IOP is fluid pressure within the eye exerted on eyeball coats, maintained by the balance between production and drainage of aqueous humour mainly through the trabecular meshwork which ranges from 10-21 mmHg (mean 16±2.5 mm of Hg) [1]. Elevated IOP is the most important risk factor for the optic nerve damage. Certain factors like circadian rhythm, physical activity, body position and Valsalva maneuvers have been shown to alter IOP [2]. There is a peak in IOP levels during early morning and lower levels in IOP during late afternoon with the fluctuation of 4 to 6 mmHg [2]. These variations are due to changes in hormonal control, autonomic nervous system control and muscle tone. Considering all these factors and for better understanding of IOP variations, studies are needed to focus the effect of exercise training on IOP which could have relevance on IOP management for patients with glaucoma. IOP is increased with Bench press exercise [3]. But all forms of aerobic exercises decrease IOP [4]. Isokinetic exercises significantly decrease IOP [5]. Leg press test is an exercise which lowers the IOP [6].
Leg press test is an exercise which is done by pushing a weight or resistance away from participants using their legs with the help of leg press test machine. There is limited relevant data to study the effect of leg press test on IOP [5,6]. Hence, our study hypothesised that leg press test could decrease the IOP. So our objectives were to measure IOP for participants before and after leg press test and to compare the effect of leg press test on IOP before and after leg press test in participants.
Materials and Methods
A cross-sectional study of three months duration from May-July, 2018 after obtaining Institutional Ethical Committee Clearance.
By using G power statistical software with power of 0.85, the sample size was calculated as 102. From the article by Priya R et al., the effect size was 0.3 with combined standard deviation of 1.07 we had used matched pair design by using the G power statistical 3.0 software and we had calculated the sample size [6].
Where, Zα is type I error=1.96; Zβ is Type II Error at 0.15 level=0.84.
Inclusion Criteria
A total of 102 Male volunteers of Melmaruvathur in the age group of 18-27 years with systolic blood pressure ranging from 110-124 mmHg and diastolic blood pressure ranging from 70-82 mmHg without having the habit of smoking, taking alcohol and without any eye infection were included in this study.
Exclusion Criteria
The volunteers having the habit of smoking and taking alcohol, with hypertension, uveitis, acute and chronic conjunctivitis and corneal infection were excluded from this study.
After obtaining informed written consent from the participants, we measured the height, weight and IOP before and immediately after leg press test for the participants by using Schiotz tonometer in Melmaruvathur. To minimize the bias of diurnal variation of IOP, this study was done between 3.30 PM-4.30 PM. Schiotz tonometer (SEJO, Germany) consists of a curved foot plate which was placed on the cornea of a supine participant after sterilisation.
A weighted plunger attached to the footplate sank into the cornea. A scale gave the reading depending on how much the plunger sank into the cornea and a conversion table converted the scale reading into IOP measured in mmHg. Leg press test is a measure of the maximum weight; a participant can lift with one repetition by the legs and also it is a measure of leg strength which varies from person to person [7]. After warm up for 10 minutes, the average of maximum achievable weight for all participants was chosen without prior fatiguing the lower limb muscles. Since the maximum achievable weight for all participants was chosen, the leg press test was done by pushing that weight or resistance away from them using their legs in the leg press test machine in sitting position without locking their knees in a single sitting. Post test values of IOP were measured immediately after leg press test for the participants [6].
Statistical Analysis
These data were entered in an Excel sheet and statistically analysed. IOP measurements before and after leg press test was analysed by mean and standard deviation, paired t-test was used to compare these two measurements.
Results
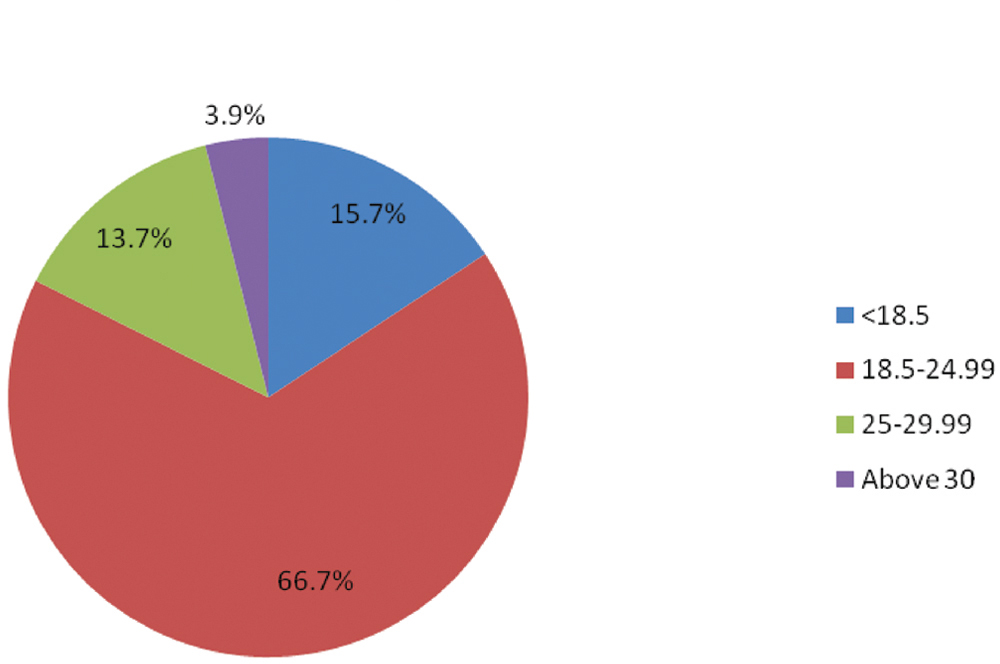
In our study, there were 102 participants of age between 18-27 years with mean age of 20.06±2.26 years and BMI between 15.73-35.51with mean BMI of 22.58±3.96 [Table/Fig-1].
Shows distribution of participants BMI.
Mean IOP of Right eye before leg press test was 16.17±3.08, after leg press test was 11.84±3.11 (Decreased) showing the p<0.001 which is highly significant [Table/Fig-2].
Shows comparison of IOP values before and after leg press test for both eyes.
| Paired t-test Samples Statistics |
|---|
| Mean | Std. Deviation | Std. Error Mean | t-value | p-value |
|---|
| IOP before exercise RT EYE | 16.17 | 3.08 | 0.30 | 11.48 | p<0.001 |
| IOP after exercise RT EYE | 11.84 | 3.11 | 0.31 |
| IOP before exercise LT EYE | 16.92 | 2.64 | 0.26 | 11.71 | p<0.001 |
| IOP after exercise LT EYE | 12.65 | 3.45 | 0.34 |
p<0.001 highly significant
Mean IOP of Left eye before leg press test was 16.92±2.64, after leg press test was 12.65±3.45 (Decreased) showing the p<0.001 which is highly significant [Table/Fig-2].
Discussion
The present study reported the fall in IOP of both eyes after performing leg press test in healthy male volunteers of age between 18-27 years in Melmaruvathur, Tamil Nadu, India. Similar results were obtained in a study conducted by Priya R et al., 2013 which also noted that IOP decreases with leg press test in young adult males of age between 18-22 years in Karnataka [6]. Study by Misra V et al., stated that there was an increase in IOP during premenstrual phase and menstrual phase due to effect of oestrogen [8], Brindha S et al., stated that there was a mild increase in IOP during luteal phase and then study by Ejimadu CS et al., concluded that there was no statistical significant difference in IOP in both genders of mean age 45.83±20.43 years [9,10]. Because of conflicting reports from these studies, we considered to include only young males as participants. There are studies which agree dynamic exercises decrease IOP [11], acute dynamic exercises decrease IOP in sedentary women but not in male athletes [12] and also shows the association between BMI and decrease in IOP [13]. There are a variety of physiological variations in IOP from decreased levels to increased levels which has been associated with day to day activities [14].
The reduction of IOP levels is correlated with increased aqueous humour drainage than production especially after an exercise with consequent hyperventilation leading to decreased venous pressure thereby decreased IOP [15]. The extent of reduction of IOP depends upon the intensity and duration of exercise and also the time of measurement of IOP [4]. Even though the responsible physiological mechanism for these changes of IOP is not yet understood, there is strong evidence that regularly performing certain physical activity for many years can reduce IOP [15].
The probable mechanism of decreased IOP levels after leg press test could be increased ocular sympathetic activity which facilitates increased aqueous drainage; activation of C-AMP favours decreased production of aqueous humour; decreased blood pH: increased plasma lactate levels which favours outflow of water from eye [4,6].
Limitation
Females were not included in this study as participants because of many conflicting reports from various studies [8-10] regarding the relationship between the hormonal status and IOP changes. So, to study the correlation between IOP and leg press test in young adult females needs larger group of subjects and continuous monitoring of IOP during different phases of menstruation with measurement of hormones during all phases of menstruation.
Conclusion
Leg press test is an isokinetic exercise which lowers IOP in young healthy males. Further studies are needed to extrapolate the association between IOP in glaucomatous patients and leg press test.
p<0.001 highly significant