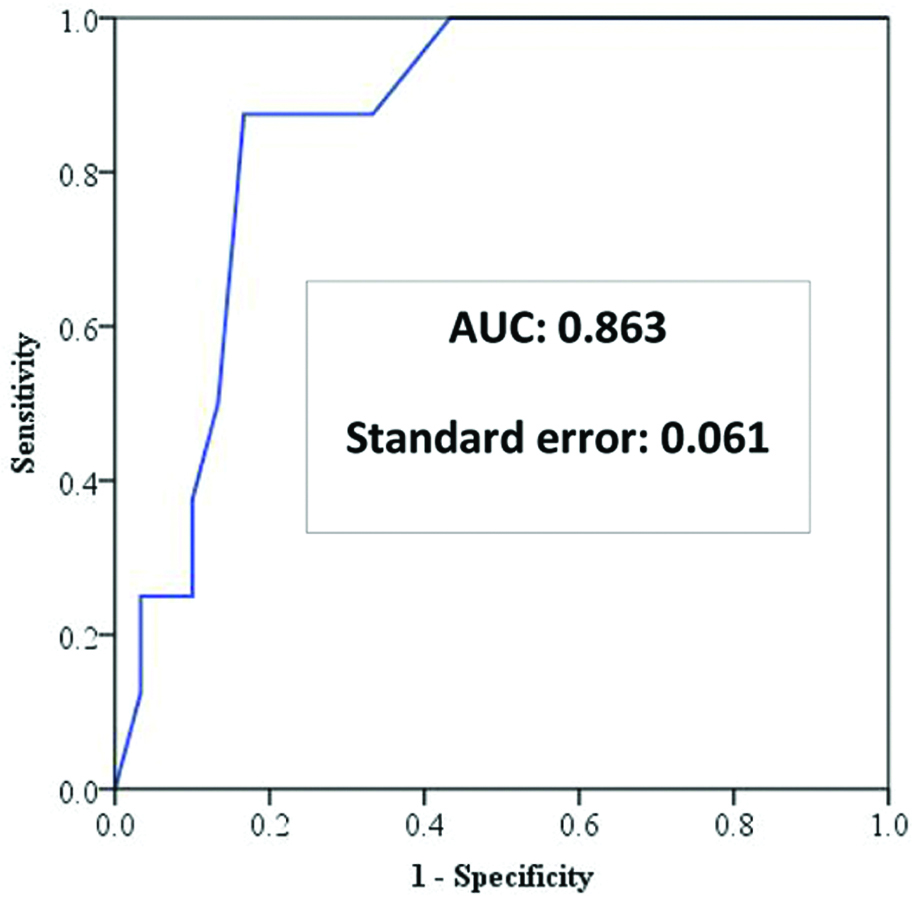
The ISS (mean±2SD) in the 3 treatment groups were 12.3±11.42, 11±3.26 and 19.3±8.94 respectively. Group C had significantly higher ISS than A (p=0.005) and B (p=0.0002). Of the grade 4 injuries, those who required surgical exploration had a higher ISS (17.80) compared to those who could be managed with minimal intervention (9.85); and this difference was statistically significant (p=0.007). Of all grade 4 injuries, 7 were stented, while 5 underwent surgical exploration. Of the grade 5 injuries, two required nephrectomy and one underwent revascularisation with renorrhaphy. One of the 8 patients that underwent surgery died. This patient had a grade 5 renal injury and approximately 2.5 to 3 litres of haemoperitoneum was found intraoperatively. This patient had an ISS of 25. Receiver Operating Characteristic (ROC) curve analysis show high accuracy of ISS in predicting the need for surgical exploration in high grade renal trauma with Area Underthe Curve (AUC) of 0.863 with a standard error of 0.061. An ISS of 15 or more can predict the need for surgical exploration in high grade renal trauma with a sensitivity of 87.5% and a specificity of 83.3% [Table/Fig-3].
Receiver Operating Characteristic (ROC) curve analysis for predictive value of ISS for surgical exploration in renal trauma.
Follow-up data was available for 35 of the 38 patients. Median follow-up period was 8.5 months. Only one patient required repeat DJ stenting in view of minimal contrast leak at ureteropelvic junction during a retrograde pyelogram done 6 weeks after the trauma. On repeat retrograde pyelography after 4 weeks, there was no contrast leak and the stent was removed. No patient was found to be hypertensive in the follow-up.
Discussion
The AIS is an internationally accepted and validated injury scoring system that assigns a score to an injury by body region according to its severity on a 6 point scale. Thus, the AIS gives a score to each injury in a patient with polytrauma. The ISS is based on the AIS and is a global score taking into account the most serious injuries in a patient with polytrauma. The AIS injuries are ranked on a scale of 1 to 6 as minor 1, moderate 2, serious 3, severe 4, critical 5 and unsurvivable 6 [26].
The ISS calculates a global score for patients with polytrauma. Each injury is given an AIS score and is classified into one of the six body regions (head, face, chest, abdomen, extremities with pelvis, external). Then, the highest AIS score in each body region is selected. ISS is calculated by squaring and adding the 3 most severely injured body regions [22,23]. For example, let us consider a patient with polytrauma with AIS of 2 for the head, 1 for the face, 1 for the chest, 3 for the abdomen, 2 for the pelvis and 1 for the external injuries. Here, the highest 3 AIS scores are 3, 2 and 2. Thus the ISS would be 32+22+22=17.
Major trauma has been defined as an ISS value more than 15 based on the 1998 edition of AIS [27]. However, with the 2008 update in AIS, there has been suggestion to use an ISS cut-off of 12 to define major trauma [28].
In our study, we had divided our patients into three groups retrospectively. Group A included patients managed conservatively without any invasive procedure; Group B included patients managed conservatively but required a less invasive procedure like DJ stenting and pigtailing. Patients requiring exploratory laparotomy were included in Group C. Patients in Group C were found to have a significantly higher ISS as compared to those in Groups A and B. Also, amongst the patients with grade 4 renal injury, those who required surgical exploration had a significantly higher ISS as compared to those who could be managed with minimally invasive treatment.
A study conducted on patients with liver trauma in South Africa over 7 years from 1998 to 2004 concluded that the ISS is one of the predictors of the outcome in surgically treated patients liver trauma [22].
After clinical evaluation, imaging modalities like ultrasonography, CECT or MRI are required to detect asses and grade the severity of trauma to internal organs. Sensitivity of ultrasonography is less for the solid organs injuries. Only 35% of isolated renal injuries with abdominal free fluid are detectable on ultrasonography [29,30]. CECT of the abdomen is the most important investigation that helps to evaluate the entire urinary system including renal vascularity and the collecting system [31]. In trauma patients with suspected renal injuries, renal enhancement phase is evaluated to look for any areas of renal infarct. The late excretory phase should be evaluated in selective cases where the laceration is deep to check for any urinary extravasation [32,33]. Section thickness of 2.5 to 5 mm is sufficient for evaluation of the renal parenchyma but for renal vasculature evaluation, CT section thickness should be 0.5 to 1.25 mm [32].
None of our patients had a raised serum creatinine level on presentation. There may arise a dilemma to proceed with a CECT of the abdomen when a patient presents with a raised serum creatinine level. Tremblay LN et al., studied 56 patients with raised serum creatinine (>1.3) who underwent a CECT for trauma; only two of these patients had a transient rise in serum creatinine following the CECT [34]. Similarly, Kulvatunyao N et al., in their study of 543 trauma patients noted that the incidence of contrast induced nephropathy in trauma patients is low and their clinical course is benign [35].
American Association for the Surgery of Trauma (AAST) classification system is most commonly used to grade renal injuries on CECT [16].
In renal trauma, conservative management for grade 1 and 2 renal injuries is the norm. There are different opinions regarding grade 3 and 4 renal injury management. Most of the grade 3 and 4 renal injuries have been managed conservatively. However, grade 5 renal parenchymal injuries have also been managed by non-operative management but vascular grade 5 renal injuries should be managed with nephrectomy [36,37]. Success rate of non-operative management for renal trauma is about 82 % [36–39].
There are different surgical options in grade 4 and 5 renal injuries like total nephrectomy, partial nephrectomy, renorraphy, primary vascular repair and renal revascularization. There is a 64% chance of nephrectomy in open renal exploration in trauma cases. In cases where nephrectomy can be avoided after surgical exploration, only 25% renal function is preserved in affected kidney after open surgical repair in high grade renal trauma cases. Hence conservative treatment trial must be considered before opting for open surgical repair in high grade renal trauma patients except in those patients who are found to have a vascular injury on CECT [40]. Also, renal angiography with subsequent selective angioembolisation is another modality of managing patients with grade 3-4 renal trauma who are haemodynamically stable but have persistent haematuria despite conservative measures. It has a 90% success rate and can be used again in patients who fail one attempt at embolization [12,41,42].
Patients with high grade renal injuries who are haemodynamically stable can be managed conservatively. Some factors that may predict failure of conservative management in renal trauma include renal trauma secondary to motor vehicular accidents, hypotension at presentation, associated injuries to other organs, grade 5 injury, presence of a medial laceration, perinephric haematoma size more than 3.5 cm and vascular extravasation are significantly associated with failure of non-operative management in blunt renal trauma [43].
Renal trauma patients with lower ISS score could be considered for conservative or minimally invasive management. But for patients with grade 4 we could predict the need for surgical exploration. We hypothesise that a patient with grade 4 renal injury and a higher ISS, and hence with more severe polytrauma compared to one with grade 4 renal injury but a lower ISS, would not have the reserve to respond to conservative management and hence would benefit from surgical intervention. To our knowledge, this is the first study evaluating the role of ISS in predicting the need for surgical management in patients with high grade renal trauma.
Limitation
Our study was retrospective but on the basis of this experience, the Injury Severity Score can be considered as a good predictor for the requirement of surgical exploration in renal injury cases; specifically, in grade 4 injuries. To validate the Injury Severity Score as a strong predictor for the requirement of surgical exploration in renal trauma, further prospective studies with a larger pool of patients are required.
Conclusion
Higher ISS can guide clinical decision making when faced with a dilemma of conservative vs surgical management for high grades of renal trauma. Grade 4 injuries with a lower ISS can be managed without surgical exploration. Conservative management leads to preserved renal function in the patients and also decreased morbidity.
*ISS: Injury severity score, **(p=0.007), Mann-Whitney U test