Immunoglobulin Light-Chain Isotype Switch (IS) during Lenalidomide Therapy in Multiple Myeloma and its Association with Increased M Protein Production and Miliary TB
Ashok Kumar Kapoor1, Supriya Mehrotra2, Rajesh Kumar Srivastava3
1 Pathologist, Department of Pathology, RML Mehrotra Pathology Pvt. Ltd, Nirala Nagar, Lucknow, Uttar Pradesh, India.
2 Pathologist, Department of Pathology, RML Mehrotra Pathology Pvt. Ltd, Nirala Nagar, Lucknow, Uttar Pradesh, India.
3 Senior Technologist, Department of Pathology, RML Mehrotra Pathology Pvt. Ltd, Nirala Nagar, Lucknow, Uttar Pradesh, India.
NAME, ADDRESS, E-MAIL ID OF THE CORRESPONDING AUTHOR: Ashok Kumar Kapoor, Pathologist, Department of Pathology, RML Mehrotra Pathology Pvt. Limited, B-171, Nirala Nagar, Lucknow-226020, Uttar Pradesh, India.
E-mail: drashokkapoor2016@gmail.com
Multiple Myeloma (MM) is a malignant neoplasm arising from a single plasma cell clone. It mainly affects older people. It forms localised osteolytic lesions. It secretes a single monoclonal immunoglobulin of constant isotype with light-chain restriction (paraprotein). MM cells may express, an adhesion molecule. This molecule is not present on normal plasma cell. In addition, immunoglobulin light-chain may be detected in urine (Bence jones proteins). Rarely, one of the isotypes may switch to another type during high-dose chemotherapy. In addition, Isotype Switch (IS) may occur spontaneously without any treatment. The present case relates about an 87-year-old man who complained of pain in dorsal thoracic region. X-ray examination showed fractures of thoracic vertebra eighth to tenth. Sternal puncture was done. Bone marrow examination showed large number of plasmacytoid cells. Moreover, serum protein electrophoresis revealed moderately raised M band proteins in gamma globulin region (M band protein concentration was 2.03 gm/dL). The patient was diagnosed as a case of MM. Initially, he was treated with Thalidomide 100 mg daily for one month. Later, he was treated with Lenalidomide 10 mg daily for 30 days followed by a drug-free period of 15 days. After eight cycles of Lenalidomide therapy light-chain IS was detected. Initially, tumour produced lambda (λ) light-chain for one year as seen in first, second and third serum specimens. Later, light-chain switch was detected in fourth serum specimen from lambda (λ) to kappa (k) light-chain. IS was accompanied with high level of M band proteins (5.4 gm/dL). In addition, the patient developed Miliary Tuberculosis. Subsequently, the patient was treated with Phaglomide (Pomalidomide) instead of Lenalidomide.
CD56, Kappa light-chain, Plasmacytoma lambda light-chain
Case Report
An 87-year-old man complained of pain dorsal thoracic region. X-ray chest revealed fractures of eighth to tenth thoracic vertebra. Sternal puncture was also done and bone marrow was aspirated. Microscopic examination showed large number of plasmacytoid cells. Serum Protein Electrophoresis (PE) and Immunofixation Electrophoresis (IFE) showed M band consisting of immunoglobulin light-chain λ in the first specimen [Table/Fig-1a,e]. Similar M protein spikes with lower levels were also seen in second [Table/Fig-1b,f] and third specimens [Table/Fig-1c,g]. The patient was diagnosed as a case of MM. Initially, he was treated with thalidomide 100 mg daily for a month. Later, he was treated with Lenalidomide 10 mg every 24 hours for 30 days. After a drug-free period of 15 days, Lenalidomide was again repeated for 30 days followed by drug-free period of 15 days. Thus, eight cycles of Lenalidomide treatment were given. Serum protein electrophoresis and IFE were repeated after every six months for one and a half years. Immunoglobulin class and light-chains were determined using Helena Bioscience electrophoresis system. Briefly, serum proteins were separated in agarose gel by electrophoresis at alkaline pH. Anti-human Serum Proteins (SP), anti-human IgG (G), anti-human IgA (A), anti-human IgM (M), anti-human kappa (k) and anti-human lambda (λ) were applied separately in different lanes as shown in lower half of [Table/Fig-1]. Immune complexes were identified after staining of precipitated antigen-antibody complexes. Serum IFE revealed production of kappa light-chain (k) instead of lambda light-chain (λ) in fourth serum specimen [Table/Fig-1h].
Upper half of figure shows results of serum protein electrophoresis with four different serum specimens of a MM patient. M peak was seen in all the specimens; a) shows moderate peak of M proteins (concentration of M proteins was 2.03 gm/dL); b and c) show fall in M protein levels following Lenalidomide therapy; d) shows extremely high level of M proteins (5.4 gm/dL) due to development of Lenalidomide-resistance. Lower half of figure shows results of serum immunofixation electrophoresis with different antisera. Total serum proteins have been electrophoresed and precipitated onto agarose gel in lanes e to h). Lambda (λ) paraprotein is seen in e to g). On the contrary, prominent Kappa (k) paraprotein was seen in h). Fourth specimen showed IgG- kparaprotein (red arrow).
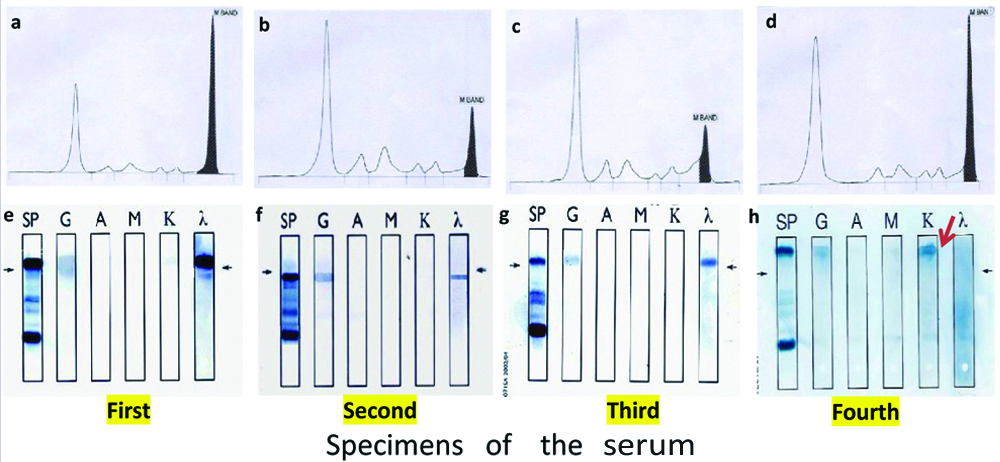
Initially, the patient favorably responded to Lenalidomide therapy for 11 months. In first specimen (starter) serum M band concentration (2.03 gm/dL) was moderately raised [Table/Fig-1a]. Later, it dropped to 0.98 gm/dL and 0.91 gm/dL in second and third specimens [Table/Fig-1b,c]. The patient was producing λ light-chains throughout during one year [Table/Fig-1]. Subsequently, after one and a half years of treatment in fourth serum specimen, M band concentration was found to be increased to extremely high level (5.04 gm/dL), suggesting development of Lenalidomide-resistance [Table/Fig-1d]. However, fourth serum specimen showed production of k light-chains instead of λ light-chains. Findings were suggestive of IS from λ to k light-chains due to Lenalidomide therapy. After one and a half years of Lenalidomide treatment, he developed fever and millet-like lesions in X-ray lungs (miliary TB), for which he was given ATT. Later, he was treated with Phaglomide (Pomalidomide) instead of Lenalidomide. At this time, he was producing k light chains. Phaglomide was given because the patient developed Lenalidomide-resistance. The patient could not be followed further.
Discussion
Multiple Myeloma is usually characterised by production of a single monoclonal immunoglobulin (Ig) protein with constant heavy-chain isotype and light-chain restriction. Rarely, multiple isotype switches may develop in untreated MM patients. However, more commonly these switches develop in treated MM patients. The abnormal protein bands may develop due to altered paraprotein production by malignant plasma cell clone or it may be due to recovery of B-cell function following myeloablative treatment [1]. Another case of myeloma has been reported in a women who initially presented with a non-secretory MM. Eleven months later it switched to IgD secreting λ type myeloma following velcade plus dexamethasone treatment. Current case produced λ light-chains during first year of Lenalidomide therapy. Another interesting feature of current case was biochemical and clinical deterioration of the patient following long-term Lenalidomide therapy lasting for a year. After one and a half year of treatment, M band concentration suddenly increased to extremely high level is fourth specimen (serum M band protein concentration was 5.4 gm/dL). This observation suggested increased proliferation of plasmacytoid cells, resulting in increased production of M band proteins. In addition, it suggested development of Lenalidomide-resistance. Therefore, Lenolidomide was replaced by Phaglomide (Pomalidomide). At this stage of illness, the patient’s general condition also deteriorated and he developed miliary tuberculosis. Therefore, he was treated with anti-tuberculous drugs. In the present case, Ig isotype light-chain switch occurred following Lenalidomide therapy alone. There was no history of bone marrow and/or stem cell transplantation in our patient. Conversely, in earlier studies [1,2] high-dose myeloablative therapy was given along with bone marrow/or stem cell transplantation. These drugs (Lenolidomide and Pomalidomide) are derived from basic drug structure of Thalidomide with similar properties. For example, these drugs are immunomodulators, affect both T-cell mediated and antibody mediated responses [3,4]. In addition, these drugs have anti-angiogenic anti-inflammatory properties. Anti-inflammatory effect of these drugs in erythema nodosum leprosum appeared to be through suppression of mycobacterial hypersensitivity. Anti-cancer property of these drugs may be operative along with suppression of mycobacterial immunity resulting in reactivation of primary complex in present case.
Conclusion
Light chain isotype switch from λ to k chain may occur following treatment. However, it occurs rarely. Immunoglobulin light-chain switch in MM was associated with Lenalidomide-resistance and extreme rise in level of M band proteins. In addition, Lenalidomide resistance resulted in reactivation of Mycobacterium tuberculosis and its widespread haematogenous dissemination. Interrupted low-dose Lenalidomide-therapy resulted in Ig isotype light-chain switch in present patient.
[1]. Zent CS, Wilson CS, Tricot G, Jagannath S, Siegel D, Desikan KR, Oligoclonal protein bands and Ig isotype switching in multiple myeloma treated with high-dose therapy and hematopoietic cell transplantationBlood 1998 91:3518-23. [Google Scholar]
[2]. Ham JY, Lee KM, Song KE, Immunoglobulin isotype switching in a plasma cell myeloma patient treated with high-dose chemotherapy and hemopoietic stem cell transplantationLaboratory Medicine online 2011 1(3):158-62.10.3343/lmo.2011.1.3.6 [Google Scholar] [CrossRef]
[3]. Kotla V, Goel S, Nischal S, Heuck C, Vivek K, Das B, Machanism of action of lenalidomide in hematological malignanciesJ Hematol Oncol 2009 2:3610.1186/1756-8722-2-3619674465 [Google Scholar] [CrossRef] [PubMed]
[4]. Gao L, Li Q, Kang J, Li C, Zhou J, Non-secretory multiple myeloma switches to IgD of lambda type; a case report and review of literatureIntJ ClinExp Med 2015 8(9):16984-90. [Google Scholar]