Effectiveness of Cervical Stabilisation Exercises on Respiratory Strength in Chronic Neck Pain Patients with Forward Head Posture- A Pilot Study
Sonia Pawaria1, Dharmpal Singh Sudhan2, Sheetal Kalra3
1 Assistant Professor, Department of Physiotherapy, SGT University, Gurugram, Haryana, India.
2 Professor, Department of Pulmonary Medicine, SGT University, Gurugram, Haryana, India.
3 Professor, Department of Physiotherapy, SGT University, Gurugram, Haryana, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Dr. Sonia Pawaria, Budhera, Gurugram-122505, Haryana, India.
E-mail: sonia@sgtuniversity.org
Introduction
Forward Head Posture (FHP) is one of the most common abnormalities associated with chronic neck pain. In FHP the altered rib cage mechanics leads to decrease in thoraco-abdominal mobility, impaired diaphragm muscle mobility and reduced the ventilator efficacy of diaphragm, reduced the effectiveness of abdominals and intercostals muscles.
Aim
To examine the efficacy of Cervical Stabilisation Exercises on neck pain, neck disability, craniovertebral angle and respiratory muscles strength.
Materials and Methods
This pilot study was conducted on a total number of 20 subjects, which were further divided into study and control groups. Study group received Cervical Stabilisation Exercise with the conventional Physiotherapy. Control group received only Conventional Physiotherapy for six weeks. The baseline measurement was taken on day one of the study for Numeric Pain Rating Scale (NRPS) and Neck Disability Index (NDI). The Forward head posture which was assessed by the digital camera, measured the Cranio Vertebral Angle (CVA). Respiratory muscle strengths (MIP and MEP) were assessed by respiratory pressure meter. All measurements were repeated at the end of sixth week. The baseline measurement and measurement at the end of sixth week were compared by using the analysis of variance.
Results
Significant increase in CVA (from mean value of 37.90 to 59.21) and respiratory strength (PImax from mean value of 65.33 to 75.01, PEmax from mean value of 77.78 to 87.89) with decrease in NPRS (from mean value of 7.6 to 0.90) and NDI (from mean value of 12.11 to 0.60) scores were found in the group that received cervical stabilisation exercises as compared to control group (p<0.05).
Conclusion
Cervical stabilisation exercise is an effective approach to reduce the forward head posture and thus helps to regain the respiratory muscle strength by improving the biomechanics of respiratory muscles.
Craniovertebral angle, Maximal inspiratory pressure, Maximal expiratory pressure, Posture correction exercises
Introduction
Chronic neck pain is one of the most frequent musculoskeletal complaints. It is estimated that 70%-80% of people suffer from neck pain at some time in their lives and up to 60% of the population may experience persistent and recurrent pain. For the largest part of the previous century neck pain was of secondary interest in relation to low back pain [1]. However, the increasing incidence of neck pain during this century, which can be justified by changes in work nature, increased use of motor vehicles and the advancement and increased use of computers, has led the last 20 years to a continuously growing interest and research regarding the clear understanding of causes, manifestations and management of neck pain.
It has been commonly observed that patients who report with chronic pain in their neck often have associated forward head posture [2]. A FHP also known as “hunched upper back “is defined as anterior slanting of the neck over head in which the lower cervical spine goes into hyper flexion and the upper cervical spine into hyper extension associated with forwarding shoulders and rounded upper back [3]. The overload on the cervical spine resulting in fatigue of the neck muscles causes pain, stiffness and other symptoms in the neck [2].
It has been found that patients with FHP presented with weakness in the scapular retractors (rhomboids, serratus anterior and middle and lower trapezius) and shortening or tightening of the cervical extensors or the pectoralis muscles [4].
Chronic neck pain is a musculoskeletal condition affecting many people. Chronic neck pain has been found to be associated with decreased hand grip strength [5]. Although patients with neck pain are managed predominantly as musculoskeletal patients, weakness and fatigue of cervical muscles, reduced cervical mobility, impaired proprioception, postural abnormalities, and psychological compromise have been argued to be factors that are associated with poor pulmonary functions [6].
This forward head posture will lead to disorganisation of the muscle blocks, impairing diaphragm muscle mobility and, consequently, diaphragmatic function. This postural change also leads to accessory muscle recruitment, with increased sternocleidomastoid muscle activity, causing rib cage elevation, reducing thoraco-abdominal mobility, and compromising the ventilatory efficacy of the diaphragm. The faulty mechanics associated with FHP results into weakness of inspiratory muscles, poor respiratory strength, reduced chest expansion and hence increased work of breathing. This eventually results in impaired pulmonary functions such as reduced vital capacity, maximum inspiratory and expiratory pressures [7].
To correct misalignment towards an ideal posture using a combination of strengthening, stretching, and behavioural/bio-feedback training represent a significant component of the physical therapy intervention provided to clients with painful neck and/or thoracic musculoskeletal conditions. Improvement in postural alignment secondary to exercise would be expected due to improvement in muscle length and/or strength [8].
An exercise program for FHP guided by strengthening and stretching principles that address underlying soft tissue imbalances would include deep cervical flexor and shoulder retractor strengthening and cervical extensor and pectoral muscle stretching. The therapeutic approach of strengthening weakened postural muscles and stretching shortened ones to improve postural alignment has been advocated [9].
Researchers have reported that neck stabilisation exercises should be incorporated in the rehabilitation of the patients with chronic neck pain as the exercises improve strength, endurance and coordination of spinal stabiliser muscles and hence are helpful in reducing neck pain and enhancing cervical functions [10]. Nam CW et al., studied the effectiveness of cervical stabilisation exercises and breathing training on respiratory functions in stroke patients. They found that the patient with cervical stabilisation exercises in adjunct with breathing retraining showed greater improvement in respiratory functions [11]. Although similar study exists in literature which was done on stroke patients, but due to different mechanism of alteration of pulmonary function in stroke patients and patients with forwarding head posture this study is different from the previous studies. Hence, the current study was done to observe the effectiveness of cervical stabilisation exercises along with conventional physiotherapy treatment on the strength of respiratory muscles in chronic neck pain patients with forwarding head posture.
Materials and Methods
This pilot study was carried out at SGT Hospital Gurugram. The study was approved by the Ethical Research Committee, Ref. No. SGTU/ FMHS/D./96
Twenty subjects with chronic neck pain with mild neck disability (NDI score 5-15) who had poor performance (unable to achieve 24 mmHg of pressure) on Craniocervical flexion test were included in the study [12].
Subjects who were excluded from the study were those who reported of neck pain secondary to trauma, abnormalities/deformities of thoracic region or vertebral column, previous history of any thoracic or vertebral column surgery, subjects in the category of overweight as measured by BMI >30 and history of smoking.
Subjects who fulfilled the inclusion and exclusion criteria were divided into two groups by simple random allocation method i.e., Group A included 10 subjects received the conventional physiotherapy and Group B included 10 subjects who received the Cervical stabilisation exercise with the conventional physiotherapy. All the subjects underwent baseline assessment for neck pain (Numeric Pain Rating Scale), Disability (NDI), Respiratory Muscle Strength (PImax and PEmax with respiratory pressure meter and forward head posture by measuring the Craniovertebral angle [12,13]. Whole procedure of treatment program was explained to the subjects and written informed consent was taken from all of them.
Procedure
Subjects in Group A received the conventional physiotherapy treatment for six weeks which included cervical isometric exercises, Transcutaneous Electrical Nerve Stimulation (TENS) and hot pack. TENS was given at a frequency of 80 Hz with 10-30 mA intensity for 30 minutes. Cervical isometric exercises were performed in the sitting position by resisting at the forehead (cervical flexion, extension, rotation and side bending) for 10 seconds with 15 seconds breaks between holds with 10-15 repetitions in a progressive manner [10].
Subjects in Group B received the Cervical Stabilisation exercise for 6 weeks in addition to conventional physiotherapy treatment. The exercise was performed in supine position. The sphygmomanometer was used for exercise; the cuff of it was placed sub-occipitally to monitor the flattening of cervical spine that occurs with longus colli’s contraction. Subjects were guided by feedback to sequentially reach 5 mmHg pressure target in 2 mmHg increments from a baseline of 20 mmHg to the final level of 30 mmHg. Subjects were instructed to gently nod their head as though they said ‘yes’. The target pressure that the subject could hold steadily for 10 seconds was identified. The duration of contraction was increased to 10 seconds for each target level. Subjects performed 10 repetitions before progressing to the next target level.
The baseline measurement and measurement at the end of sixth week were compared by using the IBM SPSS 21.0 Multilingual software by analysis of variance.
Statistical Analysis
All statistical analysis was done by using the software package SPSS 21.0 for window version. Mean and standard deviation of all the variables were calculated. The level of significance was set at p<0.05. Analysis of variance was used to compare the pre and post values in both the groups.
Results
This study was done on 20 subjects, 10 in each group. At the beginning of the study, there were no significant differences (p>0.05) between the two groups based on age, BMI or the outcomes measures CVA, PImax, PEmax, NDI, NPRS [Table/Fig-1]. After six weeks between groups comparison showed significant differences (p<0.05). Significant improvement was found in study group (Group B) as compared to control group (Group A) [Table/Fig-2]
Subjects’ baseline characteristics represented as Mean±SD.
| Variables | Control Group (Group A) (n=10) Mean±SD | Study Group (Group B) (n=10) Mean±SD | p-value |
|---|
| Age | 33.60±2.01 | 32.50±1.27 | 0.16NS |
| BMI | 22.20±5.15 | 21.78±3.59 | 0.83NS |
| CVA | 38.56±1.87 | 37.90±1.79 | 1.1NS |
| PImax | 63.33±1.8 | 65.33±1.8 | 0.18NS |
| PEmax | 76.78±1.4 | 77.78±1.4 | 0.39NS |
| NDI | 11.11±1.3 | 12.11±1.2 | 0.18NS |
| NPRS | 7.4±1.2 | 7.6±1.2 | 0.39NS |
p<0.05, NS: Non significant; BMI: Body mass index; CVA: Craniovertebral angle; PImax: Maximum inspiratory pressure; PEmax: Maximum expiratory pressure; NDI: Neck disability index; NPRS: Numeric pain rating scale
Comparison of variables between the Groups.
| Dependent variables | Control Group (Group A) | Study Group (Group B) | Sources | p-value |
|---|
| Mean±SD | Mean±SD |
|---|
| CVA | Pre | 38.56±1.87 | 37.90±1.79 | Group | 0.03* |
| Time | 0.001* |
| Post | 44.5±1.09 | 59.21±1.27 | Interaction (G×T) | 0.001* |
| PImax | Pre | 63.33±1.8 | 65.33±1.8 | Group | 0.01* |
| Time | 0.001* |
| Post | 66±1.6 | 75.01±3.2 | Interaction (G×T) | 0.001* |
| PEmax | Pre | 76.78±1.4 | 77.78±1.4 | Group | 0.04* |
| Time | 0.001* |
| Post | 82.9±3.4 | 87.89±8.9 | Interaction (G×T) | 0.003* |
| NDI | Pre | 11.11±1.3 | 12.11±1.2 | Group | 0.001* |
| Post | 6.67±1.9 | 0.60±0.6 | Time | 0.001* |
| Interaction (G×T) | 0.03* |
| NPRS | Pre | 7.4±1.2 | 7.6±1.2 | Group | 0.001* |
| Post | 4.24±0.44 | 0.90±0.80 | Time | 0.001* |
| Interaction (G×T) | 0.03* |
Data are presented as mean±SD. Results of analysis of 2×2 Mixed design ANOVA. G: represents the main effect of group difference; T: represents main effect of time within subject factors; I: represents (G×T) interactions. *p<0.05 represents significant difference.
BMI: Body mass index; CVA: Craniovertebral angle; PImax: Maximum inspiratory pressure; PEmax: Maximum expiratory pressure; NDI: Neck disability index; NPRS; Numeric pain rating scale
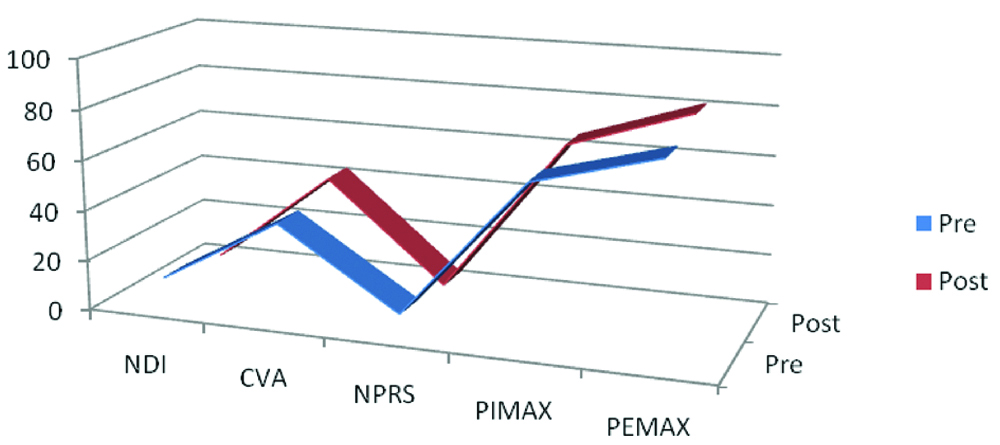
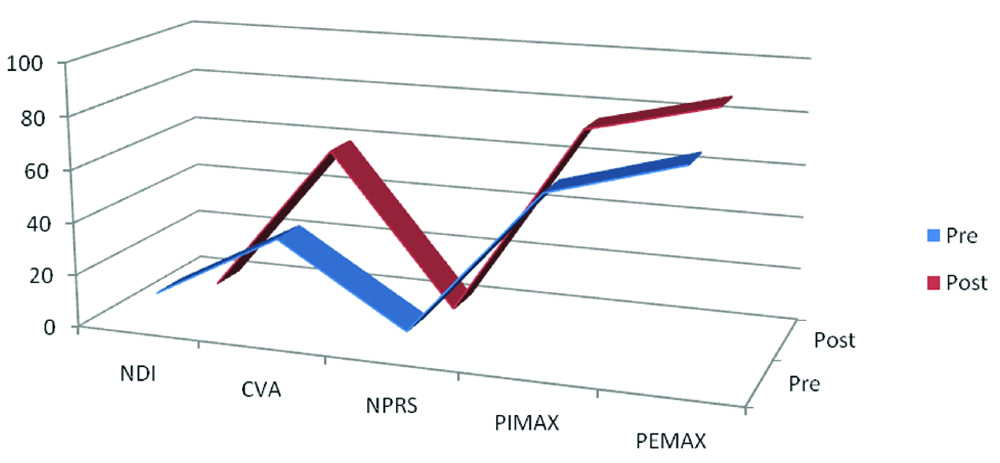
Significant changes occured in outcomes measures NDI, CVA, NPRS, PImax and PEmax from baseline to after sixth weeks in Group A [Table/Fig-3] and in Group B [Table/Fig-4].
Changes in the dependent variables at baseline and after intervention in the Group A.
Changes in the dependent variables at baseline and after intervention in the Group B.
Discussion
This study intended to find the beneficial effects of Cervical Stabilisation exercises along with conventional physiotherapy treatment on the respiratory muscles strength in chronic neck pain patients with forwarding head posture. A forward head posture is one in which the head is positioned anteriorly and the normal anterior cervical convexity is increased with the apex of the lordotic cervical curve at a considerable distance from the line of gravity in comparison with the optimal posture. The anterior slanting of the head caused by forwarding head posture causes abnormal compression on the posterior structures of the spine viz., zygoapophyseal facet joints and intervertebral disks. There is also shortening of zygoapophyseal joint capsule and narrowing of the intervertebral foramina leading to nerve root compression. Muscles of lower cervical spine and upper back are overloaded and continuously work to counterbalance pull of gravity which may cause them to become ischaemic over a period of time in an attempt to counteract the normal external flexion moment. The posterior aspect of the zygoapophyseal joint capsules may become adaptively shortened and the narrowed intervertebral foramen may cause nerve root compression. These all are the potential sources of neck pain in patients with FHP. In addition, in the FHP the scapulae may rotate medially and a thoracic kyphosis may develop and leads to diminished thoracic capacity which causes reduction in vital capacity [14].
It has been found that forward head posture results in reduction of respiratory movements of the lower ribs and alters the biomechanics of breathing and thereby reducing the ventilator efficacy of diaphragm and leads to decrease in strength of the muscles of respiration [15]. Han J et al., in their study found decreased activity of accessory respiratory muscle activity in subjects with forwarding head posture compared to subjects with normal subjects [16]. It is observed that cervical lordosis due to forward head posture affects the vital capacity [17].
Lee K et al., in their study have found that exercises that target to correct the posture and strength of deep neck muscles reduce cervical angle and improves pulmonary function [13]. A Study by Kim SY et al., found that Sustained Natural Apophyseal Glides (SNAGS) to be effective in improving neck posture and pulmonary functions in patients with forwarding head posture [18]. Cervical Stabilisation exercise has been found to control the forward head posture [19].
Dusunceli Y et al., demonstrated the superiority of the neck stabilisation exercises in terms of pain and disability outcomes when compared with isometric and stretching exercises when given with the physical therapy agents for the treatment of neck pain [10]. Study by Akodu AK et al., found neck stabilisation exercises to be effective in reducing neck pain, forward head posture, depression and anxiety in individuals with non-specific chronic neck pain. The mechanism of pain reduction is suggested to be increased activation of motor pathways which suppresses the pain centre in the brain. There was also an improvement in functional status of the patients [20].
In this study, significant improvement has been found in the group who received the Cervical Stabilisation exercise with the conventional physiotherapy program. Results of this study suggested that reduction of forwarding head posture with cervical stabilisation exercises improve the strength of muscles of respiration by correcting the altered biomechanics of cervical and thoracic spine which in turns improve the thoraco-abdominal mobility and efficacy of diaphragm can be improved.
Limitation
The sample size of the study was small and there was no follow-up to check the sustaining effects of cervical stabilisation exercises.
Conclusion
Cervical Stabilisation exercise can be incorporated in the management of patients suffering from FHP to correct the faulty mechanics which leads to impaired respiration.
p<0.05, NS: Non significant; BMI: Body mass index; CVA: Craniovertebral angle; PImax: Maximum inspiratory pressure; PEmax: Maximum expiratory pressure; NDI: Neck disability index; NPRS: Numeric pain rating scale
Data are presented as mean±SD. Results of analysis of 2×2 Mixed design ANOVA. G: represents the main effect of group difference; T: represents main effect of time within subject factors; I: represents (G×T) interactions. *p<0.05 represents significant difference.
BMI: Body mass index; CVA: Craniovertebral angle; PImax: Maximum inspiratory pressure; PEmax: Maximum expiratory pressure; NDI: Neck disability index; NPRS; Numeric pain rating scale
[1]. Jull G, Sterling M, Falla D, Treleaven J, O Leary S, Whiplash, headache and neck pain: research-evidenced directions for physical therapies 2008 ChinaChurchill Livingstone10.1016/B978-0-443-10047-5.50019-9 [Google Scholar] [CrossRef]
[2]. Silva AG, Punt TD, Sharples P, Vilas-Boas JP, Johnson MI, Head posture and neck pain of chronic nontraumatic origin: a comparison between patients and pain-free personsArchives of Physical Medicine and Rehabilitation 2009 90(4):669-74.10.1016/j.apmr.2008.10.01819345785 [Google Scholar] [CrossRef] [PubMed]
[3]. Yip CHT, Chiu TTW, Poon ATK, The relationship between head posture and severity and disability of patients with neck painManual Therapy 2007 :1-7. [Google Scholar]
[4]. Harman K, Kozey CLH, Butler H, Effectiveness of an exercise program to improve forward head posture in normal adults: a randomized, controlled 10-week trialJournal of Manual & Manipulative Therapy 2005 13(14):163-76.10.1179/106698105790824888 [Google Scholar] [CrossRef]
[5]. Kalra S, Pal S, Pawaria S, Correlational study of chronic neck pain and hand grip strength in physiotherapy practitionersInternational Journal of Yoga, Physiotherapy and Physical Education 2017 2(4):30-32. [Google Scholar]
[6]. Kapreli E, Vourazanis E, Strimpakos N, Neck pain causes respiratory dysfunctionMedical Hypotheses 2008 70(5):1009-13.10.1016/j.mehy.2007.07.05017959320 [Google Scholar] [CrossRef] [PubMed]
[7]. Okuro RT, Morcillo AM, Riberio MA, Sakano E, Margosian PB, Ribeiro CJ, Mouth breathing and forward head posture: effects on respiratory biomechanics and exercise capacity in childrenJ Bras Pneumol 2011 37(4):471-79.10.1590/S1806-3713201100040000921881737 [Google Scholar] [CrossRef] [PubMed]
[8]. Lee S-M, Lee C-H, O’Sullivan D, Jung J-H, Park J-J, Effectiveness of an exercise program to improve forward head posture in normal adults: a randomized, controlled 10-week trialThe Journal of Manual & Manipulative Therapy 2005 13(3):163-76.10.1179/106698105790824888 [Google Scholar] [CrossRef]
[9]. Kendall F, Kendall McCreary E, Provance P, Muscles: Testing and Function 1993 4th edBaltimore, MDWilliams & Wilkins [Google Scholar]
[10]. Dusunceli Y, Ozturk C, Atamaz F, Hepguler S, Durmaz B, Efficacy of neck stabilization exercises for neck pain: a randomised controlled trialJ Rehabil Med 2009 41:626-31.10.2340/16501977-039219565156 [Google Scholar] [CrossRef] [PubMed]
[11]. Nam CW, Lee JH, Park YH, Effect of cervical stabilization exercises on the respiratory function of stroke patientsAdvanced Science and Technology Letters (Healthcare and Nursing) 2015 88:196-99.10.14257/astl.2015.88.41 [Google Scholar] [CrossRef]
[12]. Thangavelu K, Moorthy AS, Effect of craniocervical flexor training and cervical flexor training on sitting neck posture in patients with chronic neck pain; comparative studyIndian Journal of Physical Therapy 2014 2(1):66-70. [Google Scholar]
[13]. Lee K, Jung S, Lee Y, Kang KW, Effects of exercise on cervical angle and respiratory function in smartphone usersOsong Public Health Res Perspect 2017 8(4):271-74.10.24171/j.phrp.2017.8.4.0728904850 [Google Scholar] [CrossRef] [PubMed]
[14]. Levangie Pamela K, Norkin CC, Joint Structure and Function: A comprehensive Analysis 2005 4th EditionPhiladelphia, PAF.A. Davis C [Google Scholar]
[15]. Szczygiel E, Weglarz K, Piotrowski K, Mazur T, Metel S, Golec J, Biomechanical influence on head posture and the respiratory movements of the chestActa of Bioengineering and Biomechanics 2015 17(2):143-48. [Google Scholar]
[16]. Han J, Park S, Kim Y, Choi Y, Lyu H, Effects of forward head posture on forced vital capacity and respiratory muscle activityJournal of Physical Therapy Science 2016 28:128-31.10.1589/jpts.28.12826957743 [Google Scholar] [CrossRef] [PubMed]
[17]. Lee Y, Gong W, Kim B, Correlation between cervical lordosis, vital capacity, T-spine ROM and equilibriumJournal of Physical Therapy Science 2011 23:103-05.10.1589/jpts.23.103 [Google Scholar] [CrossRef]
[18]. Kim SY, Kim NS, Kim LJ, Effects of cervical sustained natural apophyseal glide on forward head posture and respiratory functionJ Phys Ther Sci 2015 27:1851-54.10.1589/jpts.27.185126180334 [Google Scholar] [CrossRef] [PubMed]
[19]. Noh HJ, Shim JH, Jeon YJ, Effects of Neck stabilization exercise on neck and shoulder muscle activation in adults with forward head postureInternational Journal of Digital Content Technology and its Applications 2013 7(12):492-98. [Google Scholar]
[20]. Akodu AK, Odunsi FA, Giwa SO, Effects of Neck stabilization exercise on pain, disability, craniovertebral angle and psychological status in patients with non-s[pecific chronic neck painJournal of Riphah College of Rehabilitation Sciences 2018 6(1):10-15. [Google Scholar]